Page 21 of 33
FM13.18 | Narcotics, Anaesthetics, Cardiotoxic Plants & Insulin — SDL Guide (Part 2)
Insulin Poisoning: Mechanism, Forensic Challenges and Management
Insulin poisoning — whether accidental (incorrect dose), suicidal, or homicidal — presents the forensic medicine specialist with one of the most challenging investigative scenarios in clinical toxicology.
Mechanism:
Exogenous insulin administered in excess → profound hypoglycaemia → brain glucose deprivation (the brain is almost exclusively dependent on glucose under normal circumstances) → neuronal dysfunction → seizures → coma → irreversible neurological injury → death.
Clinical features of hypoglycaemic coma from insulin overdose:
- Autonomic symptoms (early): sweating, tremor, palpitation, hunger (from catecholamine response to hypoglycaemia)
- Neuroglycopenia (as glucose falls further): confusion, aggression, focal neurological signs
- Severe hypoglycaemia (blood glucose <2.0 mmol/L): seizures, loss of consciousness, coma
- The person may be found in a coma that looks like a natural cause if no one knows they are diabetic or if insulin was administered covertly
Forensic challenge — detecting insulin homicide:
1. Post-mortem glucose is unreliable: Glucose is rapidly metabolised post-mortem by microbial and cellular enzymes → PM blood glucose is almost always low regardless of the ante-mortem level. Normal vitreous glucose may be marginally more reliable but still unreliable.
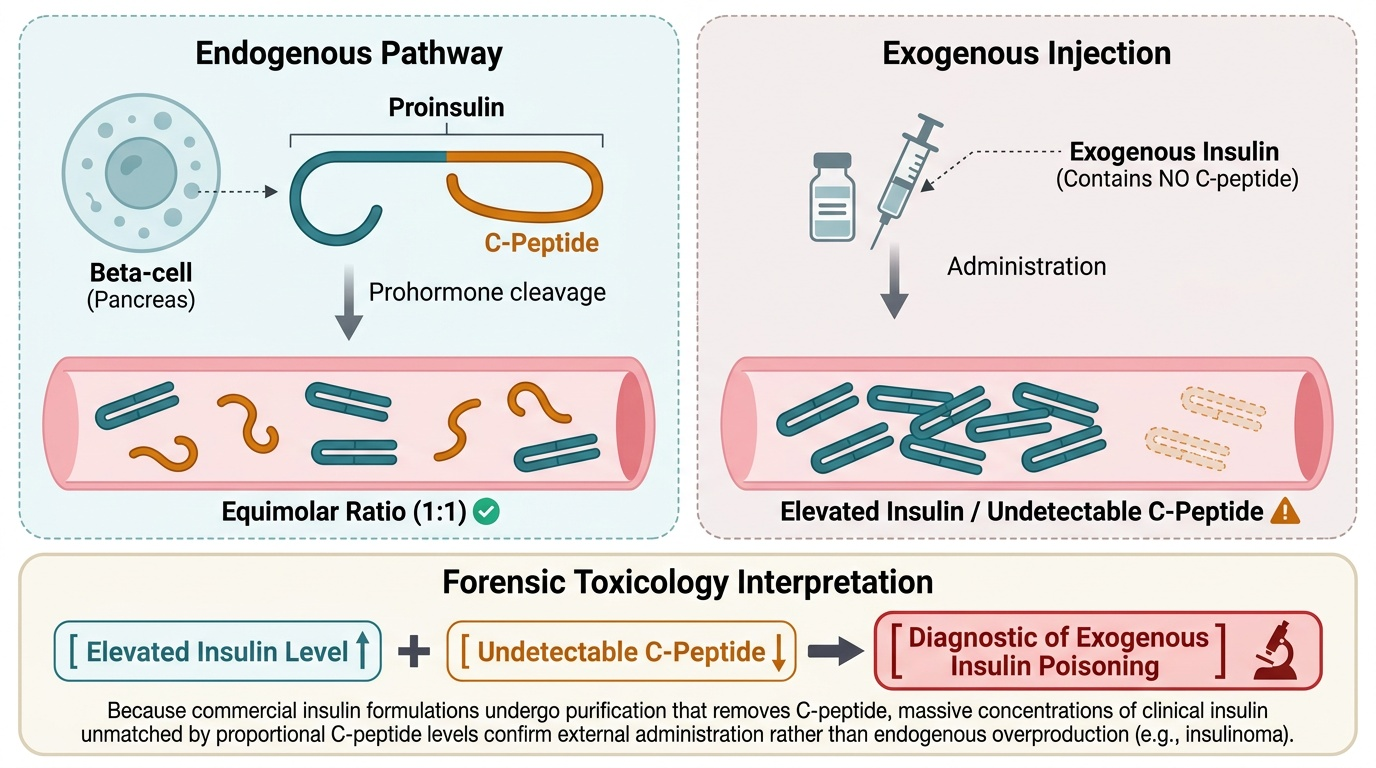
