Page 6 of 16
FM13.{6,8} | Diagnosis & General Management of Poisoning — SDL Guide (Part 2)
Antidote Therapy: Specific Antidotes for Common Poisons
Specific antidotes are available for a limited but critically important set of poisons commonly encountered in India. An antidote reverses or mitigates the toxic effect through one of three mechanisms: pharmacological antagonism (blocking or competing at the receptor where the poison acts), physiological antagonism (counteracting the physiological effects through an opposing mechanism), or chemical antagonism (binding the poison itself to reduce its free concentration). Knowing the correct antidote, its mechanism, timing, and contraindications is one of the highest-yield competencies in clinical toxicology.
Provided image
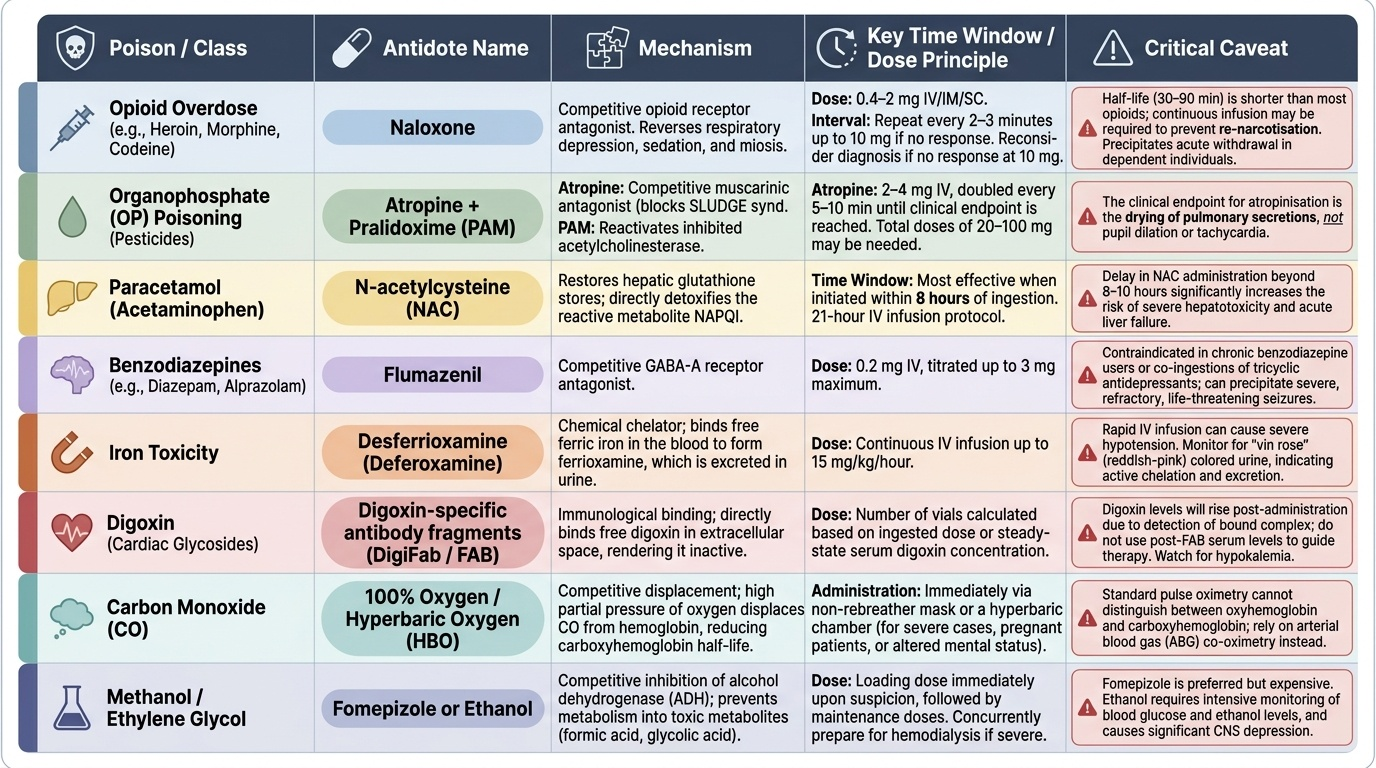
The following table summarises the key antidotes. The critical time windows and caveats are non-negotiable — an antidote given outside its effective window, or to the wrong patient, can cause serious harm.
