Page 27 of 33
FM14.{2-3,16} | Toxicology Practical Skills: Clinical Exam, Sampling & Specimen Inference — SDL Guide
Learning Objectives
- Conduct a systematic clinical examination of a patient with suspected poisoning and prepare a medicolegal report (FM14.2)
- Collect, preserve, label, and dispatch forensic exhibits in a suspected poisoning case with proper chain of custody (FM14.3)
- Identify and draw a medicolegal inference from visual specimens of common poisons — dhatura, castor, cannabis, opium, aconite, copper sulphate, pesticides, marking nut, oleander, Nux vomica, abrus seeds, snakes, capsicum, calotropis, lead compounds, and tobacco (FM14.16)
INSTRUCTIONS
This skills SDL integrates the toxicological knowledge from all the specific-poison SDLs of this cluster into practical competencies. FM14.2, FM14.3, and FM14.16 are simulation/supervised skills — they require performance on a real or simulated patient, a real or simulated evidence collection exercise, and visual recognition of poison specimens. This SDL provides the conceptual framework, procedural guide, and specimen recognition knowledge that you must practise in the OSPE and clinical lab setting.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The OSPE examiner places four items in front of you: a jar of a dark blue crystalline substance; a brown seed with a characteristic shape; a seedpod and seeds that look like tiny red-and-black beads; and a yellowish, waxy piece of material smelling faintly of garlic. On the table next to them is a simulated patient who is unconscious, with pinpoint pupils and a garlic odour on the breath. You have 8 minutes to identify all four specimens, state their toxicological significance, and begin the clinical assessment of the simulated patient with dictation into a prepared MLR form. This is what FM14.16 + FM14.2 + FM14.3 look like in practice.
WHY THIS MATTERS
The practical toxicology skills covered in this SDL — clinical examination of the poisoned patient, specimen collection with chain of custody, and visual specimen identification — are exactly what a district hospital doctor or forensic medicine specialist will perform in the first hour of a poisoning case. These are also the most directly examined OSPE skills in the FM professional examination. The visual identification of common Indian plant poisons (FM14.16) is a unique competency that requires deliberate memorisation and practice with real specimens or photographs — it cannot be acquired purely from text.
RECALL
Recall the toxidromes and poison identification clues from across the specific poisons SDLs of this cluster:
- Colour signatures: copper sulphate = blue crystals; arsenic trioxide = white powder; carbon monoxide → cherry-red lividity; nitric acid → yellow staining; carbolic acid → white-then-brown skin; iodine → blue-black mucosal staining
- Odour signatures: phosphorus = garlic; arsenic = garlic; cyanide = bitter almond; phenol/carbolic = characteristic antiseptic phenolic; organophosphates (some) = garlic; phosphine (AlP) = garlic/rotten fish; CO = odourless
- Pupil size: miosis = opioids, OPs/carbamates; mydriasis = anticholinergics (TCA, atropine), cocaine, amphetamines
- Toxidrome taxonomy (from specific SDLs): cholinergic (SLUDGE), anticholinergic (dry/hot/red), sympathomimetic, opioid, serotonin syndrome, sedative-hypnotic
Legal and Professional Context of Toxicology Practical Skills
Forensic medicine practical skills in toxicology exist at the intersection of clinical medicine and legal procedure. Every skill — clinical examination, specimen collection, specimen identification — produces a document or an exhibit that may be presented in court. Understanding this legal context shapes how each step is performed.