2. C-peptide test — the key forensic marker:
- Endogenous insulin is synthesised as proinsulin → cleaved to insulin + C-peptide (connecting peptide) in equimolar amounts
- Exogenous (injected) insulin preparations do NOT contain C-peptide
- In a suspected insulin homicide, the finding of very low or undetectable C-peptide with elevated insulin levels strongly suggests exogenous insulin administration
- Normal insulin secretion: C-peptide is always present in proportion to endogenous insulin
3. Injection site analysis:
A localised depot of insulin may be identified at an injection site (subcutaneous tissue) using specific immunohistochemistry. The injection site may show a bruise, but this is non-specific.
4. Insulin analogue identification:
Modern insulin analogues (glargine, aspart, detemir) can be specifically identified by LC-MS/MS — this can distinguish the type of insulin administered and potentially trace it to a prescription.
Treatment:
- Mild/moderate hypoglycaemia: oral glucose (juice, sugar water)
- Severe (unconscious): IV dextrose 25–50 mL of 50% dextrose (D50W) immediately
- If IV access is unavailable: IM glucagon (1 mg) — stimulates hepatic glycogenolysis → raises blood glucose
- Maintain blood glucose monitoring; continuous glucose infusion may be required (especially for long-acting insulin overdose)
- For long-acting insulin overdose: octreotide (somatostatin analogue) — inhibits endogenous insulin secretion and is used adjunctively to blunt glucose demand
Provided image
Clinical Examination, PM Documentation and Medicolegal Inference