Opioid overdose: naloxone (competitive opioid receptor antagonist) reverses all effects of opioid overdose — respiratory depression, sedation, and miosis. Dose: 0.4-2 mg IV/IM/SC, repeat every 2-3 minutes up to 10 mg if no response (if no response at 10 mg, reconsider diagnosis). Half-life of naloxone (30-90 min) is shorter than most opioids — an infusion or repeated dosing may be required for long-acting opioids (methadone, buprenorphine, morphine SR) to prevent 're-narcotisation.' Naloxone precipitates acute withdrawal in dependent individuals.
Organophosphate (OP) poisoning: the two-drug regimen of atropine + pralidoxime (PAM) is mandatory. Atropine (competitive muscarinic antagonist) reverses the muscarinic effects — the SLUDGE syndrome, bronchospasm, bradycardia — and must be given in high doses until the secretions dry (the clinical end-point is drying of secretions, not pupil dilation or tachycardia). Starting dose 2-4 mg IV, doubled every 5-10 minutes until secretions dry; total doses of 20-100 mg may be required in severe OP poisoning. Pralidoxime (PAM, 2-PAM) reactivates the inhibited acetylcholinesterase enzyme by displacing the OP from the active serine site — this must be given within 24-48 hours of exposure, before irreversible 'ageing' of the cholinesterase-OP bond occurs. After ageing, PAM has no effect and is potentially harmful. Dose: 1-2 g IV over 15-30 minutes, then infusion. Note: PAM does NOT reverse muscarinic effects and does NOT replace atropine — both must be given together.
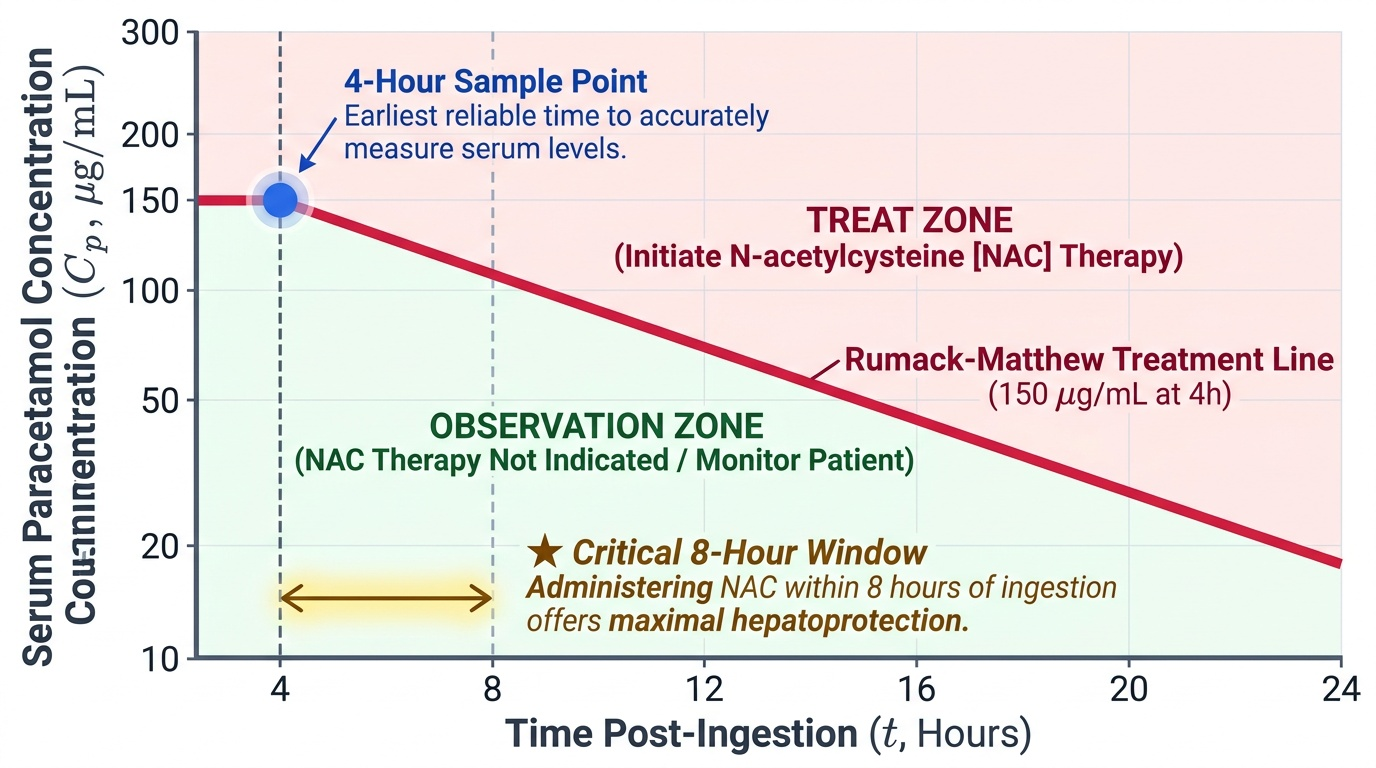
Paracetamol (acetaminophen) overdose: N-acetylcysteine (NAC) replenishes glutathione, which is depleted in overdose, thereby preventing accumulation of the toxic intermediate NAPQI (N-acetyl-p-benzoquinone imine) that causes hepatocellular necrosis. Timing is critical: NAC is most effective within 8 hours of ingestion (near-complete hepatoprotection), remains effective from 8-24 hours (partial protection), and has reduced but still clinically meaningful benefit beyond 24 hours. The decision to treat is based on the Rumack-Matthew nomogram — serum paracetamol level measured at 4 hours post-ingestion plotted against time. If the level falls on or above the treatment line, NAC is started. NAC is given IV: loading dose 150 mg/kg in 200 mL D5W over 60 minutes, followed by a 4-hour infusion, then a 16-hour infusion (modified Prescott regimen).
