Page 2 of 33
FM13.11 | Corrosive Poisons (Acids) — SDL Guide (Part 2)
Clinical Examination and Documentation in Corrosive Poisoning
Clinical examination in suspected acid poisoning serves a dual purpose: it is simultaneously a life-saving assessment and the collection of medicolegal evidence. These two functions cannot be separated — the history, examination findings, and biological samples obtained in the emergency setting form the evidentiary record. As the examining doctor, you must be systematic and contemporaneous.
History and documentation of exposure:
Record the exact time of exposure, the nature of the substance (if known), the route (skin/eye/ingestion/inhalation), the quantity, any first-aid measures already taken, and the source of information (patient, bystander, accompanying police). Document verbatim statements in quotes.
General examination and vital signs:
Assess airway, breathing, and circulation first. Acid vapour inhalation (especially H₂SO₄, HNO₃, HCl fumes) may cause laryngeal oedema and upper airway compromise — listen for stridor. Burns involving the face/neck raise the risk of oropharyngeal burns with rapid airway swelling. Document pulse rate, blood pressure, respiratory rate, and GCS/consciousness level.
Local examination — skin and mucous membranes:
- Record the distribution of burns (extent, depth, body surface area — use Lund-Browder chart for burns documentation)
- Note the characteristic colour/appearance of the eschar (see Classification section above)
- Photograph injuries with scale marker (or describe precisely in words if photography is not available)
- Note splash pattern vs contact pattern vs ingestion pattern
Specific systemic findings by agent:
- Carbolic acid/phenol: assess CNS (initial excitability → CNS depression → coma), renal function, inspect urine (carboluria = green/black)
- Oxalic acid: look for Trousseau's sign, Chvostek's sign (hypocalcaemia); ECG for prolonged QT
- Aspirin: assess for hyperventilation, tinnitus, level of consciousness, temperature; ABG analysis
