Page 23 of 33
FM13.19 | Snake Bite, Stings & Envenomation — SDL Guide
Learning Objectives
- Identify the four medically important snake families in India and their characteristic envenomation syndromes
- Describe the pathological basis of haemotoxic vs neurotoxic envenomation and their clinical distinction
- Apply the antivenom administration protocol, including dose determination and management of antivenom reactions
- Describe the clinical features and management of scorpion sting, bee/wasp sting, and spider bite
- Prepare a medicolegal report for envenomation death, including post-mortem sampling
INSTRUCTIONS
Envenomation — by snakes, scorpions, bees, and spiders — represents an important cause of death in rural India. India has the highest snakebite mortality in the world, with an estimated 58,000 deaths annually. Forensic medicine graduates encounter envenomation deaths in the post-mortem room and as causes of compensation or medicolegal claims. This SDL builds the clinical recognition skills and treatment knowledge needed for both urgent clinical management and accurate forensic certification.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 40-year-old farmer in Andhra Pradesh is brought to the taluk hospital at midnight, carried by his family. They found him unconscious in the field two hours ago. They report he cried out suddenly and collapsed. On examination, he has ptosis, difficulty swallowing, and his respiratory rate is down to 6 breaths/minute. There is a double fang mark on his right ankle. There is no local swelling, no haemorrhage, and his gums appear normal. In the mortuary the same night, another farmer brought in dead has haemorrhagic post-mortem lividity, blood oozing from the bite site, and purpuric skin lesions. Two snake deaths. Two completely different mechanisms. How do you manage the living patient, and how do you certify the deceased?
WHY THIS MATTERS
India accounts for nearly half of global snakebite deaths. The four medically important snakes — the 'Big Four' — are responsible for almost all venomous snakebite deaths and are distributed across India. Forensic medicine graduates must be able to distinguish neurotoxic from haemotoxic envenomation, administer appropriate antivenom, and document envenomation deaths medicolegally. Beyond snakes, scorpion stings (particularly in Maharashtra, Rajasthan, and Andhra Pradesh) and bee/wasp attacks (mass casualty events during swarming season) are forensically significant. This SDL is directly applicable to the first clinical posting.
RECALL
Recall from Year 1:
- Neuromuscular junction physiology: motor neurone → acetylcholine → nicotinic NMJ receptor (opens Na⁺ channel → end-plate potential → muscle contraction). Pre-synaptic block (β-bungarotoxin — prevents ACh release) vs post-synaptic block (α-bungarotoxin, curare — block the nicotinic receptor) both cause flaccid paralysis.
- Haemostasis (clotting cascade): the extrinsic (tissue factor + FVII) and intrinsic (contact factors → FVIII/IX) pathways converge at Factor X → prothrombin → thrombin → fibrinogen → fibrin. Viper venoms contain phospholipases and proteases that either activate or consume clotting factors → disseminated intravascular coagulation (DIC) or direct fibrinogenolysis.
- Complement system and anaphylaxis: type I hypersensitivity — IgE-mediated degranulation of mast cells/basophils → histamine, leukotrienes → vasodilation, bronchospasm, oedema. Relevant for bee/wasp sting allergy.
- Rhabdomyolysis: breakdown of striated muscle (sarcolemmal damage) → myoglobin release → myoglobinuria → acute tubular necrosis → renal failure. Russell's viper venom directly damages muscle (myotoxicity).
Medicolegal Context: Snakebite Deaths in India
Snakebite is one of the few causes of poisoning death where the forensic medicine specialist may be the only person in the chain who can correctly identify the causative organism and mechanism — because the snake may be long gone by the time the body reaches the mortuary. Several medicolegal dimensions arise:
Certification of cause of death: The post-mortem findings of envenomation are often non-specific. Neurotoxic snake deaths show pulmonary oedema and respiratory failure changes. Haemotoxic deaths show DIC, haemorrhagic petechiae, and haemorrhage at multiple sites. Without a history of snake bite, these may be misattributed to natural causes (heart failure, haematological disorder). The forensic doctor must specifically look for fang marks.
Compensation and insurance claims: In India, snakebite death of a breadwinner in a farming family may entitle the family to government compensation. Fraudulent claims of death by snakebite (concealing a natural cardiac death) or genuine misclassification of snakebite as natural death both require forensic clarification.