Benzodiazepine overdose: flumazenil (competitive GABA-A benzodiazepine receptor antagonist) reverses benzodiazepine sedation within 1-2 minutes. However, it is contraindicated in chronic benzodiazepine users (precipitates acute withdrawal seizures) and in mixed overdoses with tricyclic antidepressants (removal of the anticonvulsant effect of benzodiazepines unmasks TCA-related seizures). Its half-life (1-2 hours) is shorter than most benzodiazepines — resedation occurs and repeat dosing is required. In practice, flumazenil is used diagnostically (to confirm benzodiazepine overdose) more than therapeutically.
Iron poisoning: desferrioxamine (deferoxamine) is a chelating agent that binds free ferric iron (Fe³⁺) in plasma and tissues to form ferrioxamine, which is renally excreted (imparting a characteristic 'vin rosé' pink colour to urine, confirming ongoing iron toxicity). It is indicated when serum iron exceeds the total iron binding capacity (TIBC), the patient is symptomatic, or serum iron >90 μmol/L.
Digoxin toxicity: digoxin-specific FAB antibody fragments (Digibind/DigiFab) bind and neutralise digoxin and other cardiac glycosides (including plant glycosides from oleander and yellow oleander — important in India). Each vial neutralises 0.5 mg digoxin; the dose is calculated from the ingested amount or serum digoxin level.
Methanol/ethylene glycol poisoning: fomepizole (4-methylpyrazole, preferred where available) or ethanol (IV or oral, 100% alcohol diluted to 10% in D5W) competitively inhibits alcohol dehydrogenase, preventing conversion of methanol to formaldehyde/formate (which causes metabolic acidosis and blindness) and ethylene glycol to oxalic acid/oxalate crystals (which cause renal failure). Haemodialysis removes methanol, ethylene glycol, and their toxic metabolites directly.
SELF-CHECK
A farmer with severe organophosphate poisoning (miosis, bradycardia, copious secretions, fasciculations) is treated with atropine 4 mg IV. After 10 minutes, his secretions are still profuse and he remains bradycardic. What is the most appropriate next step?
