Page 10 of 33
FM13.14,FM14.15 | Alcohols, Hooch & Drunkenness Examination — SDL Guide
Learning Objectives
- Describe the toxicokinetics of ethanol, methanol, and ethylene glycol, including their metabolic pathways and mechanisms of toxicity
- Explain the chemistry and public-health significance of hooch (illicit liquor) tragedies in India
- Conduct a systematic clinical examination of an intoxicated person (Section 185 MV Act request) and prepare a medicolegal report
- Apply the Widmark formula to calculate blood alcohol concentration
- Identify the specific antidotes for methanol and ethylene glycol poisoning
INSTRUCTIONS
Alcohol-related medicolegal work is among the most common tasks a forensic medicine specialist performs — from examining a person alleged to be drunk driving, to certifying the cause of death in hooch tragedy victims, to assessing the contribution of alcohol intoxication to a criminal act. This SDL integrates the chemistry of alcohols, their forensic pharmacology, and the statutory framework for drunkenness examination into a single coherent skill set.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At 11 pm on a Saturday, a traffic police officer brings a 35-year-old man to the hospital casualty. The officer says the man was driving erratically and was pulled over. The officer formally requests a medical examination under Section 185 of the Motor Vehicles Act and hands you a standard form. The man is cooperative, walks with a slight stagger, smells of alcohol, and answers questions appropriately though with slightly slurred speech. His eyes are a little bloodshot. He insists he only had 'two beers'. You have 30 minutes to examine him and produce a medicolegal report that will be submitted to the traffic magistrate. What exactly do you look for, and what does Indian law say about the blood alcohol threshold for impairment?
WHY THIS MATTERS