Homicidal envenomation (rare): Deliberately introducing venom (using the live snake, extracted venom, or venom-soaked objects) has been documented in Indian homicide cases. The forensic doctor must consider this possibility in an unexplained envenomation death, particularly if the social context suggests it (domestic disputes, inheritance disputes).
PM examination protocol for suspected envenomation:
- Careful examination of the entire body surface for fang marks (may be small and easily missed — 0.5–1 cm apart for most Indian vipers; may be single if one fang struck)
- Photograph fang marks with scale
- Collect blood for toxicological analysis (ELISA-based venom identification kits are available at reference labs)
- Examine internal organs for DIC changes (haemorrhages in multiple organs)
- Note presence/absence of local tissue necrosis at bite site
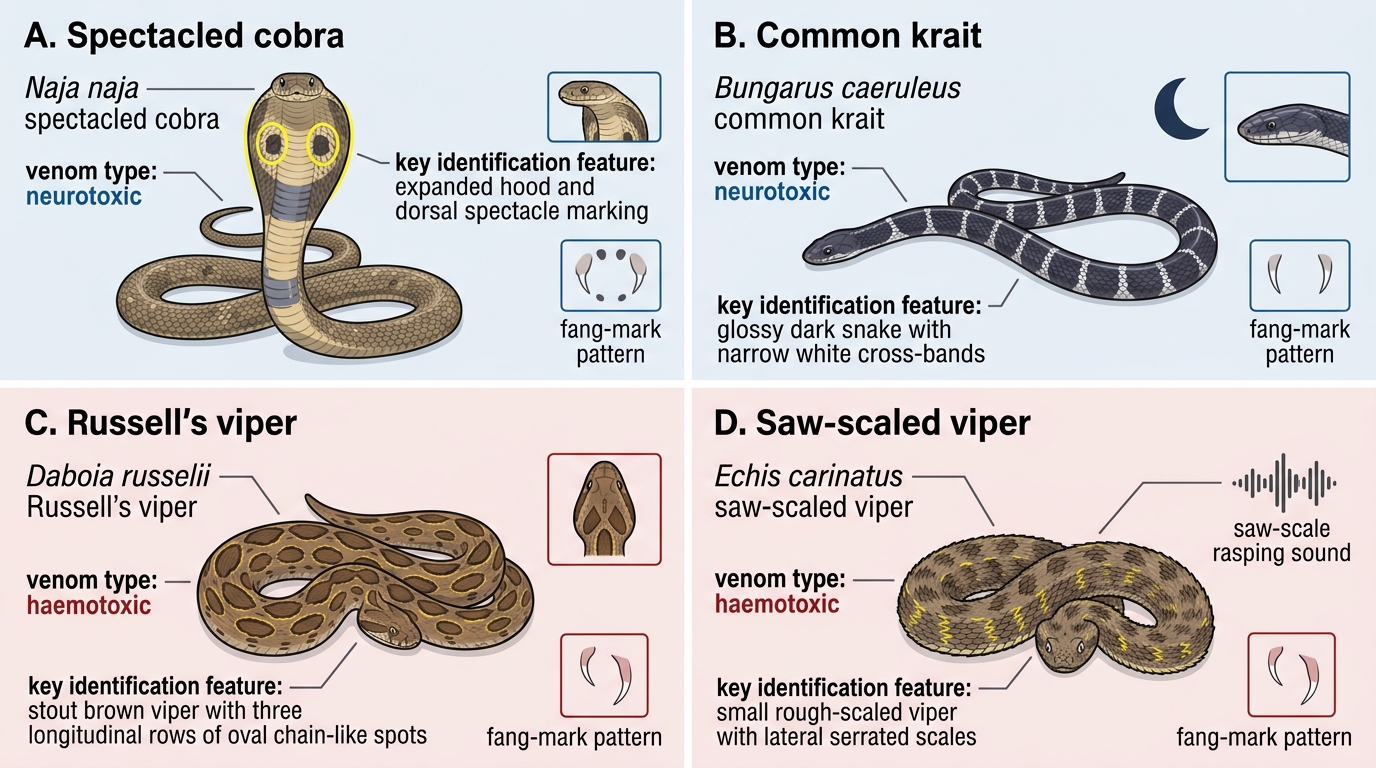
Identification Chart of Four Medically Important Indian Snakes
The Big Four: Indian Medically Important Snakes
The four medically important snakes responsible for the vast majority of serious snakebite in India are: Russell's viper (Daboia russelii), Indian cobra (Naja naja), common krait (Bungarus caeruleus), and saw-scaled viper (Echis carinatus). Understanding their venom types determines both the clinical syndrome and the management approach.
