Page 18 of 33
FM13.17 | Therapeutic Drug Overdose: Antipyretics, Anti-infectives & Neuropsychotropics — SDL Guide (Part 2)
Tricyclic Antidepressants, Neuroleptics and Haloperidol
TRICYCLIC ANTIDEPRESSANTS (TCAs) — amitriptyline, imipramine, nortriptyline, clomipramine:
TCAs remain a common cause of serious drug overdose fatality despite newer antidepressants being available. They are particularly dangerous because they combine multiple toxic mechanisms:
- Fast sodium channel blockade (quinidine-like effect on the His-Purkinje system): QRS widening → ventricular arrhythmia (most common cause of death). QRS >100 ms = significant risk; >160 ms = high risk of arrhythmia.
- Alpha-1 adrenoceptor blockade: hypotension (vasodilation)
- GABA-A receptor antagonism: seizures (paradoxical for a CNS depressant — TCAs lower the seizure threshold)
- Muscarinic receptor antagonism (anticholinergic): dry mouth, urinary retention, tachycardia, confusion, dilated pupils (anticholinergic toxidrome)
The combination of QRS widening + hypotension + anticholinergic features + seizures = TCA overdose until proven otherwise.
Treatment:
- IV sodium bicarbonate (alkalinisation) — the specific intervention for TCA-induced wide-complex arrhythmia; sodium loading (not the alkalosis per se) reverses Na⁺ channel blockade; target blood pH 7.45–7.55
- Benzodiazepines for seizures
- IV lipid emulsion (intralipid 20%) — 'lipid rescue' for refractory TCA toxicity (highly lipophilic drugs redistribute into the lipid phase)
- No specific antidote; DO NOT use physostigmine (anticholinesterase reversal) in TCA overdose — may cause asystole in the context of cardiac Na⁺ channel blockade
HALOPERIDOL and NEUROLEPTICS (antipsychotics):
Haloperidol (typical antipsychotic, D2 antagonist), olanzapine, risperidone, quetiapine (atypical antipsychotics). In overdose:
- QTc prolongation → risk of torsades de pointes (polymorphic ventricular tachycardia)
- Extrapyramidal effects (acute dystonia, akathisia) may be prominent
- Alpha-1 blockade → hypotension
- Neuroleptic malignant syndrome (NMS): a specific toxidrome from antipsychotics (can occur at therapeutic doses) — hyperthermia, rigidity, autonomic instability, altered consciousness; NOT an overdose phenomenon per se but covered here as part of antipsychotic toxicology
Treatment: supportive; QTc monitoring; magnesium sulphate for torsades; cooling for NMS; dantrolene for NMS muscle rigidity; bromocriptine (D2 agonist) for NMS.
ANTI-INFECTIVES:
For the purposes of FM13.17, the competency notes 'anti-infectives (common antibiotics overview)'. Serious antibiotic overdose is uncommon but the forensic doctor should know:
- Aminoglycosides (gentamicin, amikacin): narrow therapeutic index; nephrotoxic + ototoxic in overdose or with impaired renal clearance
- Isoniazid (INH) overdose: competitive pyridoxine antagonism → seizures refractory to standard anticonvulsants; antidote is IV pyridoxine (vitamin B6) at a gram-for-gram dose to estimated INH ingested
- Chloramphenicol: 'grey baby syndrome' in neonates (dose-related mitochondrial toxicity)
These are forensically relevant in contexts of inadvertent overdose in paediatric patients and in suicidal ingestion by healthcare workers with access to IV preparations.
