Page 9 of 17
FM8.11 | Impotence, Sterility & Sexual Dysfunction — SDL Guide
Learning Objectives
- Define impotence, sterility, frigidity, and sexual dysfunction and distinguish between them
- Classify the causes of impotence in males and females
- State the medicolegal contexts in which impotence, sterility, and sexual dysfunction are relevant
- Explain premature ejaculation and its medicolegal significance
- Describe how the doctor formulates a medico-legal opinion in cases involving these conditions
INSTRUCTIONS
Impotence and sterility are among the grounds on which marriages are challenged, criminal defences are mounted, and civil claims are filed in Indian courts. The doctor who can clearly define these terms, classify their causes, and explain the limitations of clinical assessment serves the court's fact-finding function effectively. These are conditions that overlap clinical medicine, psychiatry, and forensic medicine — approached with clinical objectivity and appropriate sensitivity.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A couple presents to court for divorce proceedings. The husband claims the marriage has not been consummated because he has been impotent since the wedding day. The wife's lawyer requests a medical examination of the husband to determine whether he is impotent. A separate case involves a man accused of rape who claims his defence is absolute impotence — he is physically incapable of performing the act. In both scenarios, the court needs a medico-legal expert's opinion. What can clinical examination actually establish, and what are its limits?
WHY THIS MATTERS
Impotence and sterility have practical medicolegal significance in three domains: matrimonial law (nullity of marriage, divorce, maintenance), criminal law (defence to charges of rape or sexual assault), and succession and legitimacy (establishing inability to father a child). The clinician must be able to assess these conditions rigorously, communicate their findings with appropriate certainty, and recognise that impotence as a complete defence to a rape charge requires both a convincing clinical picture and corroborative evidence — courts have historically been sceptical of convenient claims of impotence by accused persons.
RECALL
From Year-1 physiology: the male sexual response cycle involves libido (desire), penile erection (primarily a vascular/neurological event mediated by NO/cGMP pathway), ejaculation (sympathetically mediated), and orgasm. Female sexual response involves arousal (vaginal lubrication via parasympathetic transudation), clitoral engorgement, and orgasm. From pharmacology: PDE5 inhibitors (sildenafil) act on the erection mechanism; their existence implies the mechanism is biochemically targetable. Both conditions involve interaction between organic (vascular, neurological, hormonal, anatomical) and psychogenic factors.
Definitions: Impotence, Sterility, Frigidity, Sexual Dysfunction
Precise terminology is critical in medico-legal reporting because courts act on exactly what the doctor states.
Impotence (erectile dysfunction in contemporary clinical terminology) refers to the inability of a male to achieve or maintain a penile erection sufficient for penetrative sexual intercourse. Note: this definition is specific to the physical act of penetration. A man who can achieve erection but cannot sustain it, or who can achieve erection in some circumstances but not others (situational impotence), is not absolutely impotent. The distinction matters in medico-legal practice because only absolute, persistent impotence can serve as a defence to rape.
Sterility (infertility) refers to the inability to produce a pregnancy — in males, through failure to produce viable spermatozoa in adequate quantity (azoospermia or severe oligospermia); in females, through failure of ovulation, implantation, or other reproductive processes. Sterility does not imply impotence: a man may be able to perform sexual intercourse normally but be azoospermic. Sterility is relevant to legitimacy disputes and succession.
Frigidity is an older clinical term (largely superseded in modern medicine) referring to the absence or impairment of sexual desire or arousal in women. The equivalent contemporary terminology is female sexual interest/arousal disorder (FSIAD in DSM-5). Medicolegally, frigidity is relevant in matrimonial cases (non-consummation) and occasionally in cases where a female accused claims she was too inhibited to resist assault (a complex and legally sensitive assessment).
Sexual dysfunction is the broader term encompassing any clinically significant impairment of sexual desire, arousal, orgasm, or the physical mechanics of intercourse in either sex. It includes: erectile dysfunction (ED), premature ejaculation, delayed ejaculation, dyspareunia (painful intercourse, in either sex), vaginismus (involuntary vaginal muscle spasm preventing penetration), and disorders of desire/arousal/orgasm.
