Page 25 of 33
FM13.20 | Drug Abuse, Mushroom & Food Poisoning — SDL Guide (Part 2)
Food Poisoning: Organisms, Mechanisms and Investigation
Food poisoning is defined as acute illness caused by consumption of food or drink contaminated with pathogenic organisms or their toxins. Mass food poisoning — particularly at community gatherings, school midday meals, and hospital canteens — is a frequent cause of medicolegal investigation, public health notification, and civil litigation in India.
Classification by mechanism and onset time:
SHORT INCUBATION (1–6 h) — pre-formed toxin in food:
- Staphylococcus aureus (1–6 h): toxin-mediated vomiting (emetic toxin — heat-stable). No fever. Source: contaminated dairy, sweets, cooked foods left at room temperature. Diagnosis: isolate Staph from food remnant.
- Bacillus cereus emetic type (1–6 h): same pattern as Staph; fried rice syndrome. Short onset, profuse vomiting, no fever.
INTERMEDIATE INCUBATION (6–24 h):
- Clostridium perfringens (8–24 h): large-volume watery diarrhoea, cramps, NO vomiting; enterotoxin. Source: improperly reheated meat.
- Bacillus cereus diarrhoeal type (6–15 h): watery diarrhoea; heat-labile enterotoxin; often vegetables/meat dishes.
LONG INCUBATION (>24 h) — invasive pathogens:
- Salmonella (12–72 h): fever + diarrhoea ± vomiting; systemic bacteraemia risk; Source: eggs, poultry.
- Vibrio cholerae (12–72 h): rice-water diarrhoea; massive fluid loss; dehydration is the cause of death.
BOTULISM (special case — neurological):
- Clostridium botulinum: pre-formed neurotoxin (or in-situ production in wounds/intestine). Toxin blocks ACh release at pre-synaptic NMJ AND autonomic junctions → descending flaccid paralysis (cranial nerve palsies first — diplopia, dysarthria, dysphagia) + autonomic dysfunction (dry mouth, constipation, urinary retention). Source: home-canned/preserved foods (anaerobic conditions allow C. botulinum growth). Treatment: antitoxin (trivalent A/B/E botulinum antitoxin); supportive ventilation.
Mass food poisoning investigation — forensic medicine role:
When a mass food poisoning outbreak occurs, the forensic medicine specialist participates in:
1. Clinical diagnosis and triage of victims
2. Collection of food samples, clinical specimens (stool, blood, vomitus) for microbiological and toxicological analysis
3. Estimation of the common food vehicle (attack rate analysis — epidemiological investigation)
4. Preparing reports for public health authorities (mandatory notification under the Epidemic Diseases Act)