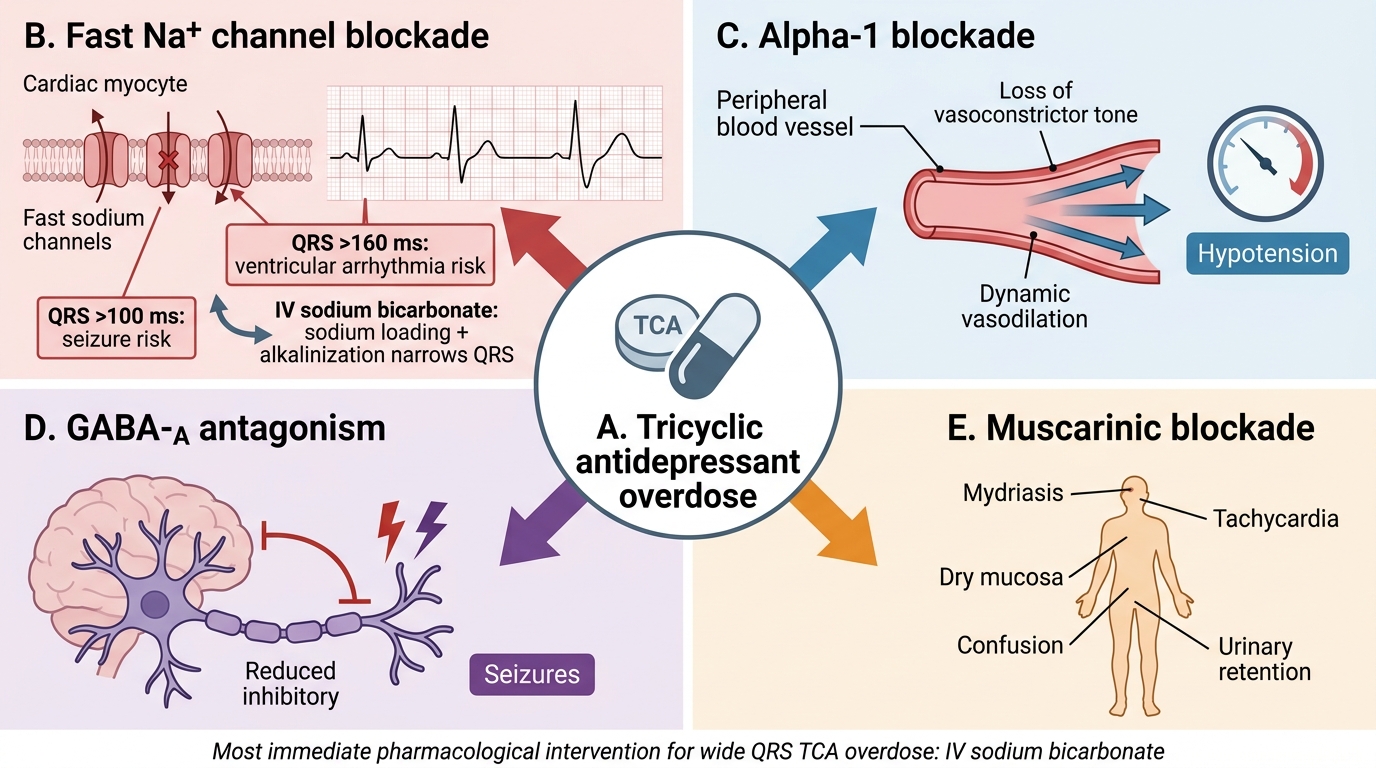
TCA Overdose: Four Toxic Mechanisms
SELF-CHECK
A 19-year-old is brought in after swallowing 'a handful of her mother's antidepressants'. She is confused, has a pulse of 120 bpm, and her ECG shows QRS of 130 ms. Her pupils are dilated and she is hypotensive. The MOST appropriate immediate pharmacological intervention is:
A. IV flumazenil — to reverse benzodiazepine sedation
B. IV sodium bicarbonate — to reverse Na⁺ channel blockade causing QRS widening
C. IV atropine — to treat the bradycardia from vagal overdrive
D. IV neostigmine — to reverse the anticholinergic effects causing tachycardia
Reveal Answer
Answer: B. IV sodium bicarbonate — to reverse Na⁺ channel blockade causing QRS widening
This is tricyclic antidepressant (TCA) overdose — the combination of anticholinergic features (dilated pupils, tachycardia), QRS widening (>120 ms), and hypotension is pathognomonic. The most immediately life-threatening problem is the wide-complex arrhythmia risk from Na⁺ channel blockade. The specific intervention is IV sodium bicarbonate — sodium loading reverses the TCA Na⁺ channel block, narrowing the QRS. Flumazenil reverses benzodiazepines (incorrect mechanism). Atropine is for bradycardia (this patient is tachycardic). Neostigmine (anticholinesterase) would worsen the picture in TCA overdose (risk of cardiac arrest in the context of Na⁺ channel blockade).
Clinical Examination, Documentation and Post-Mortem Approach
Examining a patient with suspected therapeutic drug overdose requires rapid toxidrome identification and systematic documentation of the medicolegal evidence.