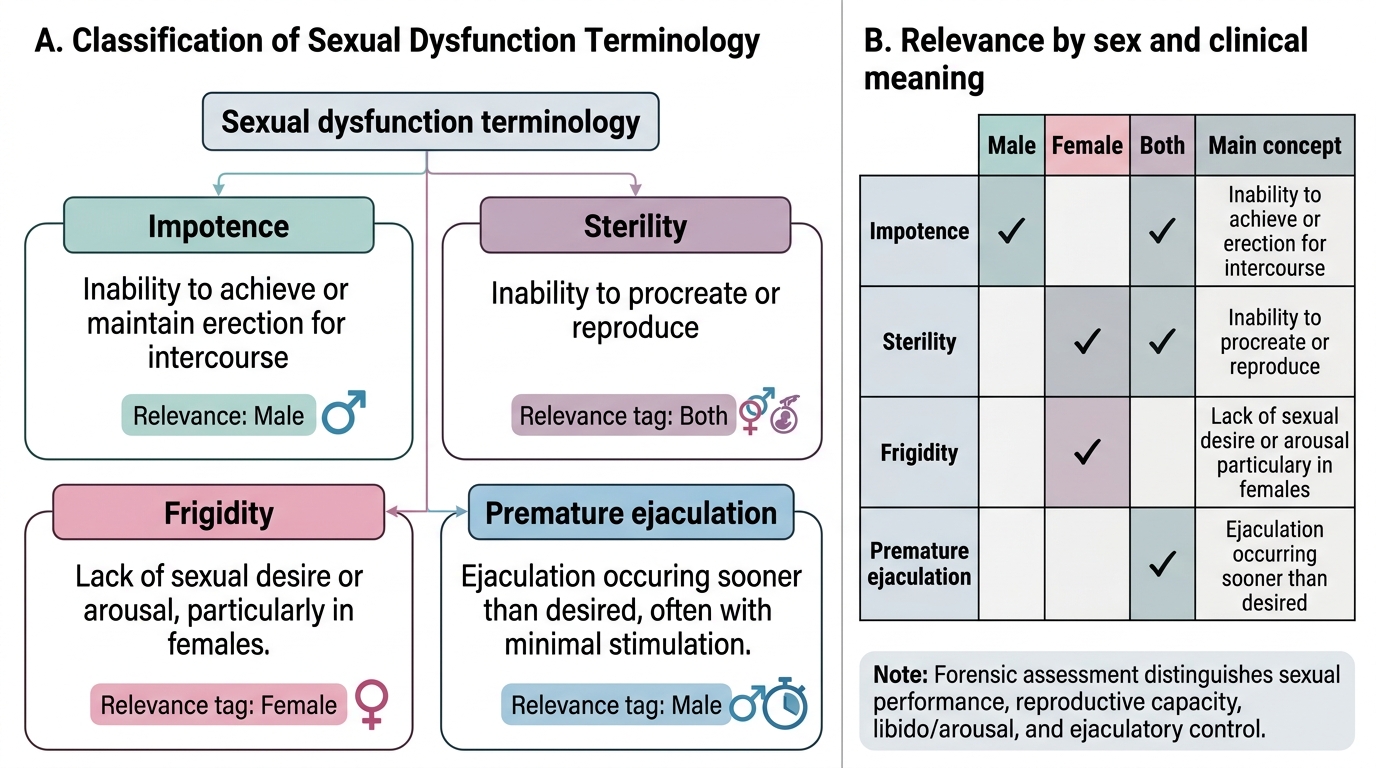
Classification of Sexual Dysfunction Terminology
Causes of Impotence in Males and Females
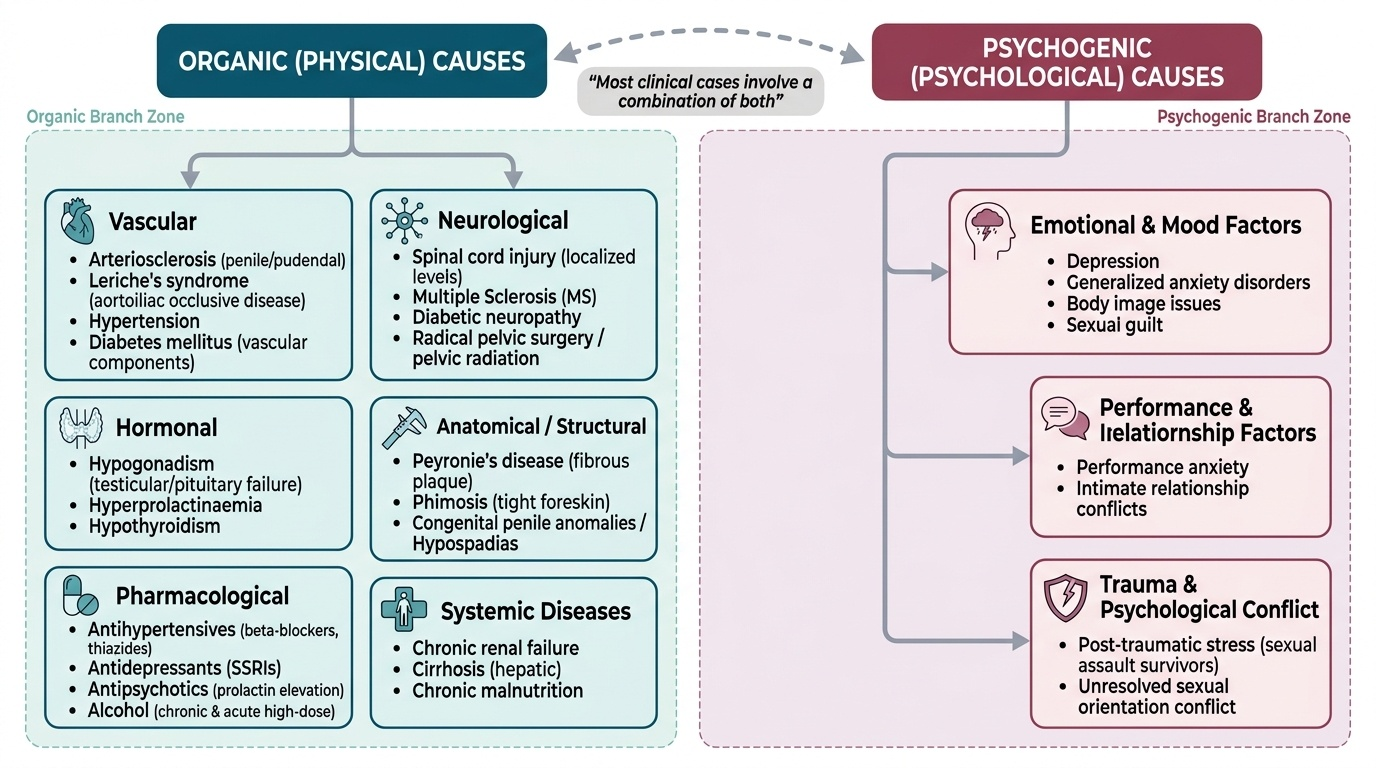
Impotence and sexual dysfunction may be organic (physical) or psychogenic in origin, and most cases in clinical practice involve a combination of both. The forensic clinician must assess both categories.