Alcohol-related medicolegal work in India is vast in scope. The Motor Vehicles Act makes drunken driving a specific offence with a defined BAC threshold, and police regularly bring alleged drunk drivers for medical examination. Beyond driving, alcohol intoxication is relevant to criminal law (diminished responsibility), civil law (contract validity while intoxicated), and public health (hooch tragedies — periodic mass-casualty events from methanol-contaminated illicit liquor). Methanol and ethylene glycol poisoning, while less common, are potentially fatal industrial accidents and occasional criminal poisonings. Mastering alcohol forensics — the chemistry, the pharmacology, and the medicolegal procedure — is indispensable for every doctor in clinical and forensic practice.
RECALL
Activate your Year-1 knowledge:
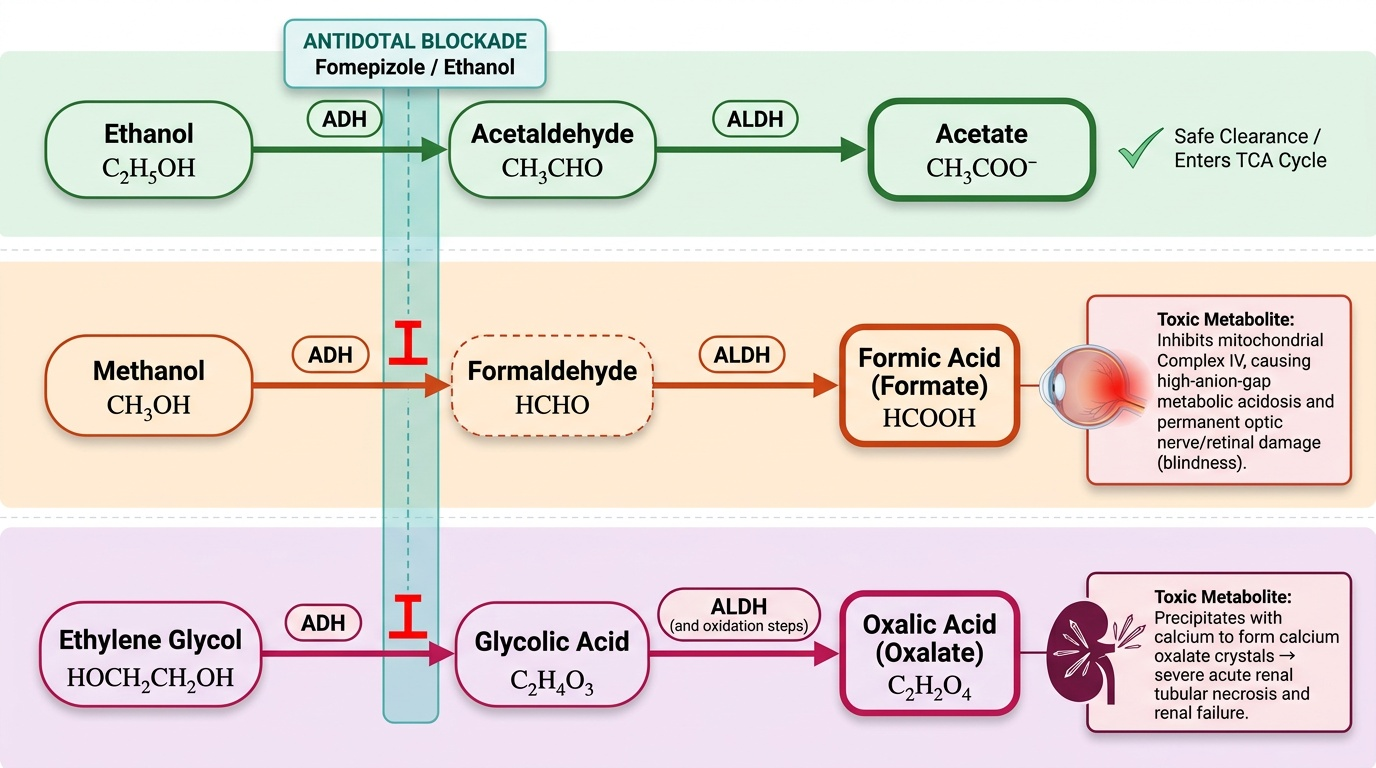
- Biochemistry: alcohol metabolism — ethanol → acetaldehyde (by alcohol dehydrogenase, ADH) → acetate (by aldehyde dehydrogenase, ALDH) → acetyl-CoA → TCA cycle. This is the normal pathway; disulfiram blocks ALDH, causing acetaldehyde accumulation → flushing, nausea, headache.
- Physiology: CNS depressant effects — alcohol enhances GABA (inhibitory) receptor function and inhibits NMDA (excitatory) receptors → dose-dependent CNS depression.
- Biochemistry: methanol vs ethanol — both are substrates for ADH, but methanol's product is formaldehyde → formic acid (not the same as ethanol's acetaldehyde pathway); formic acid is the toxic metabolite that damages the optic nerve.
- Pharmacokinetics: zero-order kinetics — ethanol is metabolised at a constant rate (approximately 10–15 mg/100 mL/hour) regardless of concentration, because ADH becomes saturated at relatively low concentrations.
Legal and Professional Context: Drunkenness Examination
The forensic examination of an intoxicated person is a well-defined statutory procedure in India. Understanding the legal basis before you examine a single patient is essential — the medicolegal report you produce is a legal document that will be presented in court, and your examination must follow the prescribed procedure or it will be challenged.