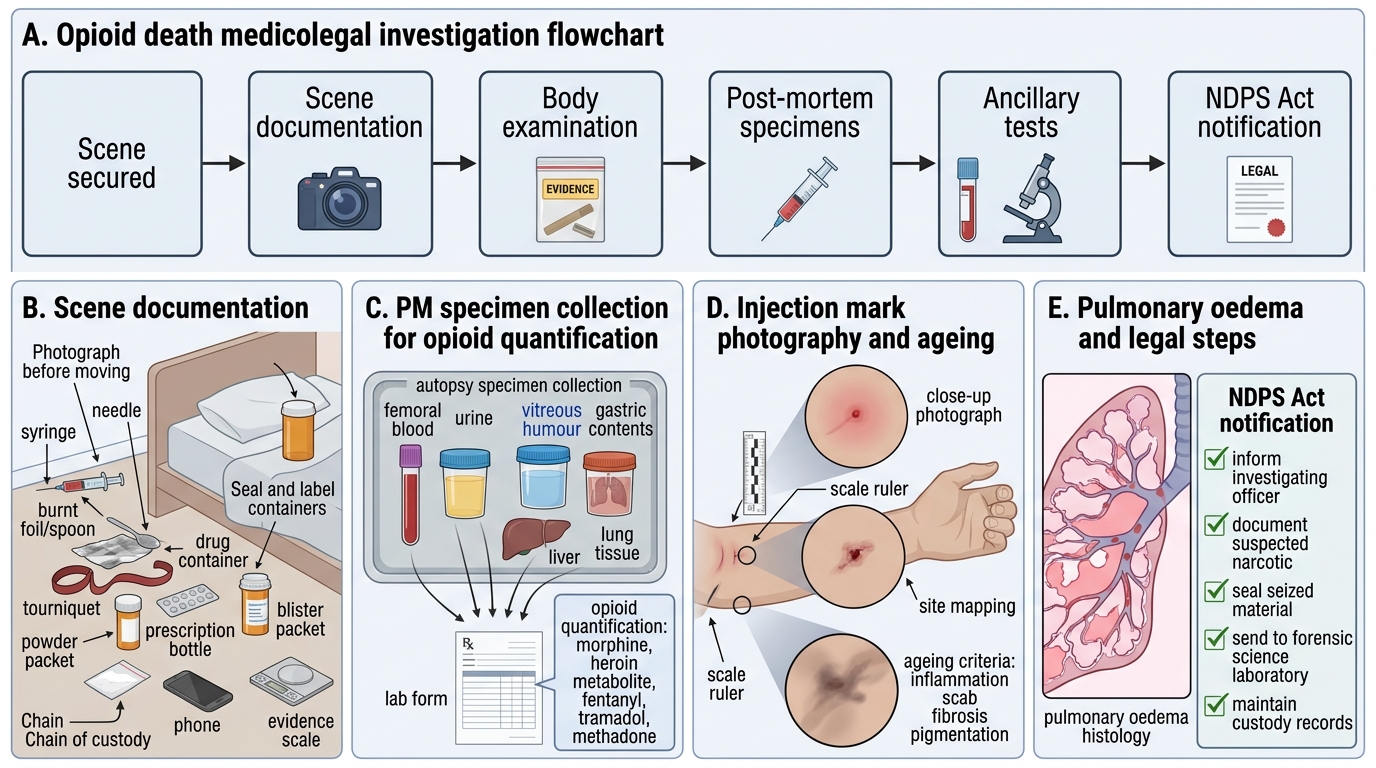
Opioid cases — examination and documentation:
In a living patient: document toxidrome (miosis, respiratory rate, GCS), injection marks (location, number, freshness), any drug paraphernalia at scene. In a PM case: injection marks should be carefully photographed and GPS-documented; skin sections for histology; blood/urine/vitreous humour for opioid quantification; lung histology for pulmonary oedema pattern.
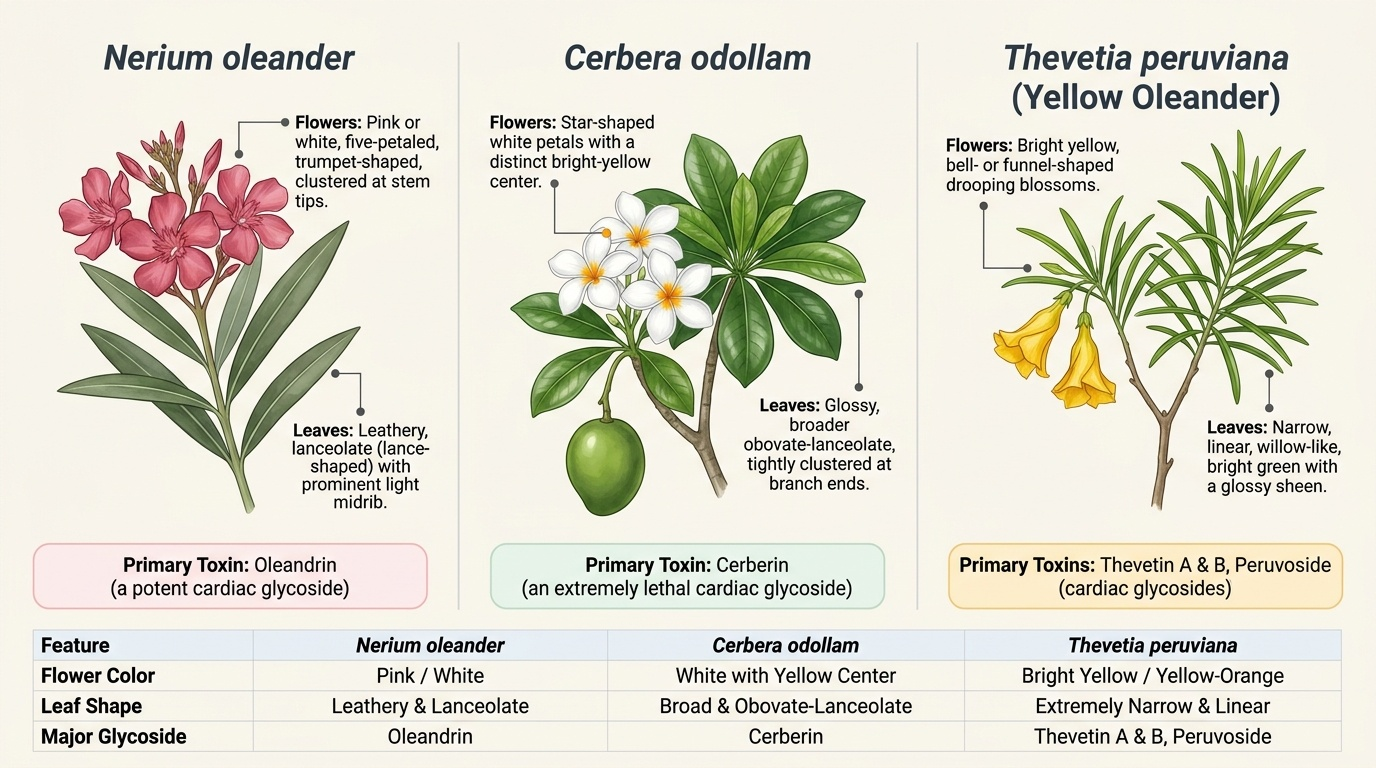
Cardiac glycoside plant poisoning — examination:
Living: ECG is the single most important investigation — bradyarrhythmia, AV block, bidirectional ventricular tachycardia, digitalis effect (scooping of the ST segment, 'reverse tick'). Collect blood for cardiac glycoside assay (oleander/cerberin-specific assay at reference lab); gastric contents if early ingestion.
PM: heart may appear entirely normal; diagnosis depends on toxicological analysis. Collect blood (femoral), gastric contents, liver, urine. Instruct the pathologist to preserve samples for specialised botanical poison analysis.
Insulin poisoning — examination:
Document: blood glucose (must be documented contemporaneously — PM glucose unreliable); serum insulin level; C-peptide level; injection sites (examine all accessible subcutaneous areas carefully — axillae, buttocks, abdomen, thighs); any insulin preparations in the environment.
For PM investigation of suspected insulin homicide:
- Document all injection sites (photograph, excise for immunohistochemistry)
