Page 19 of 25
IM1.25 | Adult Congenital Heart Disease Presentations — SDL Guide (Part 2)
Management: Eisenmenger Syndrome, Intervention, and Special Considerations
The management of adult congenital heart disease requires specialist input from dedicated ACHD centres, but the general physician must understand the principles of when to close a defect, when closure is contraindicated, how to manage Eisenmenger syndrome, and the specific considerations around anticoagulation, endocarditis prophylaxis, and pregnancy. Failure to grasp these principles can lead to the catastrophic error of recommending defect closure in a patient with established Eisenmenger physiology — a mistake that precipitates irreversible right heart failure.
Timing and indications for defect closure:
The ideal time for CHD correction is in childhood, before irreversible pulmonary vascular changes develop. However, adults presenting with previously unrecognised defects may still benefit from closure if PVR is not severely elevated. The decision to close a defect in an adult is guided by the shunt ratio (Qp:Qs) — the ratio of pulmonary to systemic blood flow — and the PVR:
- A Qp:Qs ≥1.5:1 with PVR <3 Wood units favours closure.
- PVR 3–5 Wood units — borderline; requires vasodilator reversibility testing.
- PVR >6–8 Wood units — closure is contraindicated; Eisenmenger physiology.
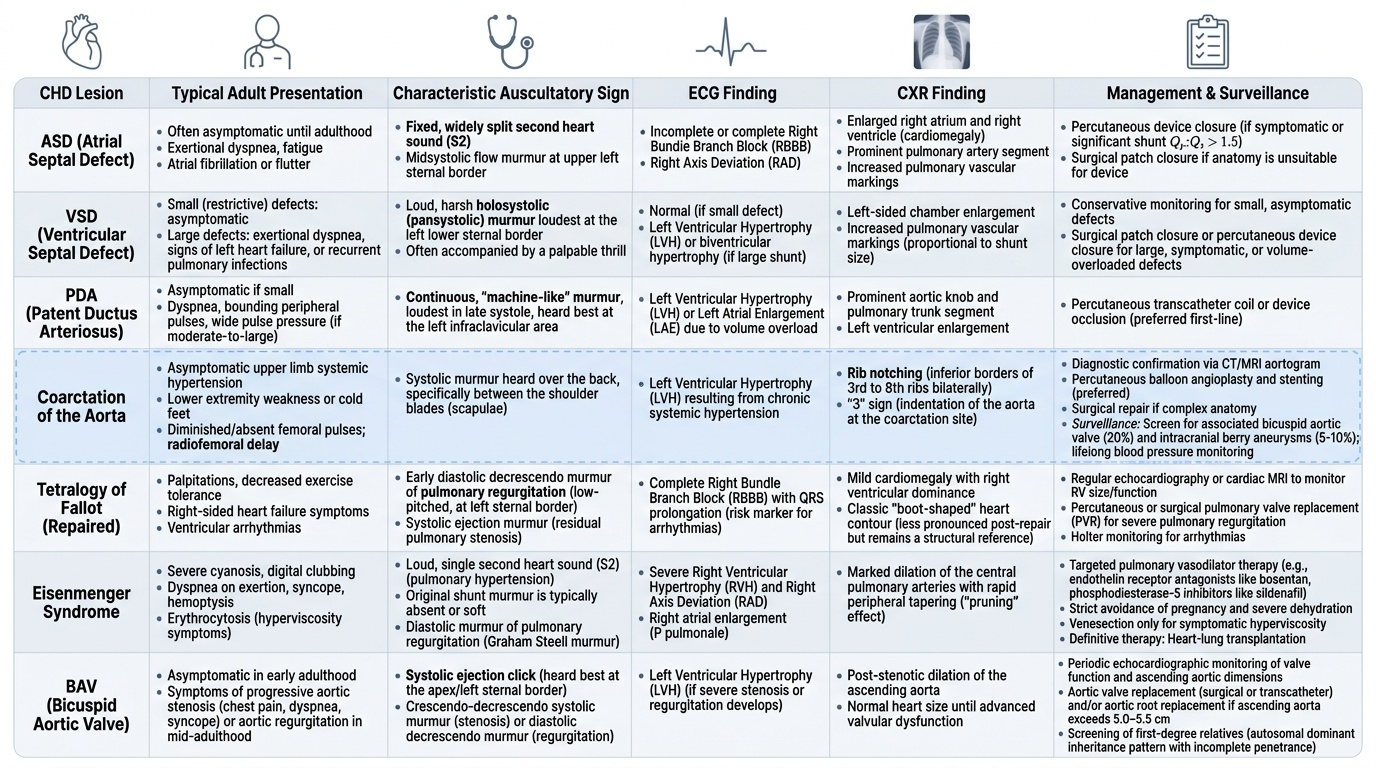
ASD closure: Ostium secundum ASDs can be closed percutaneously by transcatheter ASD closure device (Amplatzer septal occluder) if the anatomy is suitable (sufficient rim, defect size ≤38 mm). Ostium primum and sinus venosus ASDs require surgical repair (no suitable percutaneous device).