A. Switch from atropine to glycopyrrolate as atropine has failed
B. Double the atropine dose to 8 mg IV and re-assess secretion dryness every 5-10 minutes
C. Give pralidoxime (PAM) first and then reassess the atropine need
D. Withhold further atropine — tachycardia and pupil dilation have not occurred yet
Reveal Answer
Answer: B. Double the atropine dose to 8 mg IV and re-assess secretion dryness every 5-10 minutes
The clinical endpoint for atropine in OP poisoning is drying of secretions — NOT tachycardia and NOT pupil dilation. In severe OP poisoning, massive doses of atropine are required (total doses of 20-100 mg are reported). Since secretions remain profuse at 4 mg, the dose should be doubled to 8 mg and continued until secretions dry, repeating every 5-10 minutes. Switching agents is unnecessary. PAM should also be started (within 24-48h window for cholinesterase reactivation) but it does not replace atropine for muscarinic effects. Using tachycardia or pupil dilation as the endpoint leads to under-dosing atropine.
Enhanced Elimination: Accelerating Poison Removal
Enhanced elimination techniques accelerate the removal of absorbed poison from the body, using physiological and extracorporeal methods. Not all poisons benefit from enhanced elimination — effectiveness depends on the physicochemical properties of the poison (particularly Vd, protein binding, molecular weight, and water solubility) and the availability of facilities. Understanding which method applies to which poison is a frequently tested competency.
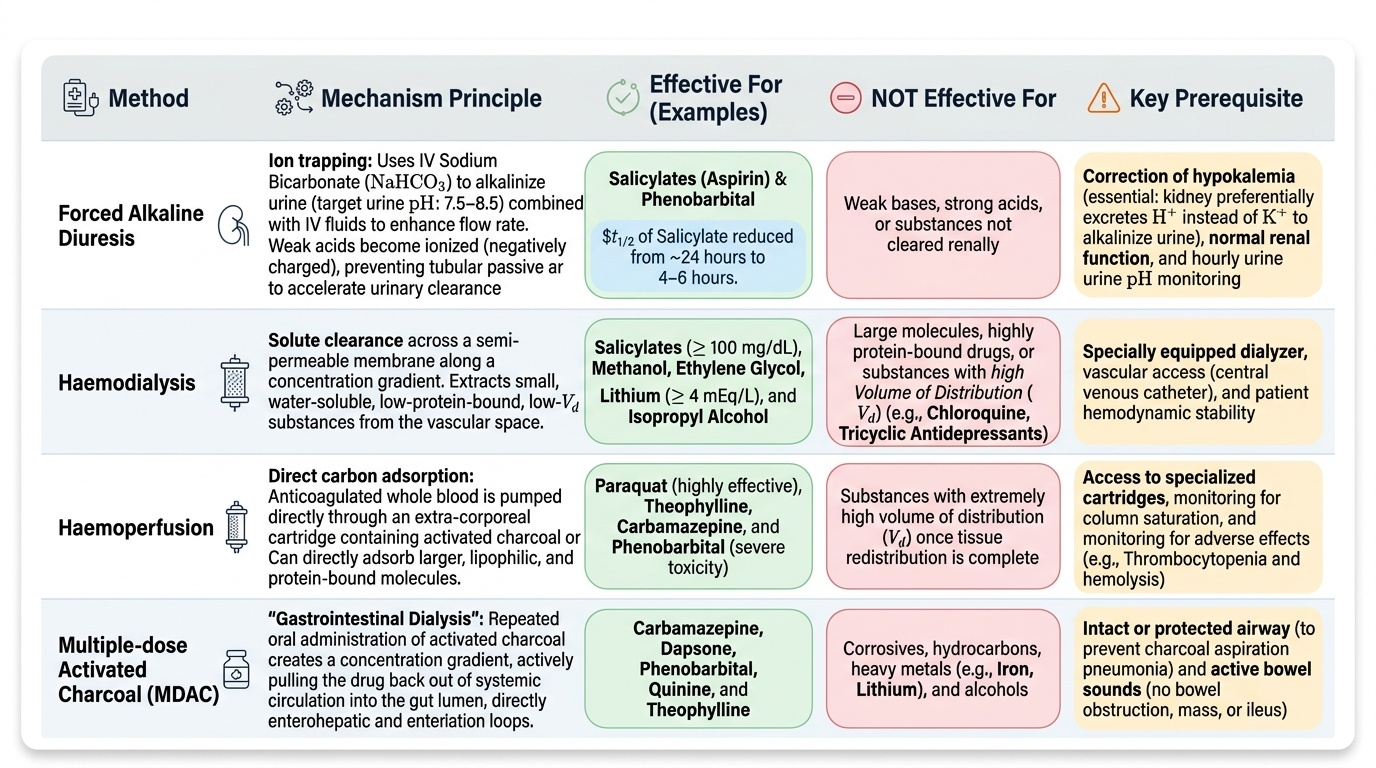
Forced alkaline diuresis uses IV sodium bicarbonate to alkalinise the urine (target urine pH 7.5-8.5), combined with IV fluid loading to increase urine flow rate. The mechanism is ion trapping: weak acids (pKa 3-8) become ionised (negatively charged) in alkaline urine and cannot be passively reabsorbed through the tubular epithelium, increasing urinary excretion. Indications: salicylate (aspirin) poisoning and phenobarbital poisoning. Forced alkaline diuresis can reduce salicylate half-life from ~24 hours to 4-6 hours. Monitoring: urine pH every 1-2 hours, serum electrolytes (hypokalaemia must be corrected — the kidney preferentially excretes H⁺ over K⁺ to alkalinise the urine), blood glucose.
Haemodialysis removes small, water-soluble, low-protein-bound, low-Vd substances from the bloodstream across a semi-permeable membrane. Indications: salicylates, methanol, ethylene glycol, lithium, and isopropyl alcohol — all small, water-soluble molecules with low Vd and low protein binding. Haemodialysis is indicated for: salicylate level >100 mg/dL with severe toxicity, methanol-associated metabolic acidosis unresponsive to bicarbonate, ethylene glycol with renal failure, lithium level >4 mEq/L with neurological toxicity. Haemodialysis does NOT effectively remove substances with high Vd (chloroquine, tricyclic antidepressants) or those highly protein-bound.