Post-mortem appearances (PM findings for FM exam):
- Sulphuric acid: blackened/charred mucosa from mouth to stomach; heat injury artefact from exothermic reaction
- Nitric acid: yellow staining of mucosa, stomach contents
- Carbolic acid: phenolic smell of viscera; greenish-black discolouration of organs; kidney shows haemorrhagic nephritis
- Oxalic acid: calcium oxalate crystals in renal tubules (microscopy); relatively mild mucosal changes
Sampling for forensic analysis:
Collect gastric washings, blood, urine, and vitreous humour (if PM) with sterile technique; label, seal, sign, and hand over with chain of custody documentation.
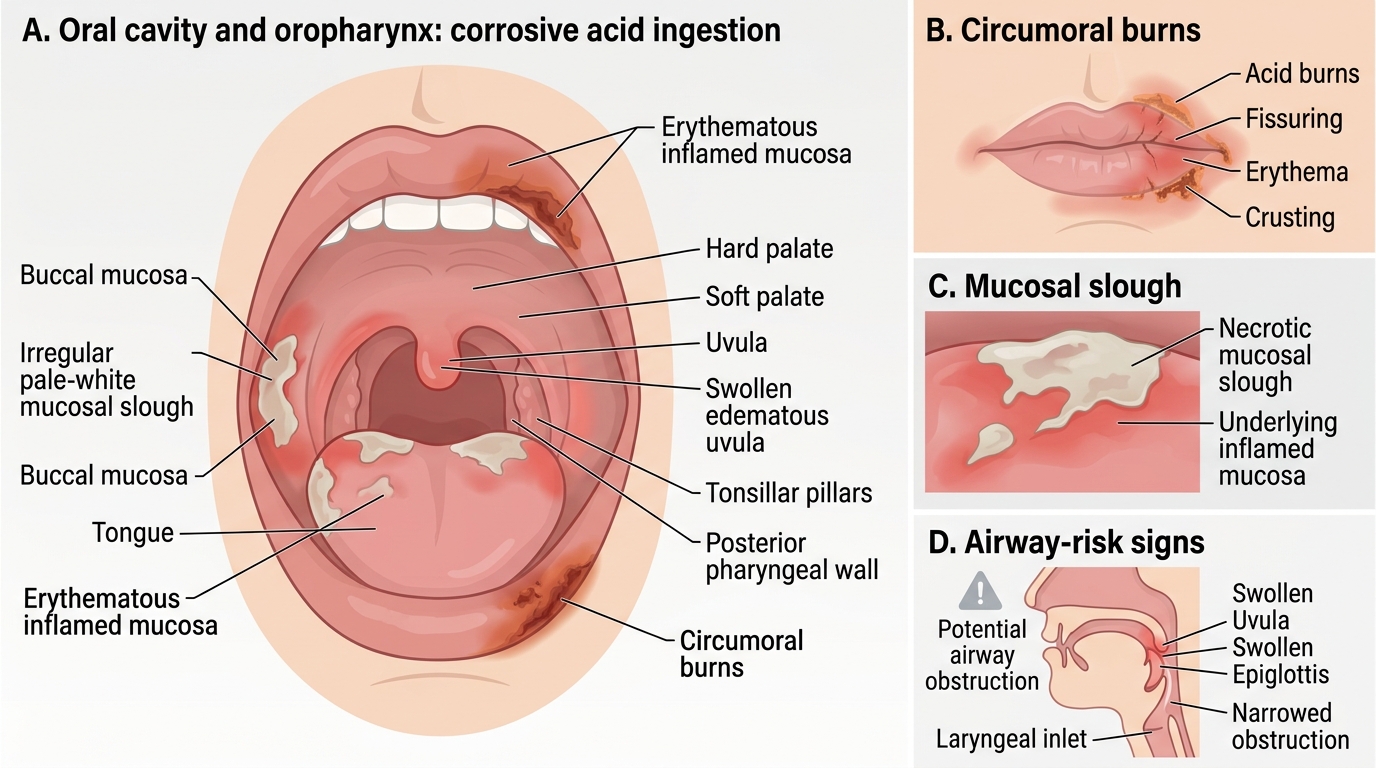
Oral and Oropharyngeal Findings in Corrosive Acid Ingestion
SELF-CHECK
A patient who ingested carbolic acid (phenol) develops dark green-black urine, has a low Glasgow Coma Scale score, and shows signs of acute renal impairment. The urine finding is best explained by:
A. Rhabdomyolysis releasing myoglobin into urine
B. Phenol metabolites (carboluria) from systemic absorption
C. Haemolysis from direct red cell membrane toxicity
D. Obstructive uropathy from calcium oxalate crystals
Reveal Answer
Answer: B. Phenol metabolites (carboluria) from systemic absorption
Phenol is rapidly absorbed systemically and undergoes hepatic conjugation; phenol and its metabolites (particularly catechol, quinol) are excreted in urine, turning it dark green/black — this is carboluria, the hallmark of carbolic acid systemic absorption. Myoglobinuria gives brown/cola urine (rhabdomyolysis); haemolysis gives pink-red urine; oxalate crystals are a feature of oxalic acid poisoning, not phenol.
Medicolegal Inference, Treatment Principles and Statutory Framework
The management framework for corrosive acid poisoning follows the universal toxicology schema — decontamination, supportive care, specific antidotes (where available), and enhanced elimination — but each agent has important specific modifications. Simultaneously, the forensic medicine doctor must place the injury in its statutory context.