VSD closure: Small restrictive VSDs (high-gradient, small Qp:Qs) — observational, because many close spontaneously in childhood and even early adulthood; if open in adults with a small size, the risk of endocarditis exceeds the haemodynamic burden. Moderate-large VSDs with Qp:Qs ≥2:1 — close percutaneously (muscular VSDs) or surgically (perimembranous VSDs). Eisenmenger VSD — closure contraindicated.
PDA closure: All haemodynamically significant PDAs should be closed (percutaneous coil or device closure for most; surgical ligation if very large). Even small PDAs carry endocarditis risk and should be considered for closure.
Eisenmenger syndrome management:
Once Eisenmenger syndrome is established, closure of the underlying defect is absolutely contraindicated — the shunt is now acting as a 'pop-off valve' for the failing right ventricle; closing it would cause acute right heart failure and death. Management is palliative and supportive:
- Pulmonary arterial hypertension (PAH)-targeted therapy: Endothelin receptor antagonists (bosentan, ambrisentan) — improve exercise capacity and quality of life. Phosphodiesterase-5 inhibitors (sildenafil, tadalafil) — also benefit. These drugs lower PVR to some extent but cannot reverse established Eisenmenger physiology.
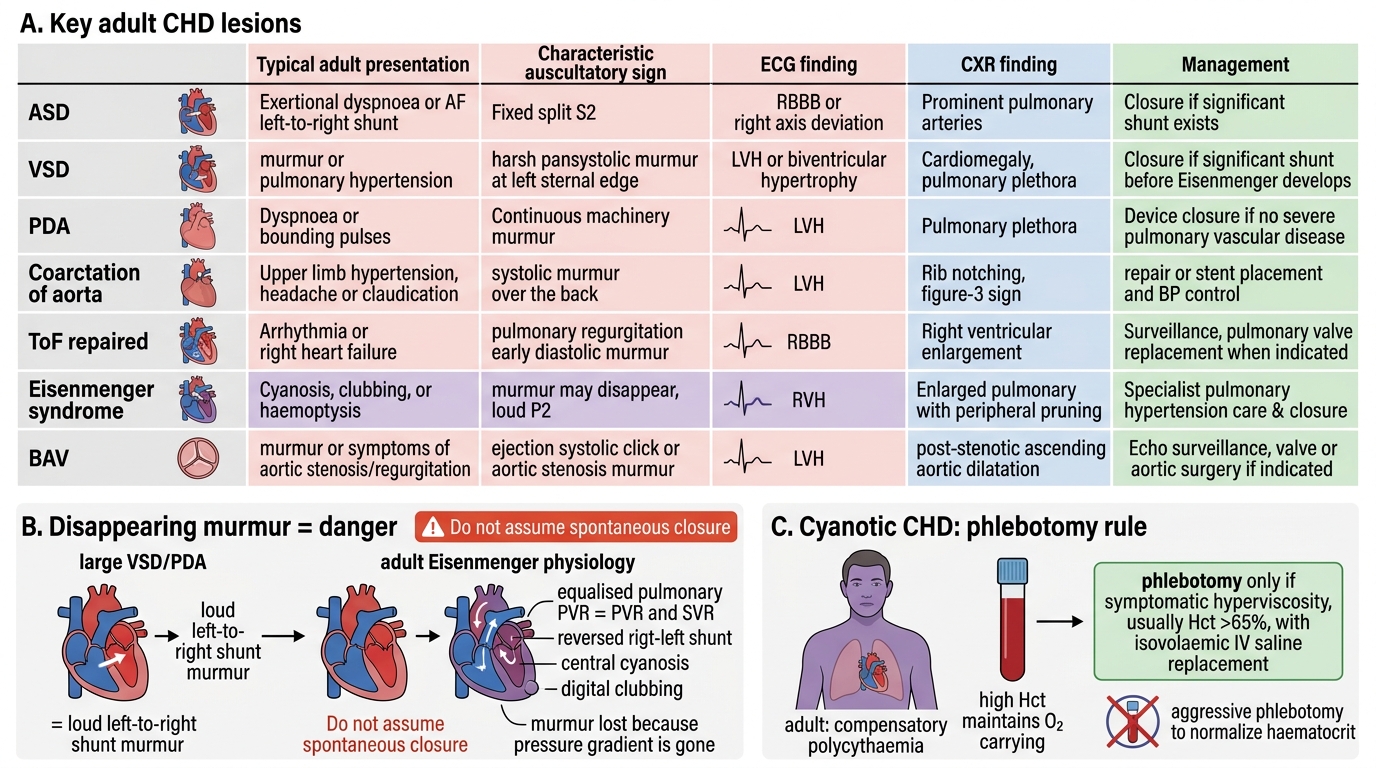
- Phlebotomy: Polycythaemia is a compensatory mechanism for hypoxia — do NOT routinely phlebotomise to normalise haematocrit (this worsens oxygen-carrying capacity). Phlebotomy is indicated only for symptomatic hyperviscosity (headache, visual disturbance, confusion) when Hct >65%, with isovolaemic replacement (IV saline of same volume as blood removed).