Haemoperfusion passes blood through a column of activated charcoal or ion-exchange resin, which adsorbs the poison directly from the blood. Unlike haemodialysis, it can remove larger, lipophilic, and protein-bound substances. Indications: paraquat (highly effective — paraquat has a moderate Vd but is not well removed by dialysis), theophylline, carbamazepine, phenobarbital (for severe toxicity), and some barbiturate overdoses. Limitations: thrombocytopenia, charcoal column saturation, haemolysis.
Multiple-dose activated charcoal (MDAC) exploits the principle that charcoal in the GI lumen can adsorb poison that re-enters the gut from the bloodstream via the enterohepatic or enteroenteric circulation — acting as a 'gut dialysis.' Dose: 25-50 g every 4-6 hours. Indications: theophylline, carbamazepine, phenobarbital, quinine — substances with significant enterohepatic recirculation or slow-release formulations.
Provided image
| Method | Mechanism | Effective For | NOT Effective For | Key Requirement |
|---|---|---|---|---|
| Forced alkaline diuresis | Ion trapping of weak acids in alkaline urine | Salicylates, phenobarbital | Weak bases, high-Vd drugs | Urine pH 7.5-8.5; correct hypokalaemia |
| Haemodialysis | Diffusion across semi-permeable membrane | Salicylates, methanol, ethylene glycol, lithium | High-Vd or protein-bound drugs | Low Vd, water-soluble, low protein binding |
| Haemoperfusion | Direct adsorption onto charcoal/resin | Paraquat, theophylline, carbamazepine | Not better than dialysis for small molecules | Trained centre; risk of thrombocytopenia |
| MDAC | Gut dialysis — interrupts enterohepatic cycling | Theophylline, carbamazepine, phenobarbital | Iron, lithium, alcohols | Intact bowel function; airway protected |
CLINICAL PEARL
The activated charcoal contraindication list is an exam trap: Students commonly administer charcoal for iron and lithium poisonings because 'charcoal adsorbs everything.' It does not. The substances AC does NOT work for must be memorised as a complete list: iron, lead, lithium, alcohols (methanol, ethanol, isopropanol), strong inorganic acids, strong alkalis, potassium, cyanide, and fluoride. For iron, the correct management is gastric lavage within 1-2 hours then whole bowel irrigation followed by desferrioxamine. For lithium, haemodialysis is indicated for severe toxicity. A second critical trap is pralidoxime timing: PAM must be given within 24-48 hours of OP exposure before cholinesterase ageing makes it permanently ineffective. A common exam question gives a patient presenting 3 days after OP ingestion — at that point, PAM is not only ineffective but potentially harmful (paradoxical cholinergic worsening reported). Atropine remains effective regardless of timing.