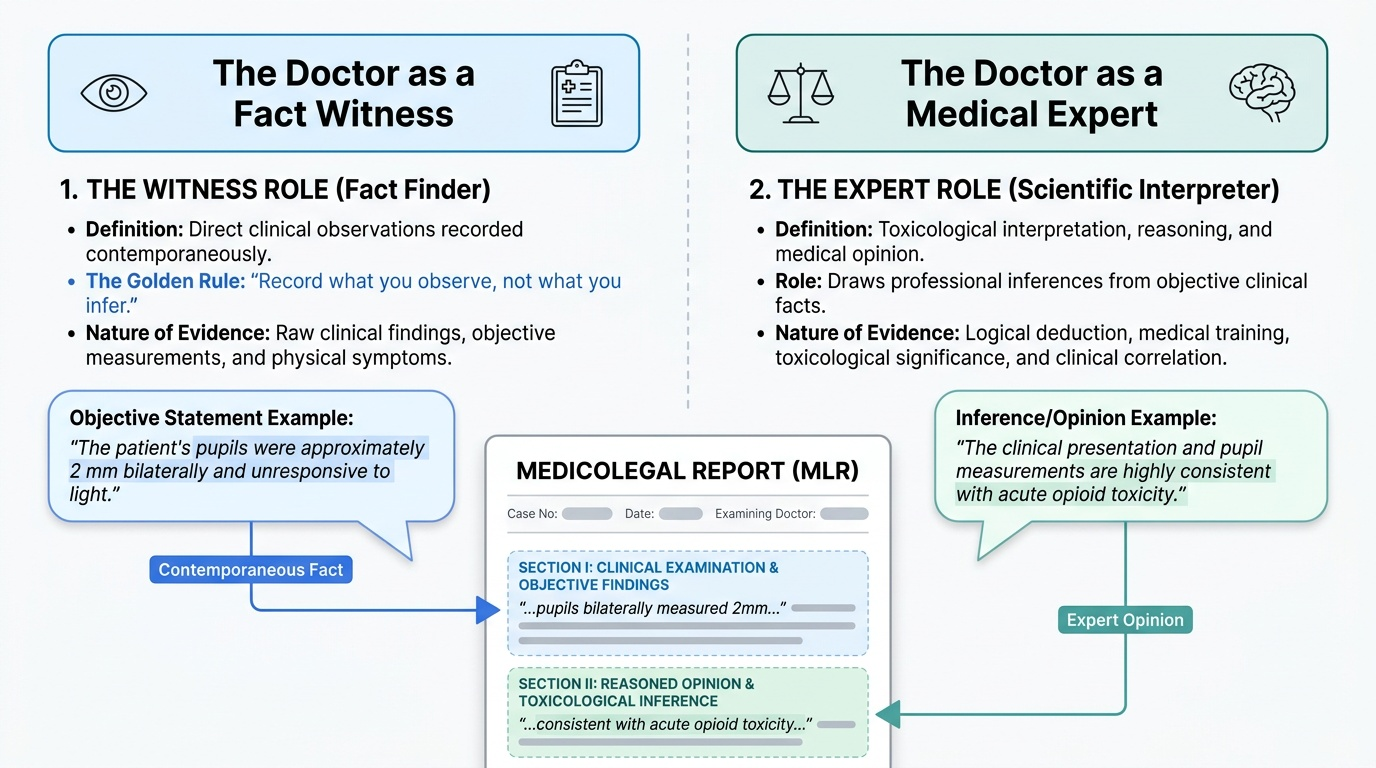
The doctor as witness vs. the doctor as expert:
In a poisoning case, the treating doctor occupies both roles simultaneously: they are a witness to the patient's clinical condition (their own direct observations) AND potentially an expert on the toxicological significance of those findings. The MLR prepared at clinical examination is both a clinical record and a legal document. Its accuracy and completeness are subject to scrutiny in cross-examination.
The golden rule of medicolegal documentation: Record what you observe, not what you infer. Describe findings objectively ('the patient's pupils were approximately 2 mm bilaterally' — not 'the patient was intoxicated with an opioid'). The opinion/inference section of the MLR draws conclusions from those objective findings.
The chain of custody principle (continuity of evidence):
Any specimen collected for forensic analysis is a legal exhibit. The chain of custody — the documented record of who collected it, when, how it was stored, who transferred it, and who received it — must be unbroken. A broken or undocumented chain of custody may render the analytical result inadmissible in court.
The duty to report:
Under Section 39 of the Code of Criminal Procedure (CrPC 1973) and in several state-specific regulations, doctors are obligated to report cases of suspected criminal poisoning to the police. This reporting obligation coexists with the duty of confidentiality — it is a statutory exception to confidentiality, not a conflict with it.
Simulation and supervised practice (FM14.2 and FM14.3):
Both FM14.2 and FM14.3 are designated 'simulated/supervised' competencies — meaning the skill must be practised on a standardised patient, a manikin, or under direct faculty supervision before it is assessed in the OSPE. Reading about these skills is necessary but not sufficient; physical practice is mandatory.
Provided image
Governing Principles: Toxicology Clinical Examination Framework
The universal toxicology examination approach (applicable to any unknown poisoning case) is structured around five questions:
- WHAT is the route of exposure? (ingestion, inhalation, skin/eye contact, injection, envenomation)
- WHAT is the toxidrome? (systematic examination of: CNS, pupils, vital signs, skin, mouth, smell, GI, neuromuscular)
- WHICH organ systems are compromised? (respiratory, cardiovascular, CNS, renal, hepatic, haematological)
- WHEN did exposure occur? (timeline determines management priorities — treatment windows vary by agent)
- WHAT is the medicolegal context? (accidental/suicidal/homicidal/occupational; who else was present; what was found at scene)
Systematic toxidrome examination — standard sequence:
Step 1 — Vital signs and airway: Respiratory rate + quality (shallow? Kussmaul? Cheyne-Stokes?); pulse rate and regularity; blood pressure; temperature; SpO₂ (noting its limitations in CO poisoning).