- Collect vitreous humour (most reliable PM specimen for glucose — bacterial contamination is minimal)
- Collect blood from femoral vein in fluoride-oxalate tube IMMEDIATELY at the start of PM (before delay allows further glucose depletion)
- Send for insulin, C-peptide, and insulin analogue LC-MS/MS at a forensic reference laboratory
Provided image
Medicolegal Inference and Statutory Framework
Narcotic deaths — medicolegal framework:
Opioid deaths in India are governed by the NDPS Act 1985 (Narcotics, Drugs and Psychotropic Substances Act) — morphine, heroin, opium, codeine, and their derivatives are Schedule I/II controlled substances. Possession, sale, and manufacture are criminal offences with severe penalties. The forensic doctor's role in a narcotic death:
- Certify cause of death (acute opioid intoxication — confirm analytically)
- Document injection marks (fresh vs old — number and pattern suggests duration of dependency)
- Opine on whether death was a criminal administration or self-use
Cardiotoxic plant poisoning — medicolegal framework:
Oleander and Cerbera poisoning deaths must be distinguished from natural cardiac death. The presence of the plant at the scene, gastric contents analysis, and cardiac glycoside levels are the forensic evidence. Relevant IPC: §302/304 (homicide); §304A (negligence — if an employer or cook allowed or used plant material). Cerbera odollam poisoning in Kerala has been associated with insurance fraud cases (death staged as natural).