Treatment framework per agent:
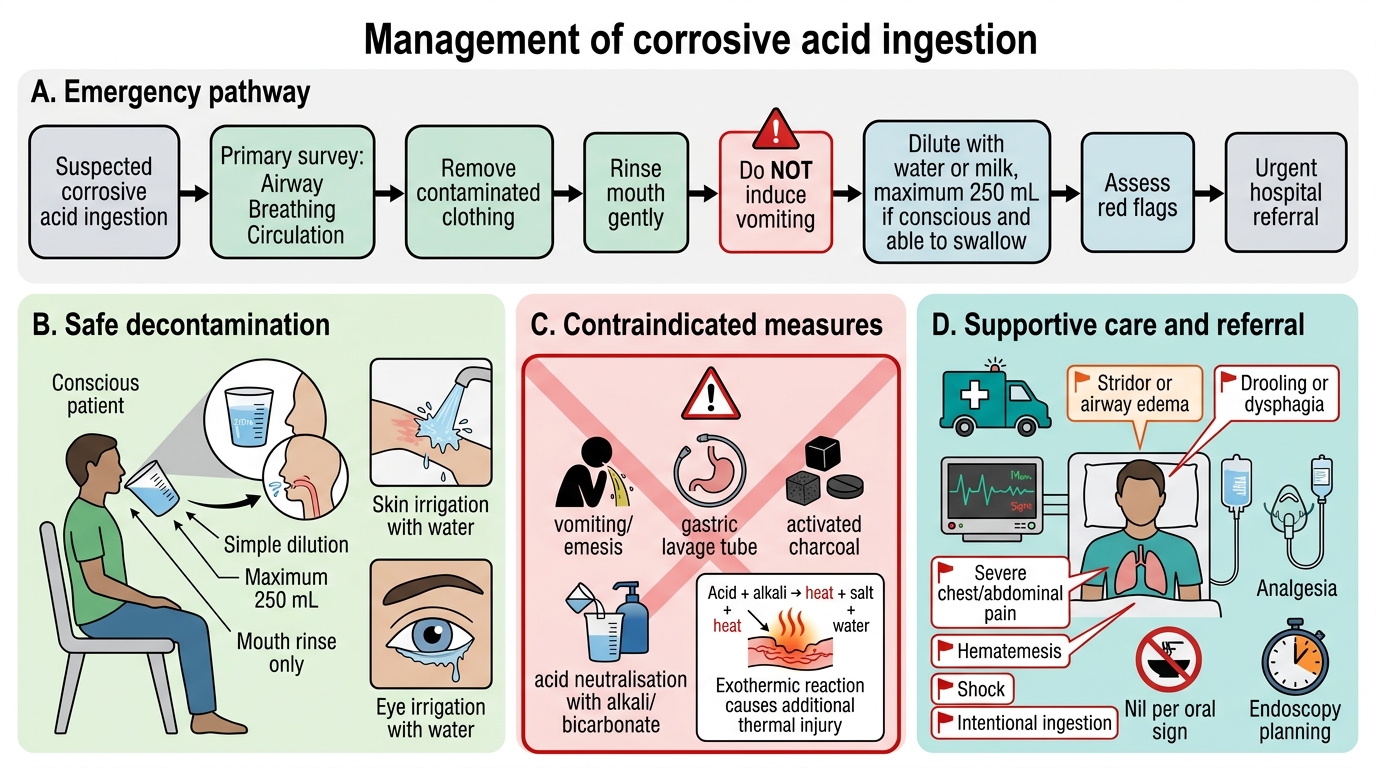
All corrosive acid ingestions (general principles):
- Do NOT induce emesis (re-exposure of oesophagus and oropharynx)
- Do NOT neutralise with alkali (exothermic reaction worsens injury)
- Dilution with water/milk within minutes of ingestion
- Supportive: IV fluids, airway management, pain control, nil orally until endoscopy assessment
Agent-specific antidotes and modifications:
- Carbolic acid/phenol: specific antidote — supportive care only for local burns; systemic toxicity managed with N-acetylcysteine (as hepatoprotective adjunct), haemodialysis for severe renal impairment. There is no specific phenol antidote.
- Oxalic acid: specific treatment — IV calcium gluconate (to correct hypocalcaemia and convert free oxalate to insoluble calcium oxalate in blood, reducing free ion toxicity); vigorous hydration to prevent renal tubular crystal deposition.