Statutory framework:
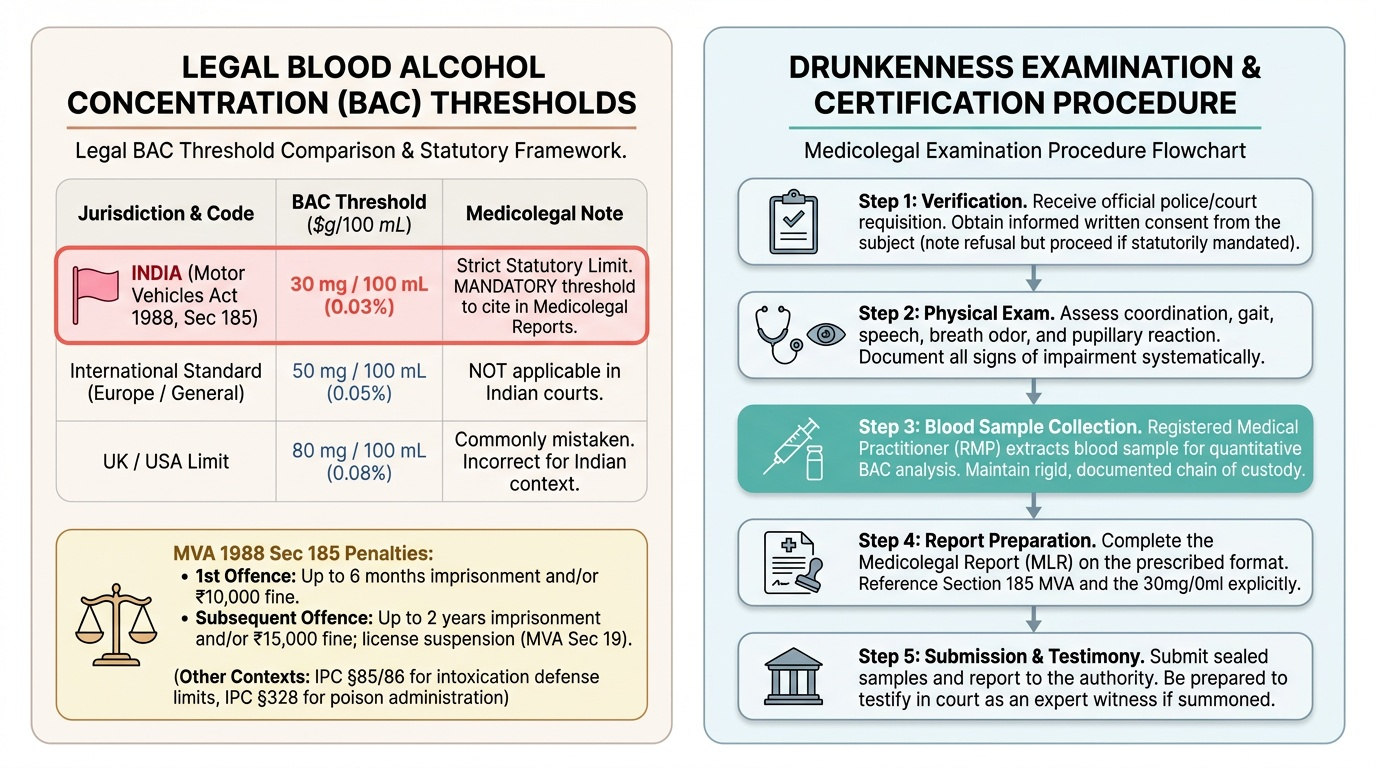
Motor Vehicles Act (MVA) 1988, Section 185: Driving or attempting to drive a motor vehicle while under the influence of alcohol or drugs is an offence. The act defines the legal threshold for impairment by alcohol in India as:
- Blood Alcohol Concentration (BAC): 30 mg per 100 mL of blood (0.03 g/100 mL = 0.03%)
This is the Indian legal limit — NOT 0.08% (the UK/USA limit) and NOT 0.05%. Any answer suggesting a higher threshold (such as 0.08%) is incorrect in the Indian context. Every medicolegal report citing BAC must reference 30 mg/100 mL as the legal threshold under MVA Section 185.
Penalties: first offence — imprisonment up to 6 months and/or fine ₹10,000; subsequent offence — imprisonment up to 2 years and/or fine ₹15,000. Additionally, the licence may be suspended under MVA Section 19.