- Anticoagulation: Controversial — VTE risk vs. haemoptysis risk. Current ESC guidelines suggest anticoagulation only for specific indications (in situ PA thrombosis, AF) not routinely.
- Iron supplementation: Iron deficiency is common in Eisenmenger (frequent phlebotomies, poor GI absorption) and reduces exercise tolerance; correct with oral or IV iron.
- Pregnancy: Absolutely contraindicated in Eisenmenger syndrome — maternal mortality is 30–50%. The reduction in systemic vascular resistance during pregnancy and at delivery causes catastrophic increase in R→L shunting and haemodynamic collapse.
- Cardiac-pulmonary transplantation: The only definitive option in refractory Eisenmenger; combined heart-lung transplant or bilateral lung transplant with repair of the cardiac defect. Very limited by donor organ availability.
Endocarditis prophylaxis in adult CHD:
The highest-risk groups who should receive antibiotic prophylaxis before invasive dental procedures are: (1) patients with prosthetic cardiac valves or prosthetic material used for cardiac valve repair, (2) patients with a history of infective endocarditis, (3) unrepaired cyanotic CHD including Eisenmenger syndrome, (4) repaired CHD with prosthetic material within 6 months, (5) repaired CHD with residual defects adjacent to prosthetic material. Prophylaxis: amoxicillin 2 g orally 30–60 minutes before the procedure (clindamycin 600 mg for penicillin-allergic patients). Importantly, routine prophylaxis is NOT recommended for most repaired CHD or simple lesions like isolated small VSDs.
Pregnancy and ACHD:
- Low-risk CHD (closed ASD, small VSD, repaired CoA with good BP control, mild pulmonary stenosis) — pregnancy is generally safe with specialist monitoring.
- Moderate-to-high risk (severe left heart obstruction — AS or LVOTO, significant MR/AR, severe pulmonary stenosis, Fontan circulation) — requires dedicated ACHD centre management.
- Absolute contraindications: Eisenmenger syndrome (30–50% maternal mortality), severe PAH, severe uncorrected systemic obstruction.
- Marfan syndrome with aortic root >45 mm: very high risk of aortic dissection during pregnancy (the hormonally-mediated changes in aortic wall during pregnancy exacerbate the pre-existing connective tissue weakness).