Organic causes in males:
- Vascular: Arteriosclerosis of penile/pudendal arteries, Leriche's syndrome (aortoiliac occlusive disease), hypertension, diabetes mellitus (autonomic neuropathy + vascular disease)
- Neurological: Spinal cord injury (above T12-L1 for psychogenic erections; above S2-4 for reflex erections), multiple sclerosis, diabetic neuropathy, radical pelvic surgery (prostatectomy, APR), pelvic radiation
- Hormonal: Hypogonadism (primary — testicular failure; secondary — pituitary-hypothalamic failure), hyperprolactinaemia, hypothyroidism
- Anatomical/structural: Peyronie's disease (fibrous plaque causing penile curvature), phimosis (tight foreskin preventing penetration), congenital penile anomalies, hypospadias
- Pharmacological: Antihypertensives (especially thiazides, beta-blockers, methyldopa), antidepressants (SSRIs — delay ejaculation, reduce libido), antipsychotics (via hyperprolactinaemia), alcohol (chronic — reduces testosterone; acute high doses impair erection)
- Systemic disease: Chronic renal failure, cirrhosis, malnutrition
Organic causes in females:
- Atrophic vaginitis (postmenopausal oestrogen deficiency — causes dyspareunia)
- Vaginismus (involuntary levator ani spasm — may prevent penetration)
- Pelvic inflammatory disease (PID), endometriosis (causes dyspareunia)
- Neurological conditions (multiple sclerosis, spinal cord injury)
- Hormonal (postpartum, hypothyroidism, hyperprolactinaemia)
- Genital anomalies (vaginal atresia, imperforate hymen, vaginal septum)
Psychogenic causes (both sexes): Performance anxiety, relationship conflict, depression, anxiety disorders, post-traumatic stress (sexual assault survivors), body image issues, sexual guilt, and unresolved sexual orientation conflict.
Provided image
SELF-CHECK
A 45-year-old diabetic man with hypertension reports erectile dysfunction. A semen analysis shows azoospermia. Which pair of conditions does he have?
A. Impotence and frigidity
B. Impotence and sterility — these are independent conditions; the diabetic neuropathy/vasculopathy causes erectile dysfunction, while azoospermia constitutes sterility
C. Impotence only — sterility is a consequence of impotence
D. Sterility only — erectile dysfunction is a symptom of sterility
Reveal Answer
Answer: B. Impotence and sterility — these are independent conditions; the diabetic neuropathy/vasculopathy causes erectile dysfunction, while azoospermia constitutes sterility
Impotence (erectile dysfunction) and sterility (azoospermia) are independent conditions. Diabetes mellitus causes erectile dysfunction via autonomic neuropathy and vascular disease, AND may cause testicular dysfunction leading to azoospermia — but through different pathways. A man can be impotent and fertile, impotent and sterile, or potent and sterile.