The doctor's duty in drunkenness examination:
- Examination must be by a registered medical practitioner
- The examining doctor has both the right and the statutory obligation to take a blood sample for BAC analysis (with consent, or under court order if refused)
- The MLR is prepared on a prescribed form and must be submitted to the requisitioning officer; the doctor may later be called as a court witness
Other legal contexts where intoxication is relevant:
- IPC §85/86: acts done under intoxication — intoxication by consent does not form a defence; involuntary intoxication (administered without knowledge) can be a partial defence
- IPC §328: administering poison (including alcohol) to commit an offence
- Life insurance policies and accidental death claims where alcohol intoxication was a contributing factor
Provided image
Toxicokinetics: Widmark Formula and Blood Alcohol Estimation
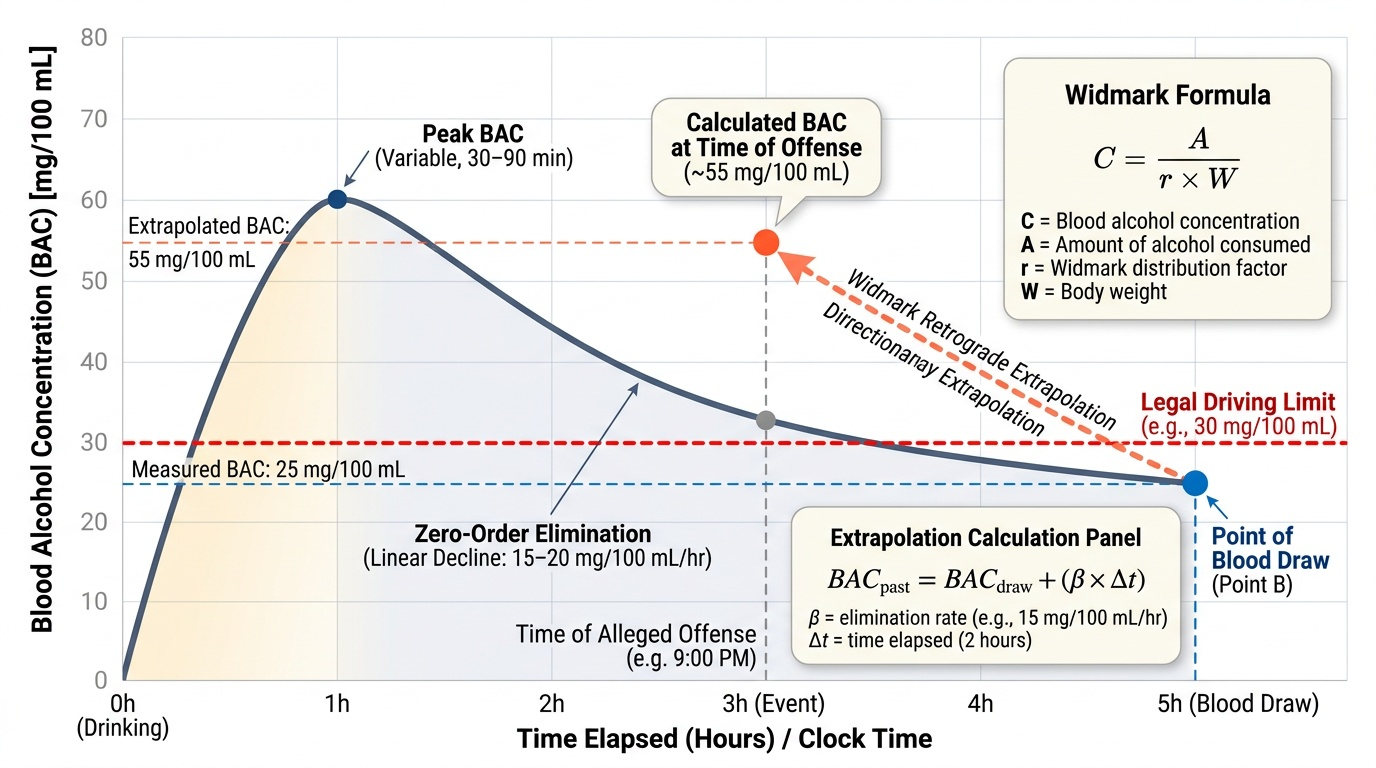
Understanding how blood alcohol concentration (BAC) correlates with the quantity consumed and the time elapsed is fundamental to forensic alcohol work. The Widmark formula is the standard equation used to calculate BAC or to back-calculate (retrograde extrapolation) to an earlier time point.