- Acetylsalicylic acid (aspirin) overdose: the most important specific intervention is urinary alkalinisation (IV sodium bicarbonate to maintain urine pH 7.5–8.0) — alkaline urine traps ionised salicylate (ion trapping), increasing renal salicylate clearance. Haemodialysis is indicated for serum salicylate >350 mg/L, severe metabolic acidosis, renal failure, pulmonary oedema, or severe CNS effects. Oral activated charcoal is useful within 1–2 hours of ingestion.
- Mineral acids (H₂SO₄, HNO₃, HCl): no specific antidote. Supportive care; endoscopy at 24–48 h to assess oesophageal/gastric damage and guide further management.
Enhanced elimination summary:
- Aspirin: haemodialysis (high protein-binding clearance by HD) + urinary alkalinisation
- Oxalic acid: IV calcium, forced diuresis
- Carbolic acid severe cases: haemodialysis
- Mineral acids: no enhanced elimination role
Medicolegal and statutory framework:
Acid attacks in India are governed by several legal provisions:
- IPC §326A (inserted 2013): voluntarily causing grievous hurt by use of acid — punishable with minimum 10 years imprisonment (may extend to life)
- IPC §326B: voluntarily throwing or attempting to throw acid — minimum 5 years imprisonment
- IPC §320: grievous hurt — includes permanent disfigurement of face/head (item 7), permanent loss of sight or hearing; acid attacks almost invariably cause grievous hurt by this definition
- Supreme Court: Laxmi v. Union of India (2013): directed regulation of acid sale (identity proof required, quantities >500 mL restricted) and established framework for victim compensation
For MLR preparation: document acid type (chemical/physical characteristics), injury distribution and depth, functional impairment (especially visual loss — document Snellen acuity), permanent disfigurement (percentage, Body Surface Area affected), and prognosis. Opine on whether injuries are consistent with the alleged mechanism.
Emergency Management of Corrosive Acid Ingestion
CLINICAL PEARL
Never neutralise an ingested acid with an alkali in the GI tract. This is an intuitive but dangerous manoeuvre — the neutralisation reaction (acid + base → salt + water) is exothermic, releasing heat that causes additional thermal injury to already-damaged mucosa. The standard emergency measure is simple dilution with water or milk (maximum 250 mL), which does not produce heat and reduces contact concentration. The same principle applies externally: copious water irrigation is the decontamination of choice for skin/eye exposure — not bicarbonate solution.
SELF-CHECK
A 35-year-old intentionally ingested 20 tablets of aspirin (500 mg each — total 10 g). ABG shows pH 7.52, PaCO₂ 28 mmHg, HCO₃⁻ 22 mEq/L. Which acid-base disturbance is this, and what is the most important specific treatment?
A. Metabolic alkalosis — treat with IV hydrochloric acid
B. Respiratory alkalosis (early aspirin toxicity) — treat with urinary alkalinisation with IV sodium bicarbonate
C. Mixed metabolic acidosis and respiratory alkalosis — immediate haemodialysis
D. Respiratory alkalosis — treat with activated charcoal only, no further intervention needed
Reveal Answer
Answer: B. Respiratory alkalosis (early aspirin toxicity) — treat with urinary alkalinisation with IV sodium bicarbonate
This ABG shows respiratory alkalosis (elevated pH + low PaCO₂ with near-normal HCO₃⁻) — the early phase of aspirin toxicity from direct stimulatory effect on the respiratory centre. At this stage, the key intervention is urinary alkalinisation with IV sodium bicarbonate (maintain urine pH 7.5–8.0) to achieve ion trapping of salicylate in urine (ionised form not reabsorbed). Haemodialysis is reserved for serum salicylate >350 mg/L, renal failure, pulmonary oedema, or severe CNS effects — this early presentation does not yet warrant it.