HAEMOTOXIC ENVENOMATION:
Russell's viper (Daboia russelii) is the most dangerous snake in India in terms of both venom potency and clinical complexity. Its venom contains:
- Serine proteases: directly activate prothrombin and Factor X → venom-induced consumption coagulopathy (VICC)
- Phospholipase A2 (PLA2): myotoxic (rhabdomyolysis), nephrotoxic (direct tubular damage), and haemolytic
- Metalloproteinases: local tissue necrosis
Clinical features: local swelling/haemorrhage, DIC (bleeding from bite site + systemic haemorrhage — gum bleeding, haematuria, haematemesis), acute renal failure (a characteristic complication of Russell's viper — direct nephrotoxicity + haemolysis + rhabdomyolysis), hypopituitarism (Sheehan-like pituitary haemorrhage — a unique feature of Russell's viper).
Saw-scaled viper (Echis carinatus) — primarily haemotoxic; causes DIC and haemorrhagic syndrome; the rasping sound of its scales rubbing is the characteristic pre-strike sound.
NEUROTOXIC ENVENOMATION:
Indian cobra (Naja naja): venom contains alpha-neurotoxins (post-synaptic nicotinic receptor block — competitive; similar to d-tubocurarine) and cytotoxins (local necrosis). Features: local significant swelling and necrosis + neurotoxic paralysis (post-synaptic block → may partially respond to anticholinesterase therapy — neostigmine + atropine).
Common krait (Bungarus caeruleus): the most neurotoxically dangerous snake. Venom contains:
- Beta-bungarotoxin (pre-synaptic): irreversibly destroys ACh vesicle release machinery at the NMJ → motor end-plate cannot release ACh → flaccid paralysis. PRE-synaptic block does NOT respond to neostigmine (no ACh to release even if AChE is blocked).
- Alpha-bungarotoxin (post-synaptic): irreversibly binds nicotinic receptor.
Classic krait scenario: nocturnal bite while sleeping (krait active at night) → patient wakes with minimal local signs, painless bite, profound ptosis + dysphagia + respiratory paralysis. The absence of significant local signs in a paralysed patient is the krait's forensic signature.
Comparison of neurotoxic snakes — cobra vs krait:
| Feature | Cobra | Krait |
|---|---|---|
| Local signs | Significant (necrosis, swelling) | Minimal |
| Bite time | Daytime | Nocturnal |
| Neostigmine response | Partial (post-synaptic) | None (pre-synaptic) |
| Key toxin | α-neurotoxin (post-synaptic) | β-bungarotoxin (pre-synaptic) |
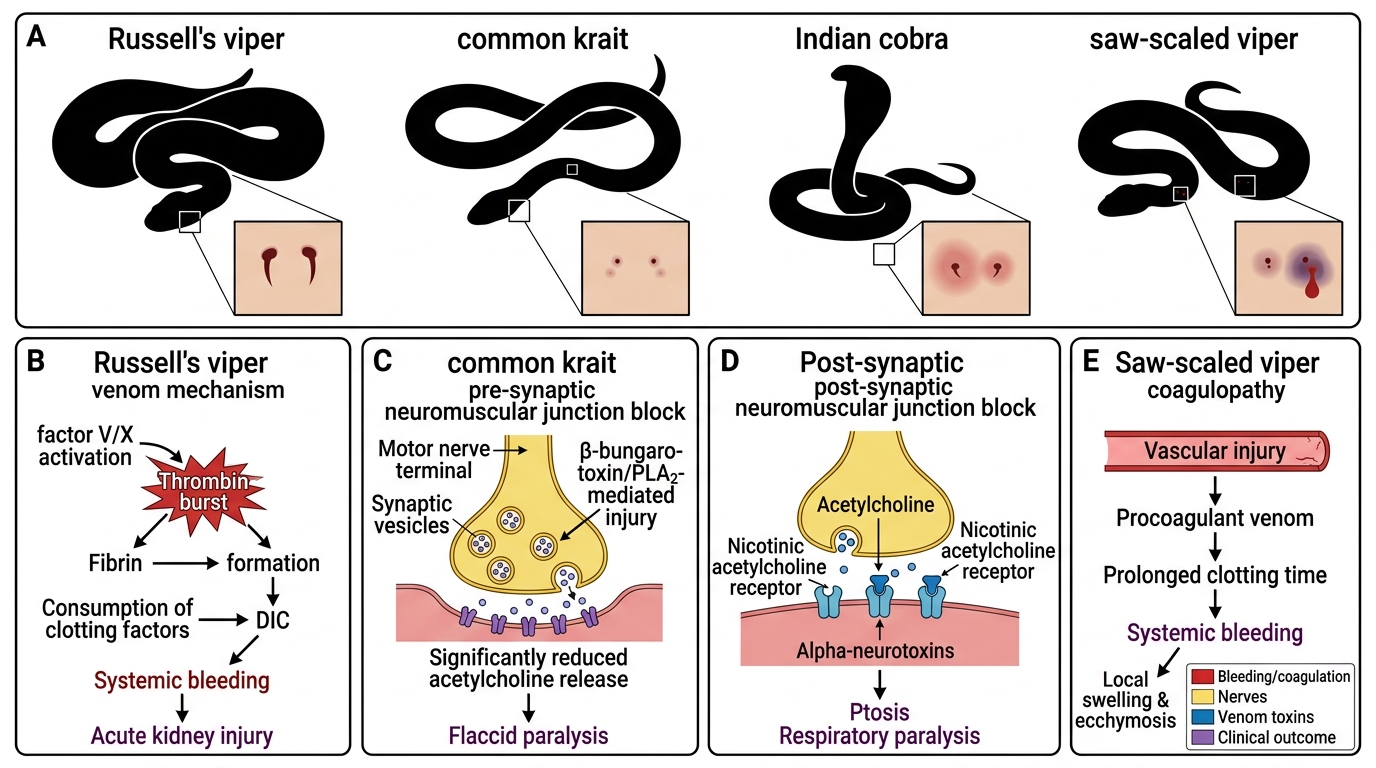
Big Four Indian Snakes: Bite Marks and Venom Mechanisms
SELF-CHECK
A patient with a nocturnal krait bite presents with respiratory failure and bilateral ptosis but almost no local swelling or pain. IV neostigmine + atropine is tried — there is no improvement in muscle power. The most correct explanation is:
A. The dose of neostigmine was too low — higher doses reverse krait neurotoxin
B. Beta-bungarotoxin from krait venom causes pre-synaptic destruction of ACh release machinery — no ACh can be released, so blocking AChE is ineffective
C. Neostigmine is contraindicated in snake bite — atropine alone should be used
D. Krait neurotoxin is a muscarinic (not nicotinic) blocker, explaining why atropine does not reverse it
Reveal Answer
Answer: B. Beta-bungarotoxin from krait venom causes pre-synaptic destruction of ACh release machinery — no ACh can be released, so blocking AChE is ineffective
Beta-bungarotoxin destroys the presynaptic ACh vesicle release mechanism at the NMJ — there is no acetylcholine available to release, so even if AChE is blocked by neostigmine, no ACh accumulates. This distinguishes krait pre-synaptic block from cobra post-synaptic block (alpha-neurotoxin competitively blocks the nicotinic receptor — here, neostigmine-induced ACh accumulation can partially overcome the competitive block). Krait neurotoxin acts on nicotinic (not muscarinic) receptors. Management for krait paralysis is ventilatory support until the pre-synaptic terminals recover.
Antivenom Protocol and Management
Polyvalent antivenom (PAV) — also called anti-snake venom (ASV) — covers all four of the Big Four Indian snakes. It is the only specific treatment for serious envenomation. The WHO supports polyvalent antivenom as the standard for India.