Premature Ejaculation: Definition and Medicolegal Significance
Premature ejaculation (PE) is defined as ejaculation that occurs within approximately 1 minute of vaginal penetration (or before penetration in severe cases) on a persistent basis, causing personal distress. It is the most common male sexual dysfunction, affecting approximately 20-30% of men at some point. DSM-5 requires the symptom to be present for ≥6 months in approximately 75-100% of sexual encounters.
The medicolegal significance of premature ejaculation is important in two specific contexts:
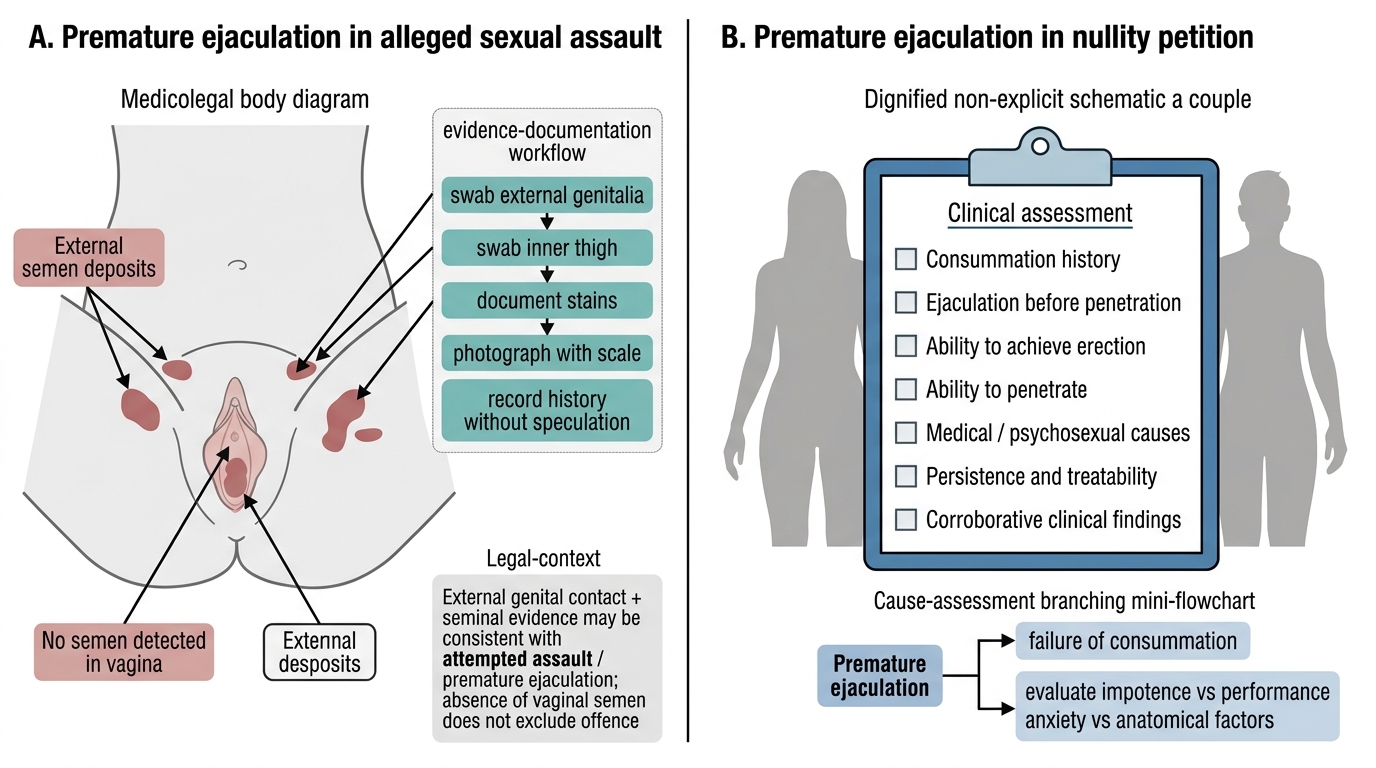
First, in rape cases: a man with premature ejaculation who ejaculates before or immediately on attempted penetration may deposit seminal fluid on the external genitalia or thighs without achieving vaginal penetration. This has been raised as a defence ('no penetration occurred') but also as evidence that a sexual act was attempted. The forensic implication: presence of spermatozoa on the external genitalia, thighs, or perianal area does not exclude sexual assault even without vaginal penetration evidence; BNS Section 63's act definition now encompasses genital apposition and external ejaculation as potentially criminal acts.
Second, in matrimonial cases (non-consummation): PE may result in non-consummation if penetration never occurs. The doctor assessing non-consummation must determine whether PE (or vaginismus, or impotence) is the cause, as this affects the legal ground cited for nullity or divorce.
Medicolegal Significance of Premature Ejaculation
SELF-CHECK
A woman reports rape; semen is found on her inner thigh and vulva but not in the vagina. The accused claims impotence and inability to penetrate. Which of the following statements is most accurate?
A. Absence of vaginal semen is proof of innocence
B. The presence of external semen is consistent with premature ejaculation during an assault attempt; BNS Section 63 acts can include external contact
C. This evidence is irrelevant to the rape charge
D. Impotence conclusively establishes a defence to any sexual assault charge
Reveal Answer
Answer: B. The presence of external semen is consistent with premature ejaculation during an assault attempt; BNS Section 63 acts can include external contact
BNS Section 63's expanded act definition encompasses sexual acts beyond vaginal penetration. Semen on the external genitalia is consistent with premature ejaculation during a sexual assault attempt. Impotence as a complete defence requires demonstrating that any physical sexual act — not merely vaginal penetration — was impossible, which is an extremely high bar.