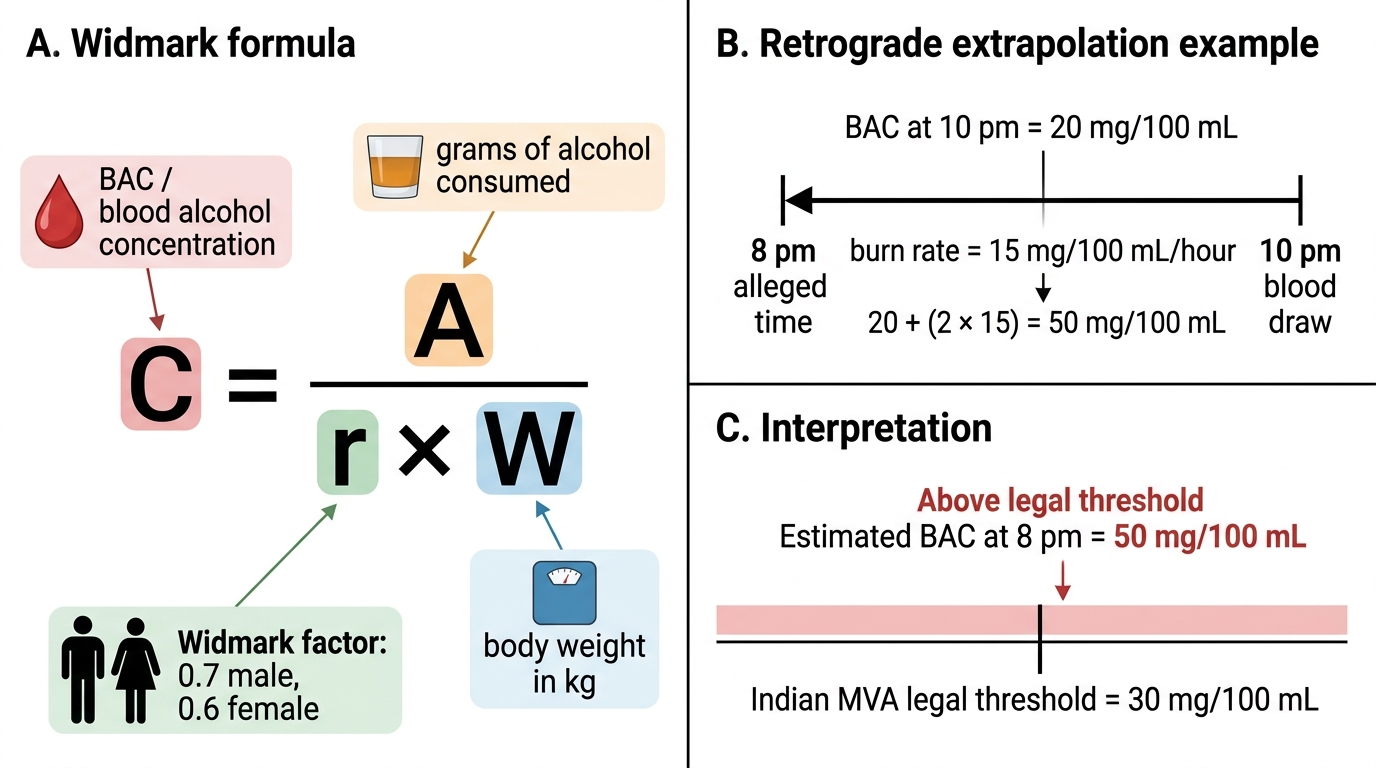
Widmark formula:
C = A / (r × W)
Where:
- C = blood alcohol concentration (in g/100 mL or g/kg)
- A = total amount of alcohol consumed (in grams)
- r = Widmark distribution factor (also called volume of distribution coefficient)
- r = 0.7 for males (approximately 70% of body water)
- r = 0.6 for females (lower body water percentage due to higher body fat)
- W = body weight in kilograms
Retrograde extrapolation:
To estimate BAC at an earlier time (e.g., at the time of the alleged offence rather than at the time of examination), the burn rate of ethanol must be applied. Ethanol is eliminated at a rate of approximately 10–15 mg/100 mL/hour (this is a fixed rate because ADH is saturated — zero-order kinetics). Add this amount back to the measured BAC for each hour elapsed between the alleged event and the blood draw.