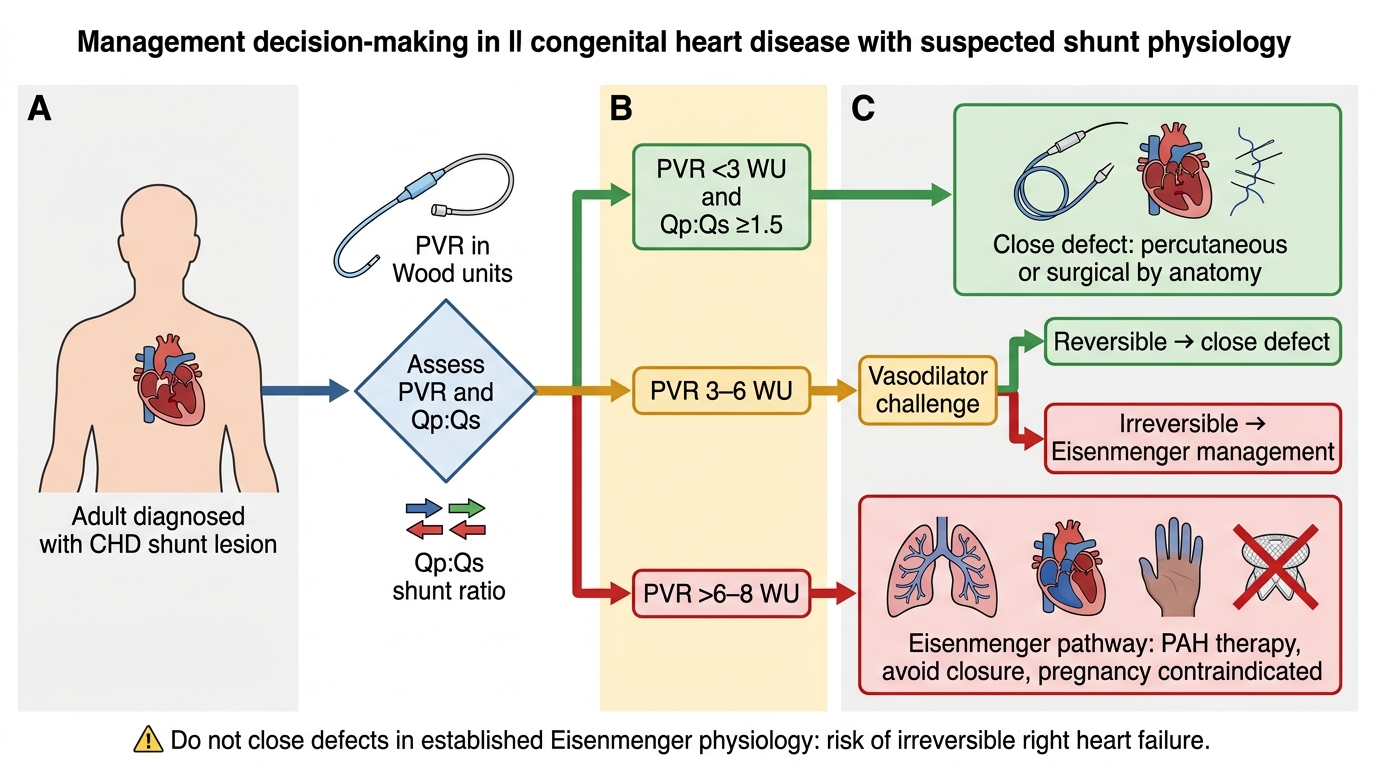
Adult CHD Shunt Closure Decision Algorithm
SELF-CHECK
A 22-year-old woman with Eisenmenger syndrome complicating a large VSD (PVR 9 Wood units, SpO₂ 82% at rest) is referred from a peripheral hospital for advice on management. She mentions she is planning to get married and asks about pregnancy. Which of the following statements is MOST accurate?
A. Pregnancy is safe in Eisenmenger syndrome if she is on PAH-targeted therapy such as bosentan
B. Pregnancy is absolutely contraindicated in Eisenmenger syndrome due to 30–50% maternal mortality
C. VSD closure during the first trimester of pregnancy would resolve the Eisenmenger physiology and make pregnancy safe
D. Low-dose aspirin throughout pregnancy will reduce the risk of thrombotic complications sufficiently to permit safe pregnancy
Reveal Answer
Answer: B. Pregnancy is absolutely contraindicated in Eisenmenger syndrome due to 30–50% maternal mortality
Pregnancy is absolutely contraindicated in Eisenmenger syndrome. Maternal mortality is 30–50%, occurring predominantly at delivery and in the immediate postpartum period when systemic vascular resistance falls sharply (afterload reduction), dramatically increasing right-to-left shunting and causing haemodynamic collapse. PAH-targeted therapy does not change this fundamental risk — it may improve functional capacity but cannot normalise the PVR or reverse Eisenmenger physiology. VSD closure at this stage (PVR 9 Wood units) would cause acute right ventricular failure and death — the shunt is acting as an essential right ventricular 'pop-off valve'. The patient must be clearly counselled against pregnancy and offered appropriate contraception.
Self-Assessment: Clinical Vignettes and Integration
At this stage you have covered the fundamental acyanotic vs cyanotic distinction, the major adult CHD lesions and their clinical signatures, the pathophysiology of Eisenmenger syndrome, the principles of investigation, and the management framework. The self-assessment section below tests integration of these themes under examination conditions, applying the knowledge to clinical vignettes that mirror the level expected in IM1.25 (KH level — knowledge with the ability to apply to clinical scenarios).