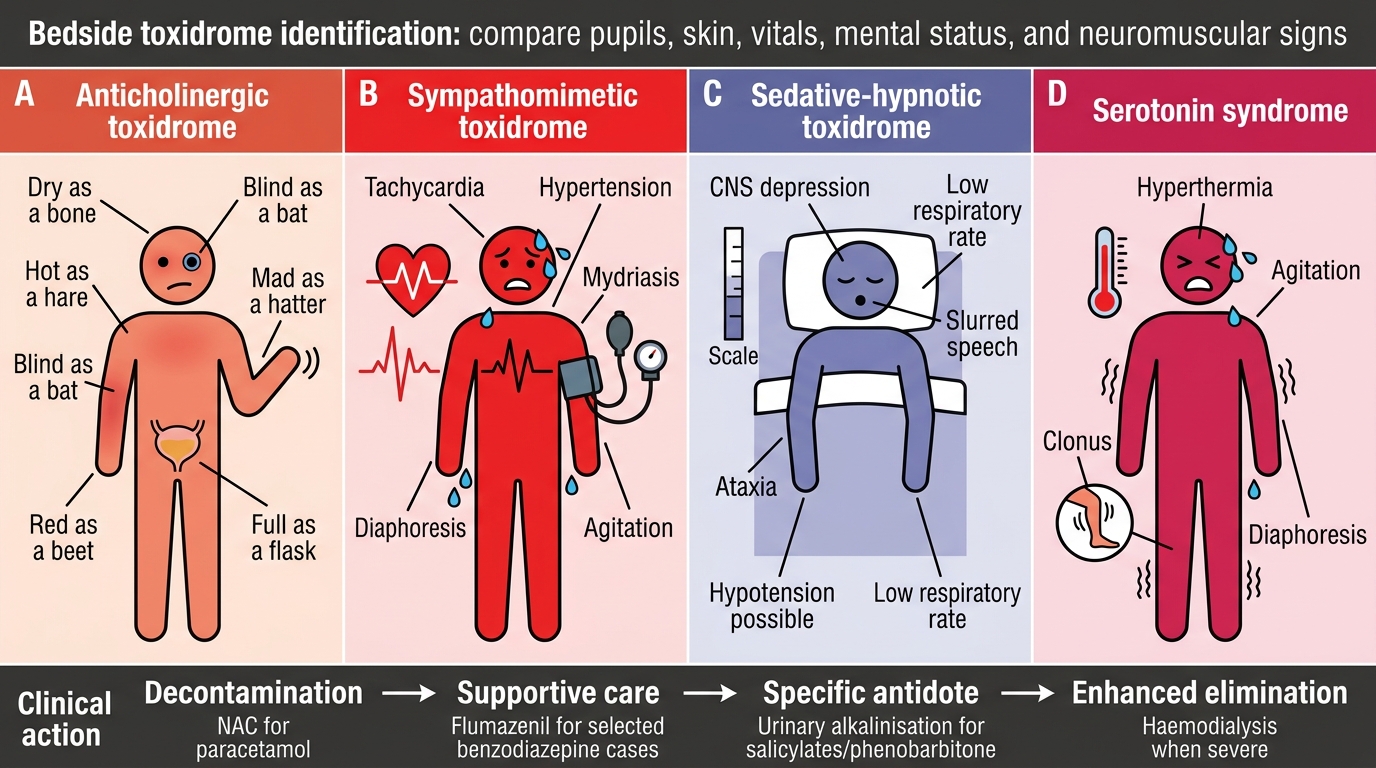
Toxidrome identification at the bedside:
- Anticholinergic (dry, hot, blind, mad, red, full): TCAs, antihistamines, atropine — dilated pupils, dry mouth, urinary retention, tachycardia, confusion, flushed skin
- Cholinergic/SLUDGE: OPs/carbamates (see sp5) — not typically from therapeutic drugs
- Sympathomimetic: cocaine, amphetamines, decongestants — tachycardia, hypertension, diaphoresis, dilated pupils
- Sedative-hypnotic: BZDs, barbiturates, alcohol — sedation, respiratory depression, small pupils (or normal); reflexes depressed
- Opioid: miosis + respiratory depression + sedation — reversed by naloxone
Key ECG changes by drug class:
- QRS widening >100 ms → TCA, Class IA/IC antiarrhythmics
- QTc prolongation → antipsychotics (haloperidol, quetiapine), antibiotics (fluoroquinolones, azithromycin), TCAs
Medicolegal documentation:
Document: the exact drug(s) implicated (generic and brand names), estimated quantity (tablets found, missing from packet), time of last known normal state, circumstances (suicide note, history of psychiatric illness, recent stressors). Preserve any tablet fragments, packets, or liquids found with the patient as forensic exhibits.