Example calculation: A 70 kg male is alleged to have been driving at 9 pm. Blood drawn at 11 pm shows BAC of 25 mg/100 mL. Retrograde extrapolation: 25 + (2 hours × 15 mg/hour) = 55 mg/100 mL at 9 pm — above the 30 mg/100 mL Indian legal threshold.
Toxicokinetic phases of ethanol:
- Absorption phase (0–1 h): BAC rises; affected by gastric contents, rate of consumption, and food co-ingestion
- Peak BAC: variable; typically 30–90 minutes after last drink on empty stomach
- Elimination phase: linear decline at 10–15 mg/100 mL/h (zero-order kinetics)
Provided image
Method: Systematic Drunkenness Examination and Documentation
The examination of an alleged drunk person is a methodical procedure. The following is the standard systematic approach for preparing a medicolegal report (MLR) as per the format used in Indian forensic practice.
Step 1 — Identity and consent:
Record full name, age, sex, address, and identification (as stated by the person and the police officer). Explain the procedure and obtain written consent for examination and blood collection. If consent is refused, document the refusal and note that you will proceed with the external examination only; blood collection without consent requires a court order.
Step 2 — History:
Record time and place of alleged intoxication, substance alleged to have been consumed, quantity, and time of last drink. Note any medical conditions, medications (particularly central nervous system medications), or recent trauma (head injury can mimic intoxication).
Step 3 — General examination:
- Smell: alcohol/ethanol odour on breath; absence of smell does NOT exclude intoxication (methanol, drugs)
- Gait: ability to walk straight line (tandem gait); staggering, swaying
- Coordination: finger-nose test, Romberg's sign
- Speech: clarity, coherence, slurring
- Behaviour: cooperative/aggressive/stuporous
Step 4 — Systemic examination:
- Eyes: conjunctival congestion (bloodshot); pupillary size and reaction to light; nystagmus (horizontal nystagmus is a reliable early sign of significant intoxication)
- CNS: level of consciousness (GCS); orientation to time, place, person; memory (short-term — 'what did you eat tonight?')
- Vital signs: pulse rate, blood pressure, respiratory rate; temperature
- Evidence of trauma: check for head injury (haematoma, lacerations) that could independently explain altered consciousness
Step 5 — Samples:
- Blood (venous, 10 mL in fluoride-oxalate tube — fluoride preserves ethanol): mandatory; label with name, time, date, and signature
- Urine (optional but corroborative): ethanol appears in urine slightly later than blood
- Chain-of-custody labelling and handing over to the police officer with signature
Step 6 — Opinion:
The MLR opinion should state whether the person appears to be 'under the influence of alcohol or drugs' based on the clinical findings — it does NOT require a BAC result at the time of examination. The blood result is typically available later and added as a supplement. The clinical opinion is independent of the biochemical result.
Widmark Formula and Retrograde BAC Extrapolation
SELF-CHECK
A 60 kg woman is alleged to have been drunk at 8 pm. Blood is drawn at 10 pm and shows BAC of 20 mg/100 mL. Using the burn rate of 15 mg/100 mL/hour, what was the estimated BAC at 8 pm?