Step 2 — Level of consciousness and CNS: GCS; orientation; cranial nerve examination (pupils — size, reactivity, equality; ptosis; extraocular movements); neck stiffness; deep tendon reflexes (exaggerated = excitatory toxidrome; depressed = CNS depressant); clonus (serotonin syndrome marker).
Step 3 — Pupils: Miosis = opioids, OPs/carbamates. Mydriasis = anticholinergics, sympathomimetics. Normal pupils do NOT exclude significant poisoning.
Step 4 — Skin: Diaphoresis (sweating) = sympathomimetic, cholinergic, serotonin syndrome. Dry/flushed = anticholinergic. Cherry-red = CO, CN. Cyanosis = methaemoglobinaemia (nitrites, dapsone), hypoxia. Injection marks (location, number, fresh vs old).
Step 5 — Smell: Garlic/phosphorus (phosphorus, arsenic, AlP), bitter almond (cyanide), phenolic/antiseptic (carbolic acid), alcohol (ethanol, methanol), acetone/fruity (ketoacidosis, isopropanol).
Step 6 — Mouth and mucous membranes: Corrosive burns/colour (acid/alkali); blue-black staining (iodine); salivation/dryness (cholinergic vs anticholinergic); froth (pulmonary oedema — OP, cardiac failure).
Step 7 — GI: Abdominal tenderness; bowel sounds; check for haematemesis/malaena; examine vomitus (colour, smell, contents — pesticide odour, blood, tablet fragments).
Step 8 — Urine: Colour (myoglobinuria/haemoglobinuria = port-wine/red/brown; carboluria = green-black; ferrioxamine = pink-orange; normal yellow).
Step 9 — Neuromuscular: Fasciculations (OPs); tremor (mercury, lithium); flaccid paralysis (opioids, snake bite, botulism, barium); spastic/excitatory (organochlorines, strychnine).
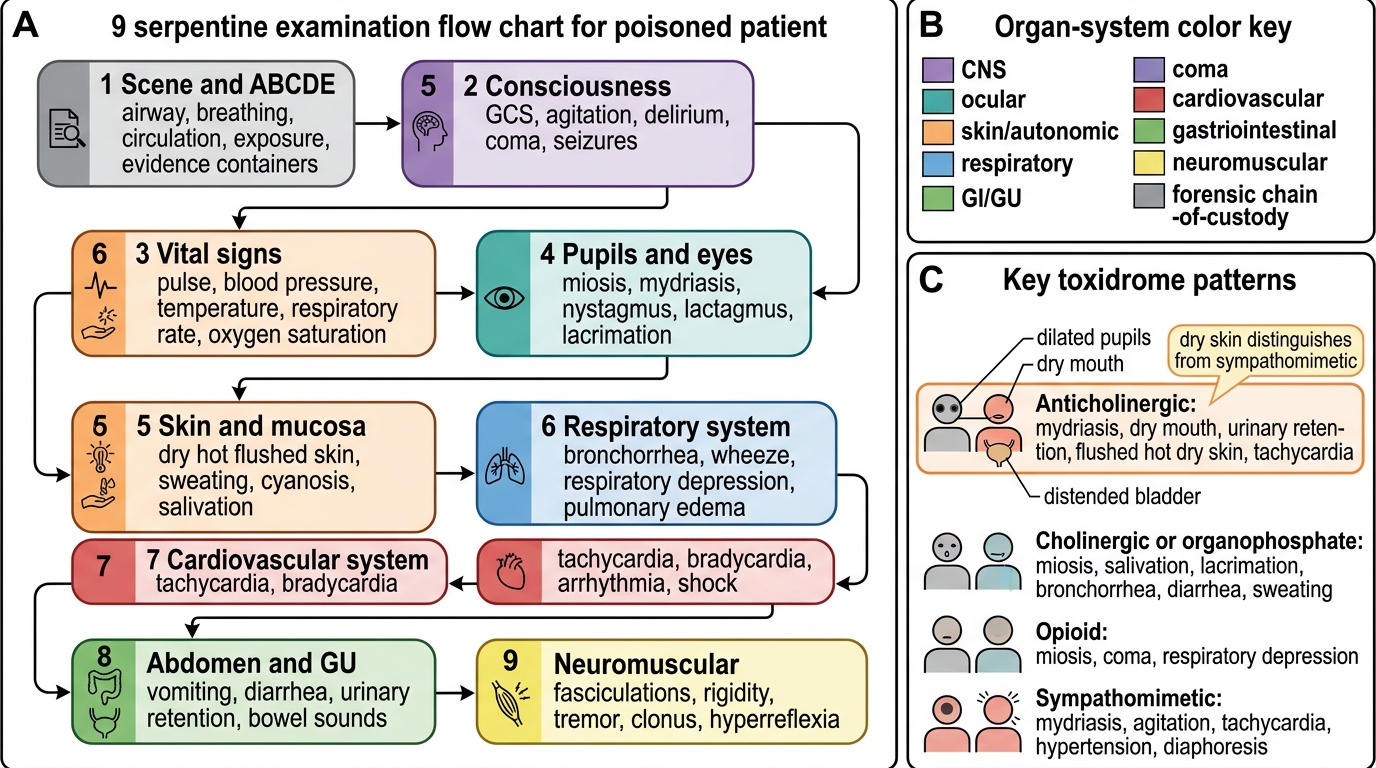
Systematic Examination Flow for the Poisoned Patient
SELF-CHECK
A patient is brought in by police for a clinical examination after a suspected poisoning. She is conscious and oriented. On examination: GCS 15, pupils 8 mm bilaterally and poorly reactive, dry mouth, urinary retention, flushed hot skin, heart rate 130 bpm, temperature 38.5°C. Which toxidrome does this represent and what is the most likely drug class?
A. Cholinergic toxidrome — organophosphate poisoning
B. Opioid toxidrome — heroin or morphine overdose
C. Anticholinergic toxidrome — tricyclic antidepressants or antihistamines
D. Sympathomimetic toxidrome — cocaine or amphetamine overdose
Reveal Answer
Answer: C. Anticholinergic toxidrome — tricyclic antidepressants or antihistamines