Medicolegal Assessment and Opinion
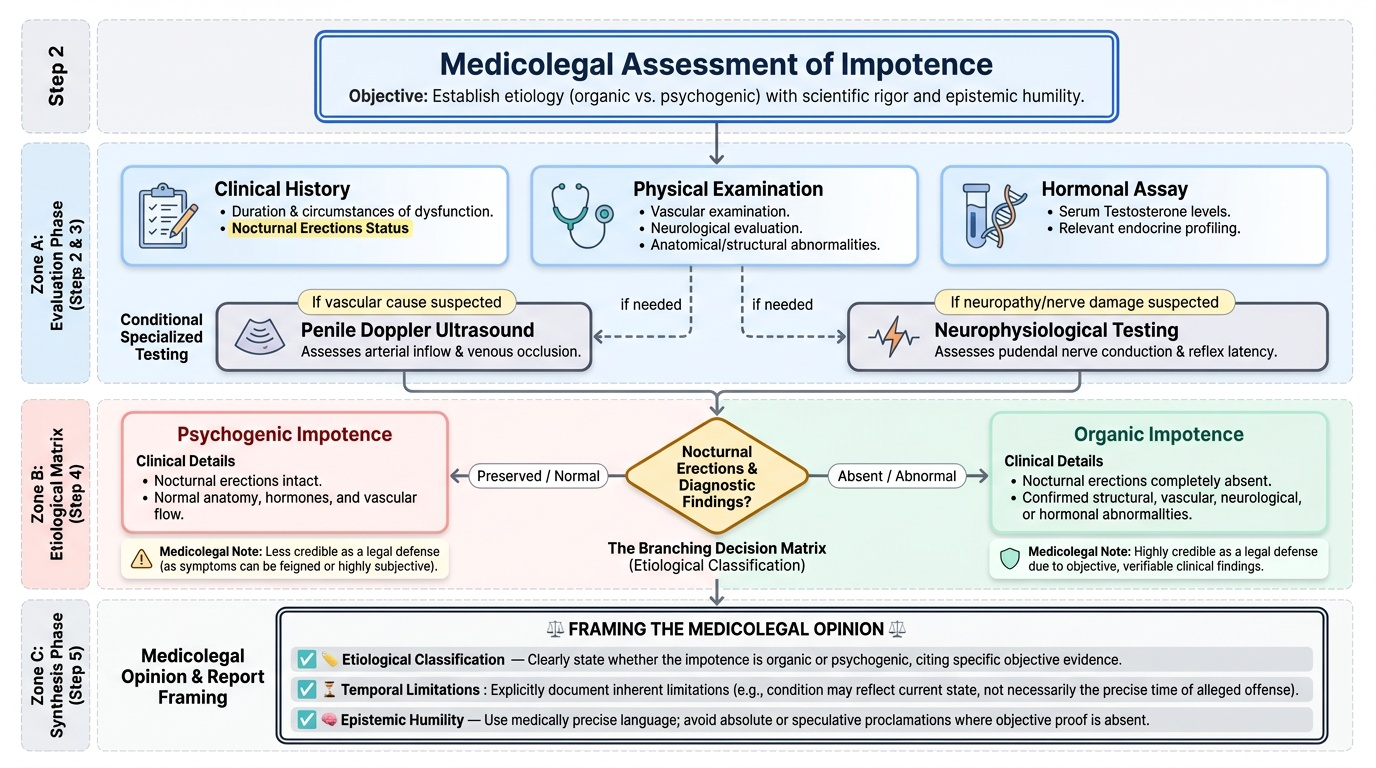
When asked to provide a medico-legal opinion on impotence or sterility, the clinician must conduct a structured assessment and frame the report with appropriate precision and epistemic humility.