A. 20 mg/100 mL (no change — blood level is constant after absorption)
B. 50 mg/100 mL — above the Indian legal threshold of 30 mg/100 mL
C. 35 mg/100 mL — at 8 pm she was above the Indian threshold but only marginally
D. 80 mg/100 mL — she was severely intoxicated at 8 pm
Reveal Answer
Answer: B. 50 mg/100 mL — above the Indian legal threshold of 30 mg/100 mL
Retrograde extrapolation: 20 mg/100 mL (at 10 pm) + (2 hours × 15 mg/100 mL/hour) = 50 mg/100 mL at 8 pm. This is above the Indian MVA legal threshold of 30 mg/100 mL. Answer A is wrong because ethanol is eliminated continuously; C is wrong (20 + 30 = 50, not 35); D is wrong (20 + 30 = 50, not 80).
Applied Practice: Methanol, Ethylene Glycol and Hooch Tragedies
The applied forensic practice of alcohol toxicology extends beyond ethanol to the toxic alcohols — methanol and ethylene glycol — and to the public health emergency of hooch tragedies.
METHANOL (CH₃OH) — the 'wood alcohol' of hooch tragedies:
Methanol itself produces only mild inebriation (similar to ethanol in the early hours). The toxicity is almost entirely due to its metabolic products. ADH metabolises methanol to formaldehyde (brief intermediate), which is rapidly converted to formic acid by aldehyde dehydrogenase. Formic acid is the principal toxic metabolite — it inhibits cytochrome c oxidase (Complex IV of the mitochondrial electron transport chain), producing:
- High anion-gap metabolic acidosis (formic acid → H⁺ + formate⁻)
- Optic nerve and retinal toxicity — the retinal pigment epithelium and optic nerve have high metabolic demands; formate inhibition of Complex IV causes selective degeneration → blindness (a characteristic and often permanent sequela)
Latent period of 12–24 hours between ingestion and symptom onset (because ADH metabolism of methanol is slower than ethanol, and symptoms begin when sufficient formic acid has accumulated). During this period the patient may appear merely 'drunk'.
Characteristic signs: visual disturbance ('snowfield vision', scotoma, reduced acuity → total blindness); severe metabolic acidosis; abdominal pain.
Antidote for methanol — two strategies:
1. Ethanol (competitive inhibitor): ethanol is a PREFERRED substrate for ADH, so administering ethanol competitively blocks methanol metabolism, preventing formic acid formation. Used when fomepizole is unavailable (e.g., in resource-limited settings — common in Indian hooch scenarios). Target blood ethanol: 100–150 mg/100 mL.
2. Fomepizole (4-methylpyrazole): a specific ADH inhibitor; safer and more titratable than ethanol; preferred where available.
3. Supportive: folate/folinic acid supplements conversion of formate to CO₂ (formate catabolism requires tetrahydrofolate) — adjuvant treatment.
4. Haemodialysis: removes both methanol AND formic acid; indicated in severe metabolic acidosis, visual impairment, or serum methanol >50 mg/dL.
HOOCH TRAGEDIES in India:
Illicit liquor (hooch) is distilled in informal settings where fractional distillation is inadequate or deliberately bypassed to increase yield. Methanol has a lower boiling point (64.7°C) than ethanol (78.4°C) — in distillation, if the 'foreshots' (the first fraction, methanol-rich) are not discarded, the product contains methanol. Some unscrupulous producers add industrial methanol to increase the apparent alcohol content. Hooch tragedies are mass-casualty events with tens to hundreds of deaths and many more cases of permanent blindness.
Medicolegal role in a hooch tragedy:
- Establish the diagnosis (characteristic latent period + visual symptoms + metabolic acidosis + survivors reporting same source)
- Collect samples from survivors and deceased for methanol/formic acid analysis
- Report to public health authorities for source identification and prevention
- IPC sections applicable: §304 (culpable homicide not amounting to murder) or §304A (criminal negligence) for the brewer/distributor
ETHYLENE GLYCOL (antifreeze):
Ethylene glycol is also metabolised by ADH — its toxic products are glycolic acid → oxalic acid (the same oxalic acid seen in plant poisoning). Oxalic acid precipitates calcium → systemic hypocalcaemia AND calcium oxalate crystal deposition in renal tubules → acute renal failure. Unlike methanol, ethylene glycol does NOT cause blindness but causes severe renal failure.