5. Medicolegal opinion on whether negligence by the food preparer/vendor caused harm
Legal framework — food safety and food poisoning:
- Food Safety and Standards Act (FSSA) 2006: the central statute governing food safety in India; Food Safety and Standards Authority of India (FSSAI) is the regulatory body
- Prevention of Food Adulteration Act 1954: now largely replaced by FSSA 2006 but may still be cited in old cases
- IPC §272 (adulteration of food or drink), §273 (sale of noxious food or drink): criminal provisions for deliberate adulteration
- Consumer Protection Act 2019: civil claims for food poisoning negligence
- Epidemic Diseases Act 1897: may be invoked for large-scale outbreaks
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
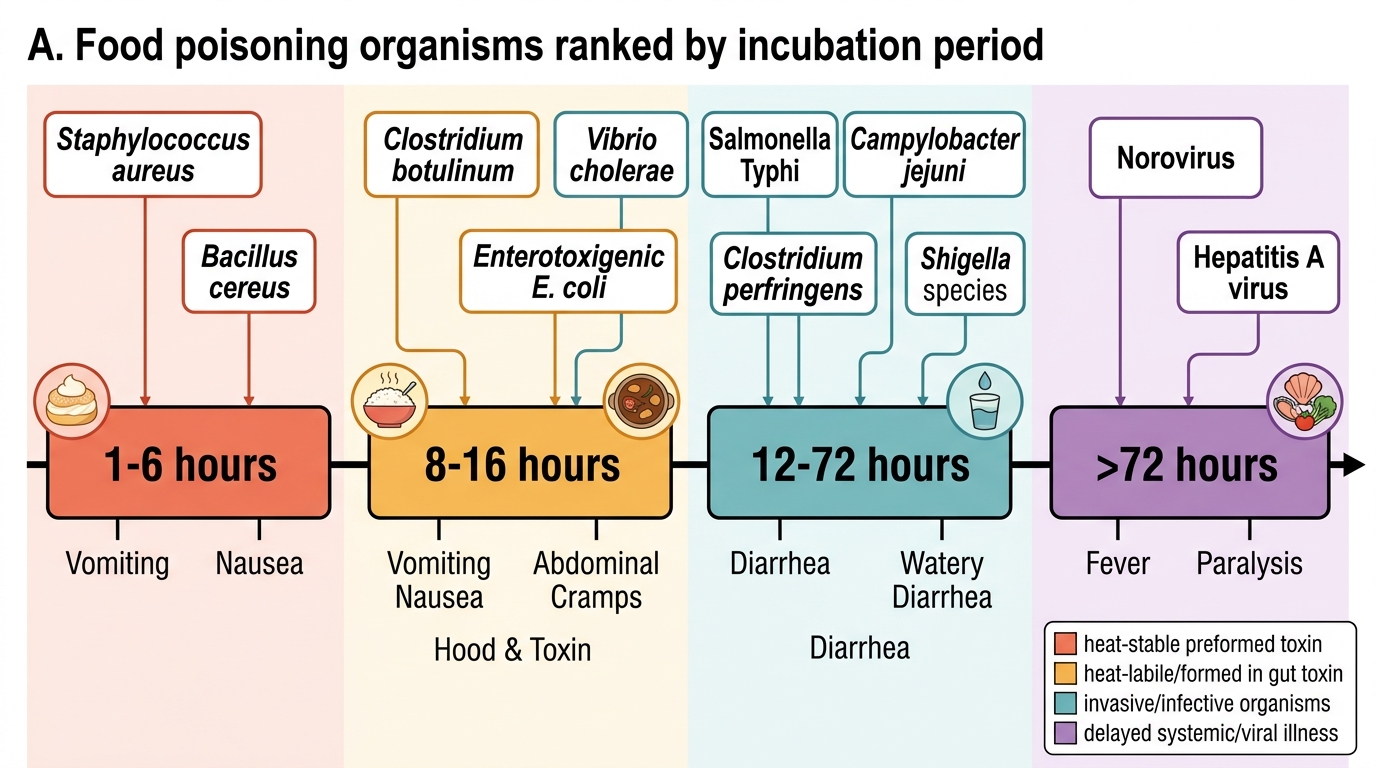
Food Poisoning Timeline by Incubation Period
Clinical Examination and Medicolegal Documentation
Drug abuse cases — examination and documentation:
For a living patient suspected of drug abuse or drug-facilitated assault:
- Detailed toxidrome identification (sympathomimetic/serotonergic vs cholinergic vs sedative-hypnotic vs hallucinogenic)
- Urine drug screen (immediately on presentation — many drugs have short detection windows, especially GHB which is undetectable in urine within 12 hours)
- Blood for quantitative drug levels (if toxidrome suggests specific agent)
- Document consent, chain of custody for all specimens
- For drug-facilitated assault: preserve urine/blood in sealed tubes with 4-fold witnessed labels before sending to forensic laboratory
For post-mortem drug-related death:
- Routine toxicological screen (blood + urine + vitreous + liver) for all unexplained deaths in persons aged 15–45
- Hair analysis for chronic use timeline reconstruction (drug deposited in growing hair — 1 cm/month of growth = 1 month's history)
Mushroom and food poisoning cases — documentation:
In a mass-poisoning event:
- Detailed attack-rate record (who ate what, who got sick — epidemiological table)
- Food samples (from the implicated dish, preserved at 4°C or frozen)
- Clinical specimens: stool (for organism culture), blood (for bacteraemia), vomitus
- Time of symptom onset relative to meal time (helps identify toxin type by incubation period)
- Photographs of the implicated food and its preparation site
- Witness statements
All specimens must be collected with documented chain of custody if criminal proceedings are anticipated (intentional food adulteration, negligent mass food poisoning).