Post-mortem approach:
In a death from therapeutic drug overdose:
- Request blood and urine for comprehensive toxicological screening (LC-MS/MS is the standard)
- Liver, vitreous humour, and gastric contents are additional PM specimens
- Liver histology for paracetamol (centrilobular necrosis); cardiac histology for TCA (myocardial degeneration)
- Correlate PM drug levels with clinical history; remember PM redistribution can elevate levels from the antemortem state (particularly for highly lipophilic drugs)
Bedside Identification of Major Drug Overdose Toxidromes
Medicolegal Inference and Treatment Framework
The management framework for therapeutic drug overdose follows the unified toxicology model — decontamination → supportive care → specific antidote → enhanced elimination — with drug-specific applications:
Summary of antidotes and enhanced elimination for this group:
| Drug/class | Specific antidote | Enhanced elimination |
|---|---|---|
| Paracetamol | N-acetylcysteine (NAC) | Haemodialysis for fulminant hepatic failure |
| Salicylates | Urinary alkalinisation | Haemodialysis (salicylate >350 mg/L) |
| Benzodiazepines | Flumazenil | Not needed (supportive ventilation if required) |
| Barbiturates | None | Urine alkalinisation (phenobarbitone); HD |
| TCAs | IV sodium bicarbonate (cardiac) | Lipid emulsion for refractory toxicity |
| Lithium | None (sodium loading promotes excretion) | Haemodialysis (small, water-soluble, not protein-bound) |
| INH | IV pyridoxine (vitamin B6) | — |
| Haloperidol/antipsychotics | None specific; magnesium for torsades | — |
Medicolegal inference:
For suicidal overdose death certification: the cause of death should specify the drug (e.g., 'acute paracetamol hepatotoxicity' or 'amitriptyline-induced cardiac arrhythmia'). If the manner of death (suicide) is in question, note: suicide note, prior attempt history, psychiatric illness, circumstances of discovery, and quantity of drug implicated vs what was prescribed (pharmacy records).
For medication-facilitated crime (sedation of victim): analysis for BZDs/antihistamines in urine/blood of victim; pharmacy investigation to trace the source; and timing analysis (correlate drug levels with alleged time of administration).
IPC sections:
- IPC §328: causing hurt by administering poison — relevant if drug administered without consent
- IPC §302: if death results from deliberate homicidal administration