SELF-CHECK
A patient with methanol poisoning (serum methanol 45 mmol/L, metabolic acidosis, visual symptoms) arrives at a district hospital where fomepizole is not available. Which management strategy is most appropriate?
A. Activated charcoal 1 g/kg and observe — methanol is absorbed slowly
B. Ethanol (as 10% solution in D5W IV, targeting blood ethanol 100-150 mg/dL) to inhibit alcohol dehydrogenase, combined with haemodialysis if available
C. Forced alkaline diuresis alone is sufficient to eliminate methanol
D. Pralidoxime is effective as an alternative alcohol dehydrogenase inhibitor
Reveal Answer
Answer: B. Ethanol (as 10% solution in D5W IV, targeting blood ethanol 100-150 mg/dL) to inhibit alcohol dehydrogenase, combined with haemodialysis if available
When fomepizole is unavailable, ethanol is the appropriate substitute — it competitively inhibits alcohol dehydrogenase with higher affinity than methanol, preventing conversion to the toxic metabolites formaldehyde and formate. The target blood ethanol is 100-150 mg/dL. Haemodialysis directly removes methanol and its metabolites and should be added if the patient has severe metabolic acidosis or visual symptoms. Activated charcoal does not adsorb alcohols. Forced alkaline diuresis alone is inadequate for severe methanol toxicity. Pralidoxime is a cholinesterase reactivator with no role in methanol poisoning.
Medicolegal Aspects of Poisoning Management
The management of a poisoning case is simultaneously a clinical and a medico-legal event. Every clinical decision and its rationale must be documented in real time because this documentation will be scrutinised in potential criminal investigations, inquest proceedings, and civil negligence actions.
Police intimation is mandatory in all cases where poisoning is suspected to be suicidal, homicidal, or the circumstances are unclear. This is a statutory duty under CrPC MLC provisions (see SDL tx1) — it is not dependent on patient consent and cannot be withheld by the family. The intimation must be in writing, delivered or transmitted to the nearest police station, and a copy retained in the hospital records.
Consent for procedures in the unconscious patient: an unconscious patient cannot provide informed consent. Under the law of necessity (and MCI/NMC guidelines), emergency treatment necessary to save life may be initiated without consent. However, this does not extend to non-emergency procedures — for example, blood collection for forensic alcohol analysis requires the presence of a police officer with appropriate legal authority (a warrant or magistrate order), not just clinical convenience. This distinction matters when blood is collected for forensic purposes versus clinical diagnosis.
Documentation standards in acute poisoning: the MLC register entry must include: date, time, MLC number, name and age, alleged substance and quantity, time of exposure, clinical findings at presentation (GCS, vital signs, pupils, relevant positive and negative findings), MLC register entry signed and witnessed, treatment initiated, samples collected with chain-of-custody details, and police intimation sent (time, to whom, received by).
Physician liability in poisoning management can arise under the Consumer Protection Act 2019 (deficiency in service — management errors) and the NMC Act 2020 (professional misconduct — failure to report). Common medicolegal pitfalls: failure to document the time of notification, failure to initiate NAC within the 8-hour window for paracetamol (an eminently preventable outcome where late treatment is now well-documented), prescribing PAM beyond the 48-hour window in OP poisoning (ineffective treatment), and administering activated charcoal to an obtunded patient without airway protection (aspiration pneumonitis).
Provided image