Treatment summary for drug abuse:
| Toxidrome | Treatment |
|---|---|
| Sympathomimetic (cocaine, amphetamine) | Benzodiazepines; cool; IV fluids; avoid beta-blockers (unopposed alpha in cocaine → worse hypertension) |
| Serotonin syndrome (MDMA) | Cyproheptadine (5-HT2A antagonist); benzodiazepines; active cooling; avoid paracetamol (high temp + paracetamol → hepatotoxicity) |
| Cannabis acute psychosis | Benzodiazepines; haloperidol if severe |
| Solvent inhalation | Avoid adrenaline (sensitised myocardium → VF); supportive |
| Botulism | Antitoxin; ventilatory support |
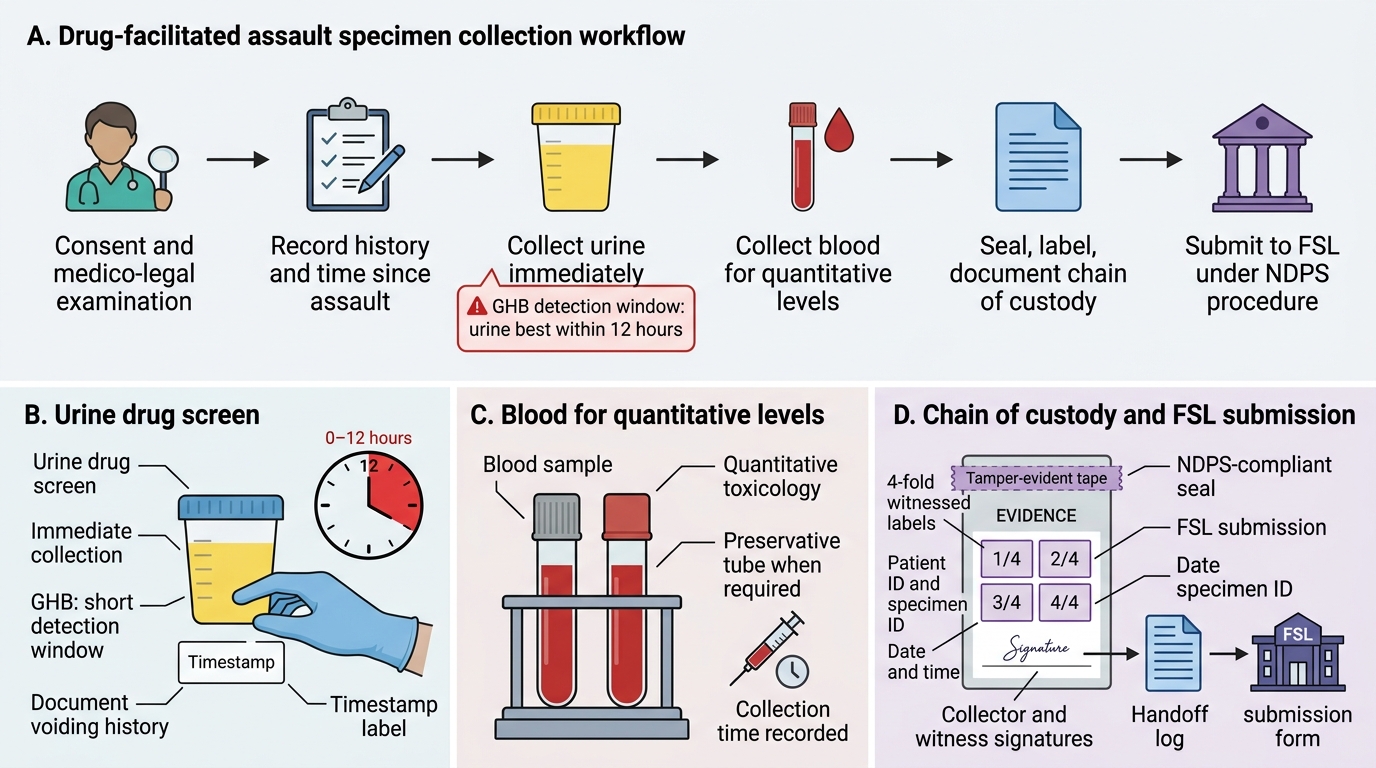
Drug-Facilitated Assault Specimen Collection Flowchart
CLINICAL PEARL
The incubation time is the key to mushroom toxin identification — and 'feeling better' after 24 hours may be the most dangerous sign. Amatoxin (Amanita phalloides) poisoning has a 6–24 hour latency, followed by a 'false recovery' that often leads to premature discharge from hospital, only for fulminant hepatic failure to develop on days 4–7. Any mushroom ingestion followed by GI symptoms and then apparent recovery should be presumed to be amatoxin poisoning until proved otherwise — admission, serial LFTs, and continued monitoring are mandatory, not optional.
SELF-CHECK
In botulism, the characteristic neurological syndrome and its mechanism are:
A. Ascending flaccid paralysis — botulinum toxin blocks post-synaptic nicotinic receptors
B. Descending flaccid paralysis — botulinum toxin blocks pre-synaptic ACh release at the NMJ and autonomic junctions; cranial nerves affected first
C. Ascending spastic paralysis — botulinum toxin activates AChE, preventing ACh clearance
D. Flaccid paralysis with intact sensation — botulinum toxin selectively blocks motor cortex neurons
Reveal Answer
Answer: B. Descending flaccid paralysis — botulinum toxin blocks pre-synaptic ACh release at the NMJ and autonomic junctions; cranial nerves affected first
Botulinum toxin cleaves SNARE proteins (SNAP-25 for types A and E) at the pre-synaptic terminal, preventing ACh vesicle fusion and release. This blocks both NMJ cholinergic transmission (flaccid paralysis) and autonomic cholinergic junctions (dry mouth, constipation, urinary retention). The paralysis is DESCENDING — cranial nerve NMJs (diplopia, dysarthria, dysphagia) are affected first, followed by trunk and limbs. This is OPPOSITE to the ascending pattern of Guillain-Barré syndrome. Botulinum toxin acts PRE-synaptically (similar to krait beta-bungarotoxin, not to cobra alpha-toxin which is post-synaptic).