Anticholinergic toxidrome: mydriasis (8 mm dilated pupils), dry mouth, urinary retention, flushed hot skin, tachycardia, low-grade fever — the classic 'dry, hot, red, blind, mad, full' mnemonic. Drug classes: TCAs, antihistamines, atropine. Cholinergic (OP) has MIOSIS + SLUDGE; Opioids have MIOSIS + respiratory depression; Sympathomimetics (cocaine/amphetamine) have mydriasis + tachycardia + diaphoresis (sweating) — NOT dry skin. The dry skin distinguishes anticholinergic from sympathomimetic (sympathomimetic = diaphoresis).
Method: Specimen Collection, Preservation and Chain of Custody
FM14.3 requires the practical ability to collect, preserve, and dispatch forensic specimens in a suspected poisoning case. The following is the standard method for each specimen type.
SPECIMEN TYPES AND COLLECTION PROTOCOL:
1. Gastric aspirate/washings (HIGHEST PRIORITY — time-limited):
- Passed nasogastric tube before gastric lavage; collect first aspirate in a sealed glass bottle
- Label: patient name, date/time of collection, collector's name and signature
- Preserve: seal with wax; place in sealed paper bag; hand to police with countersignature
- Note: if lavage has already been performed, keep the lavage fluid for analysis (first 100–200 mL is most valuable)
2. Blood:
- Volume: 10 mL
- Container: fluoride-oxalate tube (grey-top) for ethanol/volatile substances; EDTA or plain tube for other analyses
- Specific: for CO poisoning — glass tube with cap sealed (HbCO is light-sensitive and vaporises)
- Label, sign, seal; hand to police officer with countersignature
3. Urine:
- Volume: 50 mL, mid-stream or catheter specimen
- Plain container; seal tightly
- Important for: drug screen, arsenic (24-h urine), carboluria, ferrioxamine (pink-orange in iron + deferoxamine)
4. Vomitus/stool:
- Collect entire available sample; do not dilute
- Glass or wide-mouth plastic container; sealed
5. Physical exhibits (containers, tablets, plant material):
- Place each item in a separate sealed paper bag (NOT plastic — some samples require air circulation; AND solvent-contaminated samples may dissolve plastic)
- Label each bag with contents, date, location of recovery
- The sealed bags constitute a formal 'property exhibit' — entered in the police property register
CHAIN-OF-CUSTODY DOCUMENTATION:
Every specimen must have a 4-fold witness label:
- Patient's name and hospital number
- Date and time of collection
- Type of specimen
- Name and signature of the collecting doctor
- Name and signature of the receiving police officer
The doctor retains a copy; the police officer takes the specimens. Every subsequent transfer (to forensic science laboratory, to court) requires a new signature by each handler. A gap in the documentation (e.g., the specimen was left unattended on a ward for two hours before police collection) may be challenged in court as 'tampering possibility'.