Antidote: same as methanol — ethanol or fomepizole (block ADH to prevent oxalate formation). Haemodialysis.
Provided image
CLINICAL PEARL
Methanol is metabolised to formic acid — NOT formaldehyde. The formaldehyde is an intermediate that is rapidly converted. The toxicity and blindness of methanol poisoning are caused by formic acid, not formaldehyde. This distinction is critical both factually and for treatment: folate supplementation supports formate catabolism (formate → CO₂ via folate-dependent pathway), which is why folinic acid is given as an adjuvant. Additionally: the Indian legal BAC threshold is 30 mg/100 mL under the Motor Vehicles Act — not 0.08% (the US standard). Never import foreign thresholds into Indian forensic reports.
SELF-CHECK
In a hooch tragedy, 40 survivors present 18–24 hours after drinking illicit liquor with visual disturbances, severe abdominal pain, and ABG showing pH 7.12 with anion gap of 28 mEq/L. The most important IMMEDIATE antidote treatment (available in most Indian district hospitals) is:
A. IV sodium bicarbonate alone to correct acidosis
B. Oral/IV ethanol administered to achieve blood ethanol of 100–150 mg/100 mL
C. IV deferoxamine to chelate the methanol
D. IV diazepam to prevent seizures from metabolic acidosis
Reveal Answer
Answer: B. Oral/IV ethanol administered to achieve blood ethanol of 100–150 mg/100 mL
Methanol poisoning — confirmed by the latent period, visual symptoms, and high anion-gap metabolic acidosis. The antidote is competitive inhibition of ADH with ethanol (or fomepizole if available). Ethanol is the practical first-line in Indian district hospitals where fomepizole is not stocked. Target blood ethanol 100–150 mg/100 mL blocks methanol metabolism by competing for ADH. Sodium bicarbonate corrects acidosis transiently but does not stop formic acid production; deferoxamine is for iron; diazepam addresses seizures only.
KEY TAKEAWAYS
Alcohol forensics (FM13.14, FM14.15) spans three skill domains:
1. Drunkenness examination (FM14.15): Statutory examination under MVA §185. Indian BAC threshold: 30 mg/100 mL (0.03%) — NOT 0.08%. Widmark formula: C = A / (r × W); r = 0.7 (male), 0.6 (female). Retrograde extrapolation using elimination rate 10–15 mg/100 mL/h. MLR opinion on clinical intoxication is independent of lab BAC.
2. Ethanol toxicokinetics: ADH → acetaldehyde → acetate; zero-order elimination; GABA enhancement + NMDA inhibition → CNS depression.
3. Toxic alcohols (FM13.14):
- Methanol: ADH → formaldehyde → formic acid → optic nerve toxicity + metabolic acidosis; 12–24 h latent period; antidote = ethanol (competitive ADH inhibitor) or fomepizole; HD for severe cases
- Ethylene glycol: ADH → glycolic acid → oxalic acid → renal failure (no blindness); antidote = ethanol or fomepizole; HD
- Hooch tragedies: illicit methanol-contaminated liquor; foreshots not discarded; public health emergency; IPC §304/304A for perpetrators
REFLECT
A hooch tragedy has just occurred in a rural district — 25 people have died and 60 survivors are being brought to the district hospital. You are the senior doctor on duty. Beyond the immediate treatment priorities (which you have just learned), what is your medicolegal duty in this situation? Specifically: what samples should be collected and how should they be preserved? How do you notify the appropriate statutory authorities? And in the context of future legal proceedings against the producers of the illicit liquor, what documentation would be most valuable — and who should be involved in collecting it?