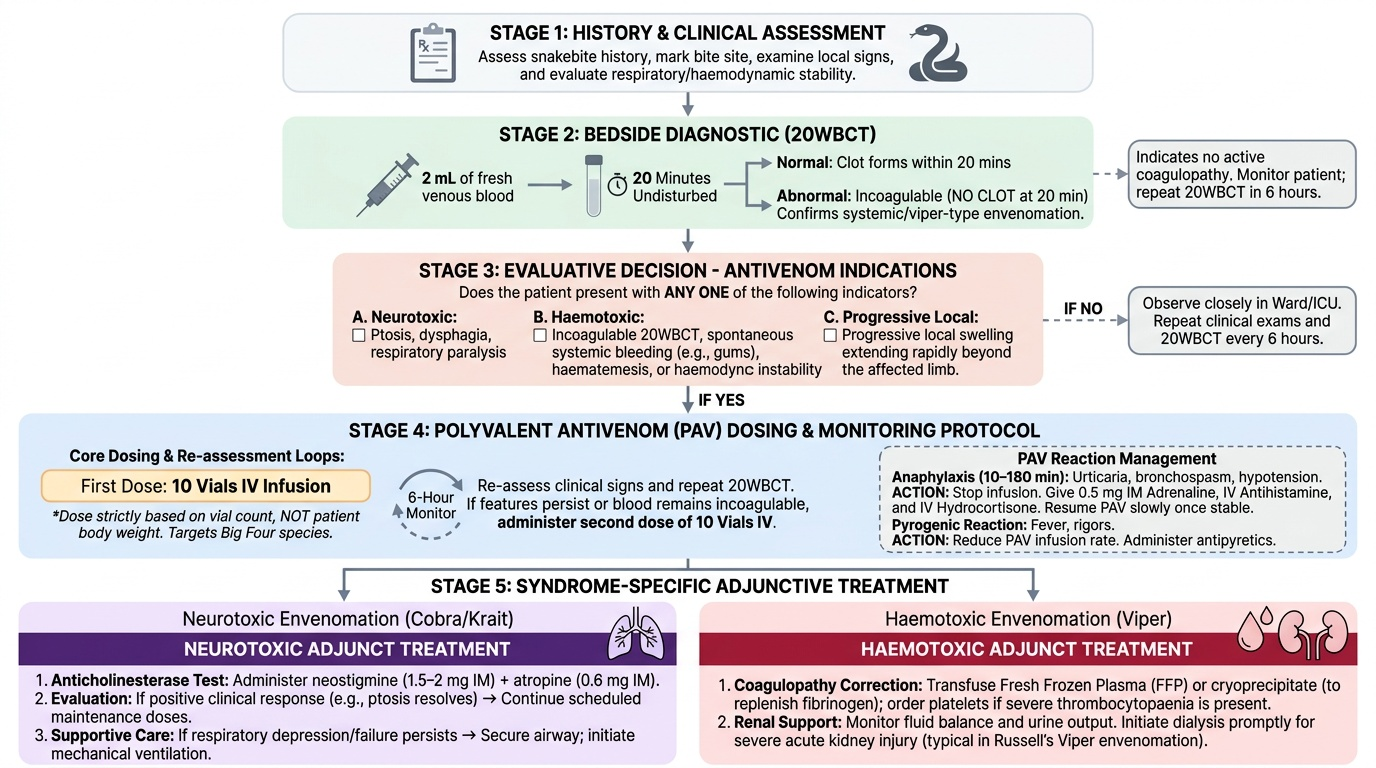
Indications for antivenom (any ONE is sufficient):
- Signs of systemic envenomation: neurotoxic features (ptosis, dysphagia, respiratory paralysis), coagulopathy (20-minute whole blood clotting test — 20WBCT — shows incoagulability), haemorrhagic features (gum bleeding, haematuria, haematemesis)
- Haemodynamic instability
- Progressive local swelling extending beyond the limb
Dose:
The dose of antivenom in India is 10 vials IV for significant envenomation (both mild and severe), repeated at 6-hour intervals if envenomation features persist. Indian antivenom is dosed by the number of vials (each vial typically neutralises a defined amount of venom) — NOT by body weight. This is a critical difference from some other countries' protocols.
20-Minute Whole Blood Clotting Test (20WBCT):
Place 2 mL of fresh venous blood in a clean, dry glass tube; leave undisturbed for 20 minutes. Normal result: clot forms (blood coagulates within 8–10 min normally). Incoagulable blood (no clot at 20 min) = significant viper envenomation. The 20WBCT is used at the bedside in resource-limited settings to confirm viper-type envenomation and guide antivenom dosing. Repeat the test 6 hours after each antivenom dose.