Insulin homicide — IPC framework:
Insulin homicide, while rare, is one of the most legally complex forensic cases. Relevant IPC:
- IPC §302 (murder) — if intent and administration are proved
- IPC §328 (causing hurt by poison)
The challenge is proof: insulin is endogenous, the PM evidence is difficult, and the defence may argue that the victim self-administered. The C-peptide test and insulin analogue identification are the forensic anchors.
Treatment summary for this SDL group:
| Agent | Specific antidote | Key emergency intervention |
|---|---|---|
| Opioids | Naloxone (0.4–2 mg IV; repeat as needed) | Airway/ventilation support |
| Cardiac glycoside plants | Digoxin Fab antibodies | Atropine for bradycardia/AV block |
| Aconite | None specific | Cardiac monitoring; amiodarone for arrhythmia |
| Insulin overdose | IV dextrose (50% D50W); IM glucagon | Continuous BGL monitoring |
| Succinylcholine/NMBs | Sugammadex (for rocuronium/vecuronium) | Ventilatory support |
| Bupivacaine | IV lipid emulsion (Intralipid 20%) | CPR + lipid rescue |
Opioid Death Medicolegal Investigation
CLINICAL PEARL
Normal post-mortem blood glucose does NOT exclude insulin homicide — C-peptide is the forensic anchor. In a suspected insulin poisoning case (coma, very low antemortem blood glucose, possible homicidal circumstances), the critical forensic test is the C-peptide level relative to insulin level. Endogenous hypoglycaemia (insulinoma) shows HIGH C-peptide with HIGH insulin. Exogenous insulin administration shows HIGH insulin with LOW or UNDETECTABLE C-peptide. This ratio is the only reliable biochemical way to distinguish natural from artificial hypoglycaemia — and it is why the blood must be collected immediately and sent to a forensic reference laboratory.
SELF-CHECK
At post-mortem of a 50-year-old woman found dead at home with no external injuries, femoral blood glucose is 1.2 mmol/L. Her husband says she was a diabetic 'who occasionally miscalculated her insulin dose'. Serum insulin is 180 mU/L (reference <25 mU/L) and C-peptide is undetectable. What is the most accurate forensic interpretation?
A. Consistent with an insulinoma (beta-cell tumour) causing endogenous insulin hypersecretion
B. Consistent with exogenous insulin administration — the absent C-peptide with elevated insulin indicates insulin was injected (not endogenously produced)
C. Post-mortem hypoglycaemia is artefactual; insulin levels are always high post-mortem; no forensic conclusion possible
D. Normal variation — C-peptide can be absent in diabetic patients on long-term insulin therapy
Reveal Answer
Answer: B. Consistent with exogenous insulin administration — the absent C-peptide with elevated insulin indicates insulin was injected (not endogenously produced)
Endogenous insulin is always co-secreted with C-peptide in equimolar amounts (proinsulin cleavage). Exogenous insulin injections contain NO C-peptide. A finding of very high insulin (180 mU/L) with ABSENT C-peptide strongly indicates exogenous insulin administration — consistent with insulin homicide in this suspicious context. An insulinoma would show HIGH C-peptide with high insulin. Post-mortem glucose is unreliable (always falls post-mortem) but the insulin:C-peptide ratio is the forensic anchor. Long-term insulin therapy does not eliminate endogenous C-peptide — the pancreas continues to secrete its own insulin (and C-peptide) unless it is totally ablated (type 1 diabetes for >10 years may have near-zero C-peptide, but this must be documented in the clinical history).