- IPC §309 (Section 309 CrPC — now effectively decriminalised by MHA 2017): attempted suicide — the Mental Healthcare Act 2017 presumes that a person who attempts suicide is under severe mental stress and must receive care, not punishment
- IPC §304A: negligence causing death — applicable to prescribing errors resulting in death
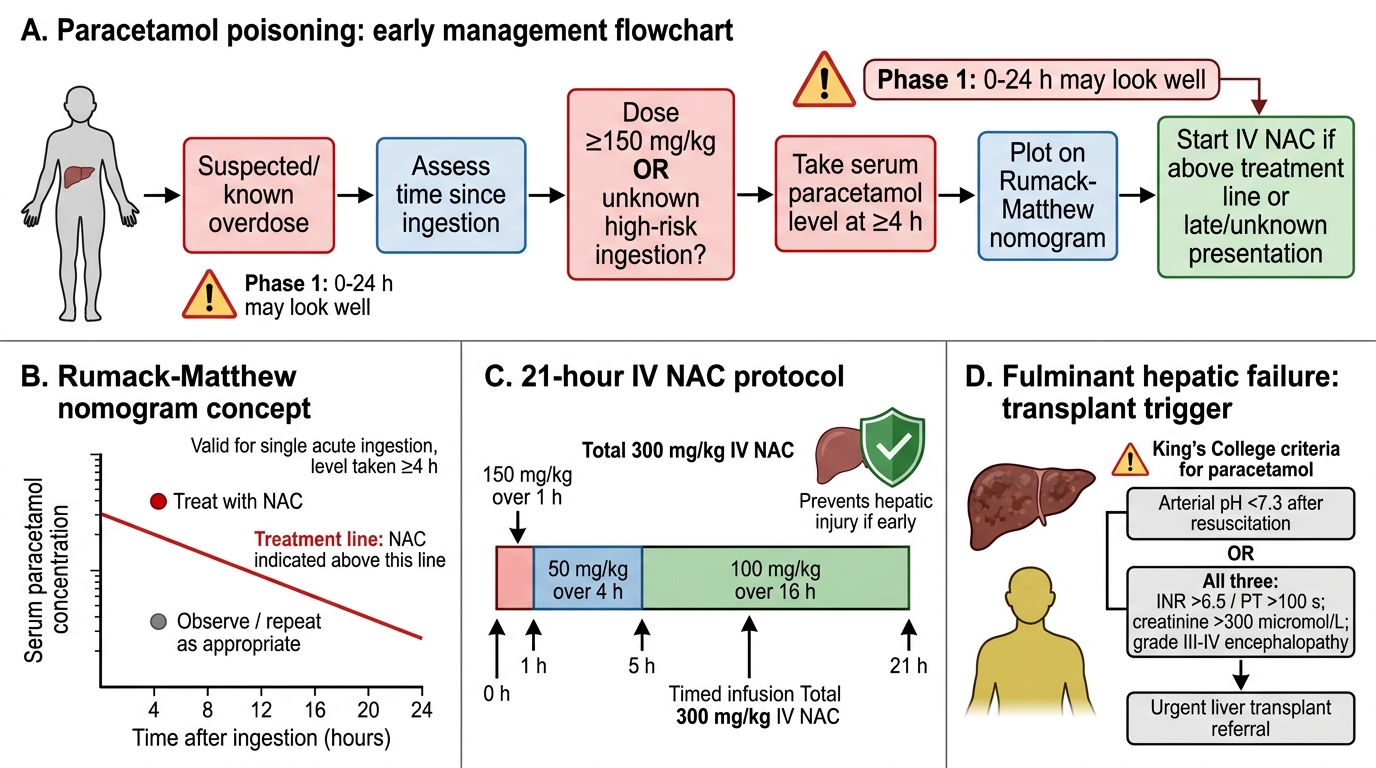
Paracetamol Poisoning Management
CLINICAL PEARL
Paracetamol hepatotoxicity kills the patient who 'looked fine' yesterday. The most dangerous aspect of paracetamol overdose is Phase 1 (0–24 h) apparent wellbeing — patients present, look normal, and may be discharged without NAC if the treating team doesn't know the nomogram. The clinical rule: any patient who has taken ≥150 mg/kg of paracetamol OR whose serum level plots above the Rumack-Matthew treatment line must receive IV NAC regardless of clinical appearance. The asymptomatic patient at 8 hours has exactly the same treatment indication as the jaundiced patient at 72 hours — but the 8-hour patient will recover; the 72-hour patient may already be in fulminant hepatic failure beyond rescue.
SELF-CHECK
A patient with known bipolar disorder on chronic lithium is found confused with a lithium level of 2.8 mEq/L. She has been taking NSAIDs for arthritis for the past 2 weeks. Her serum creatinine is 280 µmol/L. The most appropriate management priority is:
A. IV sodium bicarbonate to alkalinise the urine and increase lithium excretion
B. Stop NSAIDs, provide IV saline (sodium loading to promote lithium excretion), and arrange haemodialysis
C. IV flumazenil to reverse sedation
D. Oral activated charcoal — lithium is well-adsorbed to charcoal
Reveal Answer
Answer: B. Stop NSAIDs, provide IV saline (sodium loading to promote lithium excretion), and arrange haemodialysis
This is chronic lithium toxicity precipitated by NSAID-induced reduction in renal lithium clearance (NSAIDs reduce glomerular filtration and decrease lithium excretion) combined with possible dehydration. Lithium level 2.8 mEq/L with acute renal impairment (creatinine 280) is an indication for haemodialysis — lithium is small, water-soluble, and protein-unbound (ideal dialysis candidate). IV sodium loading (saline) competes with lithium for Na⁺ channels and promotes renal lithium excretion — always first-line. NSAIDs must be stopped. Sodium BICARBONATE alkalinisation is for salicylates/barbiturates, not lithium. Activated charcoal does NOT adsorb lithium (lithium is an inorganic ion — not adsorbed by charcoal).