Antivenom reactions — recognition and management:
- Early anaphylaxis (within 10–180 min of starting): urticaria, bronchospasm, hypotension. Treat: stop antivenom, 0.5 mg IM adrenaline (epinephrine), IV antihistamine (chlorphenamine), IV hydrocortisone. Once anaphylaxis controlled, recommence antivenom slowly with premedication.
- Pyrogenic reaction (fever, rigors): slowing the infusion rate usually manages this.
Specific supplementary treatments:
Neurotoxic envenomation (cobra):
- Anticholinesterase test (neostigmine 1.5–2 mg IM + atropine 0.6 mg IM): if clinical improvement in ptosis/respiratory function → continue with scheduled neostigmine doses
- Ventilatory support if respiratory failure
Haemotoxic envenomation (viper):
- Correct coagulopathy: FFP, cryoprecipitate (to replenish consumed fibrinogen); platelet transfusion if thrombocytopaenia severe
- Dialysis for acute renal failure (Russell's viper)
- Do NOT give heparin (it worsens viper-induced coagulopathy)
General:
- Immobilise the affected limb (reduces lymphatic spread of venom)
- Remove rings, tight clothing from bitten limb
- IV fluids, analgesia
- Tetanus prophylaxis
First-aid DON'Ts:
- DO NOT cut and suck the bite
- DO NOT apply tourniquet (worsens local ischaemia; increases compartment syndrome risk with local tissue necrosis)
- DO NOT apply ice
Provided image
SELF-CHECK
A patient bitten by a Russell's viper has gum bleeding, haematuria, and a 20WBCT showing incoagulable blood at 20 minutes. Ten vials of polyvalent antivenom IV are given. Six hours later, the 20WBCT is repeated and blood is STILL incoagulable. The MOST appropriate action is:
A. Give heparin to prevent further DIC progression
B. Give a further 10 vials of antivenom IV
C. Transfuse FFP and platelets only — antivenom is no longer effective after the first dose
D. Reassure — the 20WBCT takes 24 hours to normalise after a single antivenom dose
Reveal Answer
Answer: B. Give a further 10 vials of antivenom IV
Persisting incoagulability at 6 hours post-antivenom indicates that the initial dose was insufficient to neutralise all the venom (or ongoing absorption of venom from the bite site). The WHO/Indian protocol recommends repeating the same dose (10 vials) every 6 hours until the 20WBCT normalises. Heparin is CONTRAINDICATED in viper DIC — it worsens the coagulopathy. FFP/platelets are supportive but do not address the root cause (ongoing venom-mediated clotting factor consumption). The 20WBCT should normalise within 6 hours of an effective antivenom dose — persistent incoagulability means more antivenom is needed.
Scorpion Sting, Bee/Wasp Sting, Spider Bite and Medicolegal Reporting
SCORPION STING:
In India, the red scorpion (Mesobuthus tamulus) of Maharashtra and parts of Andhra Pradesh and Rajasthan is the most dangerous species. Its venom contains scorpion toxins that act on voltage-gated Na⁺ channels (similar to aconitine) — preventing channel inactivation → massive autonomic storm (parasympathetic and sympathetic excessive discharge simultaneously).
Clinical features — the 'autonomic storm':
- Early: intense local pain at the sting site; sweating, salivation, lacrimation (parasympathetic surge)
- Cardiovascular: hypertension, tachycardia → then bradycardia, hypotension, myocardial failure (catecholamine-induced cardiomyopathy)
- Children particularly vulnerable: pulmonary oedema, CNS toxicity
Treatment: prazosin (alpha-1 blocker) is the specific treatment for Indian red scorpion — it counteracts the alpha-adrenergic vascular constriction and reduces the cardiovascular toxicity. Supportive care; no antivenom universally available in India for red scorpion (some states have scorpion antivenom). Pain management (local ice, oral analgesics).
BEE AND WASP STING:
Single sting: local histamine-mediated response; rarely systemic. Managed with antihistamines, ice.
Anaphylaxis to bee/wasp venom (IgE-mediated, type I hypersensitivity): LIFE-THREATENING; even a single sting in a sensitised individual. Features: generalised urticaria, angioedema, bronchospasm, cardiovascular collapse within minutes.
Treatment: IM adrenaline (epinephrine) 0.5 mg is the first-line and most critical intervention; IV antihistamine + hydrocortisone; IV fluids; airway management. Adrenaline must be given IM (not SC, not IV unless cardiac arrest) in anaphylaxis — IM has more predictable absorption and faster peak effect.