POST-MORTEM SPECIMEN COLLECTION (standard):
- Blood: 20 mL from femoral vein (NOT cardiac blood — post-mortem redistribution artefact is more pronounced in cardiac blood)
- Urine: entire bladder contents via suprapubic needle aspiration
- Vitreous humour: both eyes (vitreous has minimal post-mortem decomposition — most reliable PM specimen for glucose, CO, some drugs)
- Gastric contents: entire contents in a sealed container (label: 'gastric contents — do not use preservative')
- Liver: 100 g from right lobe
- Kidney: one entire kidney
- Hair and nails: for chronic metal/drug exposure
- Brain: for chlorinated solvents, volatile compounds
All PM specimens: place in sealed glass containers (use NO preservative for gastric contents); store at 4°C; deliver to forensic science laboratory within 24–48 hours.
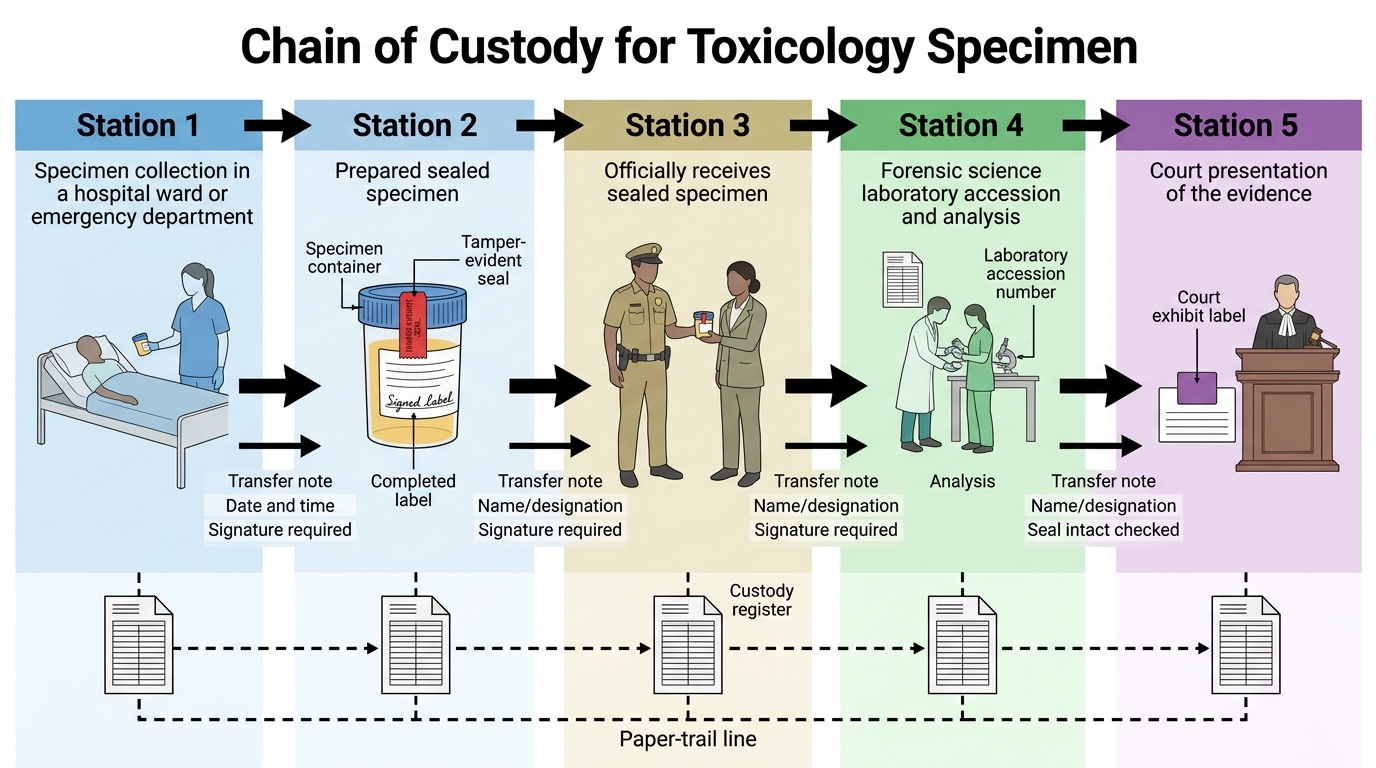
Chain of Custody for Toxicology Specimen