The assessment of impotence includes: complete sexual and medical history (duration, circumstances, presence of nocturnal erections — nocturnal erections preserved suggests psychogenic cause; absent nocturnal erections suggest organic cause); examination for vascular, neurological, and anatomical abnormalities; testosterone and relevant hormonal assay; penile Doppler ultrasound if vascular cause suspected; and neurophysiological testing if neuropathy suspected.
The assessment of sterility in males is primarily by semen analysis: volume, sperm count (normal ≥15 million/mL), morphology (≥4% normal forms by Kruger strict criteria), motility (total motility ≥40%). Azoospermia is confirmed on two samples. Where azoospermia is confirmed, testicular biopsy distinguishes obstructive (normal spermatogenesis, blocked vas) from non-obstructive (spermatogenesis failure) — relevant to the fertility treatment but also to the legal outcome.
In forming the medico-legal opinion, the doctor must state:
(1) Whether impotence is organic or psychogenic — organic impotence with preserved nocturnal erections absent, structural abnormality confirmed, or hormonal basis established is more credible as a defence than purely psychogenic impotence.
(2) Whether sterility is present — and if so, its likely duration (was it present at the time in question?).
(3) The limitations of the assessment — impotence can be feigned; semen analysis reflects the current state, not necessarily what existed at the time of the alleged offence.
Key principle: courts in India have historically been cautious about accepting impotence as a complete defence to rape, particularly where psychogenic impotence is alleged — because psychogenic impotence by definition can be overcome in a high-arousal state (including during sexual violence). The doctor must present the evidence, state its limitations, and leave the legal inference to the court.
Provided image
CLINICAL PEARL
Absolute organic impotence (no erection possible under any circumstances) is rare. Psychogenic impotence is far more common and can be overcome in specific circumstances. When an accused person claims impotence as a defence to rape, the medicolegal assessment must specifically address: are nocturnal erections preserved? Is there any history of successful intercourse? Is the clinical picture truly absolute? A man with psychogenic impotence who achieves erection in most situations but claims he was impotent on the night in question is not providing an absolute defence.
SELF-CHECK
A man accused of rape claims impotence. On assessment, nocturnal erections are preserved and there is no organic cause identified. How does this affect the medico-legal opinion?
A. Confirms his defence — any form of impotence is a complete defence to rape
B. Suggests psychogenic impotence; this does not provide an absolute defence, as psychogenic impotence can be overcome in high-arousal states
C. Is irrelevant — only laboratory testing, not clinical history, can establish impotence
D. Rules out organic impotence but cannot be commented on in the medico-legal report
Reveal Answer
Answer: B. Suggests psychogenic impotence; this does not provide an absolute defence, as psychogenic impotence can be overcome in high-arousal states
Preserved nocturnal erections indicate intact physiological erectile mechanism, suggesting psychogenic causation. Psychogenic impotence does not constitute an absolute defence to rape because it may not prevent erection in all circumstances, including during a sexual assault. The doctor must clearly state this distinction in the report.
KEY TAKEAWAYS
Impotence (erectile dysfunction) is inability to achieve/maintain erection for penetration; sterility is inability to produce a pregnancy; frigidity/FSIAD is female sexual interest/arousal disorder; sexual dysfunction is the umbrella term. Causes of male impotence: vascular (diabetes, arteriosclerosis), neurological (spinal cord injury, neuropathy), hormonal (hypogonadism, hyperprolactinaemia), structural (Peyronie's disease, phimosis), pharmacological, and psychogenic. Female causes include atrophic vaginitis, vaginismus, PID, and neurological/hormonal causes. Premature ejaculation has medicolegal significance in rape cases (external deposition without penetration) and matrimonial cases (non-consummation). Impotence claims as criminal defence must distinguish organic from psychogenic; nocturnal erections preserved = psychogenic = does not constitute an absolute defence.
REFLECT
A 38-year-old man is accused of rape. His defence team presents you with a urologist's report saying he has 'erectile dysfunction.' You are instructed to comment on the validity of this as a defence. What additional information would you require? What is the critical clinical distinction that determines whether this can serve as an absolute defence? How would you frame your opinion for the court?