Mass attack (>50 stings) — even non-allergic individuals develop systemic toxicity (direct venom effect: haemolysis, renal failure, coagulopathy). Treated with supportive care.
SPIDER BITE:
Most common spiders of medical significance in India:
- Black widow spider (Latrodectus species): venom = alpha-latrotoxin → massive ACh release at NMJ → severe muscle cramps (especially abdominal, regional), sweating, hypertension, tachycardia. Treatment: IV calcium gluconate for muscle cramps; antivenom available in some countries (not routinely in India).
- Brown recluse (Loxosceles): rare in India; venom causes local necrotic wound (loxoscelism); systemic haemolysis in severe cases.
Medicolegal reporting for envenomation death:
The MLR and death certificate must specify:
- The likely species (based on clinical syndrome, geographical distribution, and identification of the snake/scorpion if possible)
- The mechanism of death (respiratory failure from neurotoxic envenomation; cardiovascular collapse from haemotoxic DIC; anaphylaxis from bee sting)
- Whether appropriate treatment was sought and given (for compensation claims and negligence cases)
- Any first-aid that may have contributed to worse outcome (tourniquet-induced ischaemia is a notable example)
Statutory context:
- Compensation for snakebite deaths is available under various state government welfare schemes for farmers
- IPC §304A (criminal negligence) may apply if a hospital failed to stock antivenom or administer it correctly in a case that resulted in preventable death
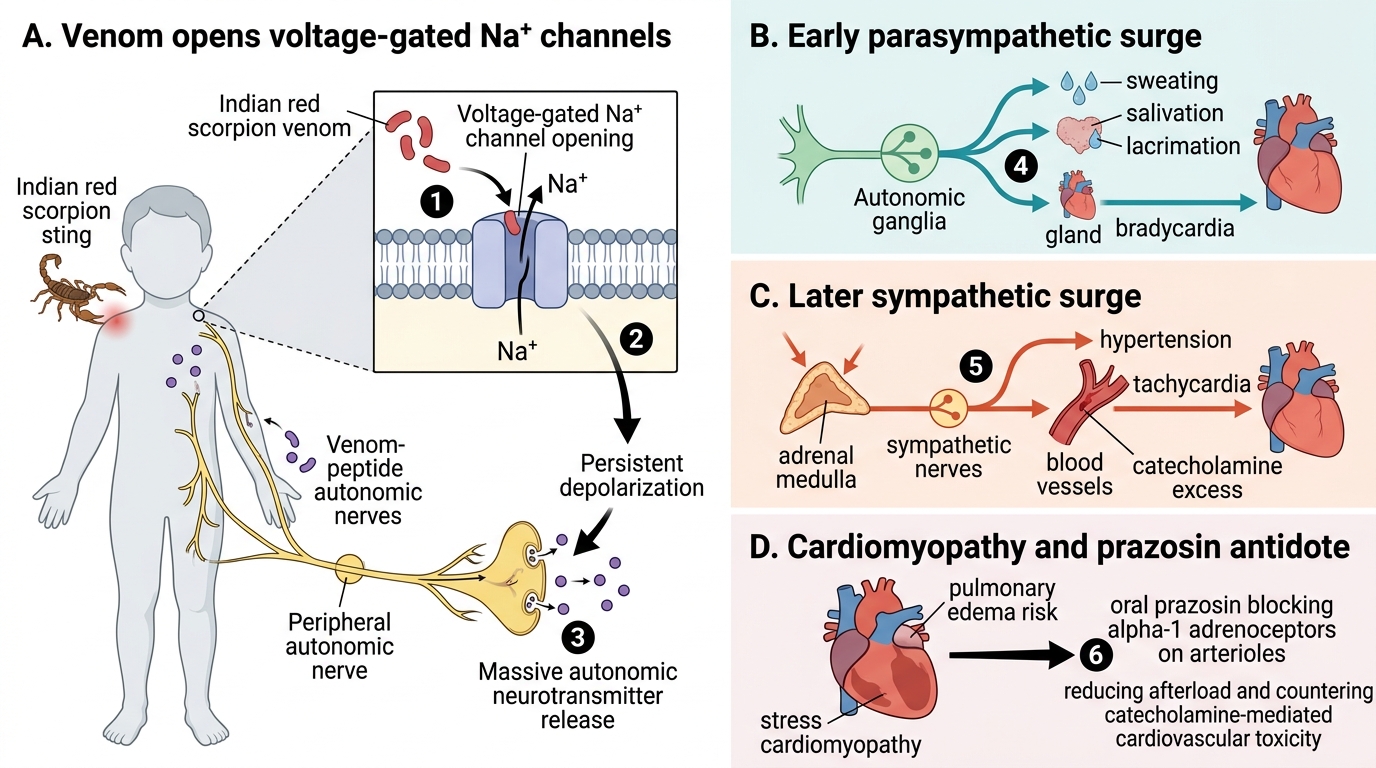
Indian Red Scorpion Venom: Autonomic Storm and Prazosin Action
CLINICAL PEARL
The 20-Minute Whole Blood Clotting Test (20WBCT) is the most important bedside test in the snakebite ward. It requires only a clean, dry glass tube and fresh blood — no laboratory, no electricity. Incoagulable blood at 20 minutes = viper envenomation; coagulable blood does not exclude envenomation (neurotoxic snakes do not affect coagulation). The test also serves as the antivenom monitoring tool: a normalising 20WBCT confirms adequate antivenom neutralisation; persisting incoagulability mandates another 10-vial dose. This test is a fundamental skill for every doctor in India.
SELF-CHECK
A 6-year-old child is brought to the hospital 1 hour after a scorpion sting on the right hand. He has profuse sweating, lacrimation, and blood pressure of 180/120 mmHg with tachycardia. The appropriate specific pharmacological treatment for Indian red scorpion (Mesobuthus tamulus) envenomation is:
A. IV atropine — to reverse the excessive parasympathetic (cholinergic) discharge
B. Prazosin oral — alpha-1 adrenoceptor blocker to counteract catecholamine-mediated hypertension and cardiovascular toxicity
C. IV adrenaline — to reverse the bradycardia and hypotension
D. IV calcium gluconate — as a direct antidote to scorpion toxin
Reveal Answer
Answer: B. Prazosin oral — alpha-1 adrenoceptor blocker to counteract catecholamine-mediated hypertension and cardiovascular toxicity
Indian red scorpion (Mesobuthus tamulus) venom causes an autonomic storm — simultaneous parasympathetic AND sympathetic excess. The cardiovascular toxicity (hypertension → catecholamine-induced cardiomyopathy → myocardial failure) is mediated by alpha-adrenergic receptor stimulation from catecholamine surge. Prazosin (an alpha-1 blocker) is the specific evidence-based treatment, particularly effective in children. Atropine alone addresses only the parasympathetic component (inadequate). IV adrenaline would worsen the initial hypertensive phase. IV calcium gluconate is for hypo-calcaemia or black widow spider cramps.
KEY TAKEAWAYS
Envenomation (FM13.19) is dominated by snakebite in India, with two main syndromes:
Haemotoxic (viper — Russell's and saw-scaled): DIC, haemorrhage, acute renal failure, local necrosis. Diagnosis by 20WBCT (incoagulable blood). Treatment: 10 vials polyvalent antivenom IV, repeat 6-hourly until 20WBCT normalises. No heparin. FFP for coagulopathy support.
Neurotoxic (cobra and krait): flaccid paralysis, respiratory failure. Cobra = post-synaptic block (neostigmine may partially reverse). Krait = pre-synaptic block (irreversible, no neostigmine response). Treatment: antivenom + mechanical ventilation. Minimal local signs = krait signature.
Scorpion (red scorpion, Maharashtra): autonomic storm → hypertension then cardiomyopathy. Treatment: prazosin (alpha-1 blocker).
Bee/wasp sting anaphylaxis: IM adrenaline 0.5 mg first-line.
Forensic principles: search for fang marks at every PM; specify mechanism of death; collect blood for ELISA-based venom identification.
REFLECT
You are examining the body of a 30-year-old farmer who was found dead in his field at dawn. The family insists it was a heart attack. There is a small double-puncture mark on his left leg. There are scattered petechiae over the trunk and the blood oozing from the bite site has not clotted. Describe your approach to this post-mortem examination and the evidence you would collect to establish snakebite as the cause of death. How would you approach the family's insistence on 'heart attack' — and what are your legal obligations regarding cause of death certification if you find evidence of envenomation?