Provided image
Vignette A:
A 40-year-old man is found to have a blood pressure of 168/96 in the right arm at a routine health check. He is asymptomatic. The nurse notes that when she tries to measure his blood pressure in the left leg, she cannot palpate a femoral pulse. His BMI is 24 and he has no family history of hypertension. Examination reveals a systolic murmur over the back between the shoulder blades and a radiofemoral delay. His CXR shows notching of the 3rd–8th ribs bilaterally. ECG shows left ventricular hypertrophy.
Analysis: This is coarctation of the aorta presenting in adulthood as isolated upper limb hypertension. The classic signs are all present: BP differential (arm > leg), radio-femoral delay, back murmur (intercostal collaterals), rib notching (dilated intercostal arteries eroding the inferior rib surface), and LVH on ECG (from long-standing systemic hypertension). Management: CT or MRI aortogram to characterise the coarctation; if anatomy is suitable — percutaneous balloon dilatation and stenting is the preferred technique; surgical repair for complex anatomy. Additionally: screen for bicuspid aortic valve (20% association), and intracranial aneurysms (5–10% association in coarctation). Lifelong follow-up required even after repair — systemic hypertension, aortopathy, and re-coarctation must be monitored.
Vignette B:
A 55-year-old woman with known atrial fibrillation presents to the emergency department with sudden onset left-sided limb weakness. Brain CT shows a right MCA territory infarct. She has no known valvular disease, no hypertension, no diabetes, and no carotid stenosis on Doppler. Her cardiologist recalls she had a 'minor heart abnormality' detected incidentally on an echocardiogram 10 years ago that was described as 'not significant'. Transthoracic echo with bubble study: agitated saline injected IV — bubbles appear in the left atrium within 2 beats of injection.
Analysis: The bubble study confirms a patent foramen ovale (PFO) with right-to-left shunting (bubbles cross from right atrium to left atrium, confirming a defect with R→L passage). The mechanism of stroke is paradoxical embolism: a thrombus (from deep veins or right-sided chambers) crosses the PFO into the left-sided circulation and embolises to the brain. AF in this patient could have further promoted thrombus formation. The RoPE (Risk of Paradoxical Embolism) score helps risk-stratify PFO-associated stroke. Management post-cryptogenic stroke with PFO in patients aged <60: transcatheter PFO closure (reduces recurrent stroke vs anticoagulation alone in selected patients — REDUCE, RESPECT, CLOSE trials).
Vignette C:
A 30-year-old man with a history of surgical ToF repair at age 3 years is referred for worsening exercise intolerance over 2 years. He can no longer climb stairs without breathlessness. ECG: sinus rhythm, RBBB (QRS 155 ms). Echo: RV severely dilated (RV end-diastolic volume index 180 mL/m²), free pulmonary regurgitation (PR fraction 55%), and LVEF 55%.
Analysis: This is the most common late complication of repaired Tetralogy of Fallot — severe pulmonary regurgitation following infundibulotomy and transannular patch repair (which necessarily renders the pulmonary valve incompetent). Chronic free pulmonary regurgitation causes progressive right ventricular dilatation and eventually RV dysfunction. QRS duration (RBBB width) on ECG correlates with RV dilatation in post-ToF repair patients. Cardiac MRI is the gold standard to quantify RV volumes. Management: when RV end-diastolic volume index >160 mL/m² or RV EF falls — pulmonary valve replacement (surgical or transcatheter with a bioprosthetic valve) to restore pulmonary competence, reverse RV dilatation, and prevent RV failure and sudden cardiac death.
Adult CHD Lesions: Key Findings and Clinical Pearls
CLINICAL PEARL
Two critical clinical pearls for adult CHD:
Pearl 1 — The disappearing murmur in VSD or PDA is an alarm, not reassurance: When a patient with a known large VSD or PDA is found to have lost their murmur in adult life, this is NOT good news (suggesting spontaneous closure). A large shunt defect rarely closes spontaneously in adulthood. Loss of the murmur alongside new central cyanosis means Eisenmenger syndrome has developed — the pressure gradient across the defect has been abolished by equalised PVR and SVR, and the shunt has reversed. This is now a surgically uncorrectable condition.
Pearl 2 — All cyanotic CHD patients need phlebotomy for symptomatic hyperviscosity only, with isovolaemic replacement: A common error is aggressive phlebotomy to 'normalise' the haematocrit in polycythaemic Eisenmenger patients. The polycythaemia is a compensatory response to chronic hypoxia — it maintains oxygen-carrying capacity. Removing it without replacing it (isovolaemic replacement with IV saline) worsens oxygen delivery and causes decompensation. Phlebotomy is reserved for symptoms of hyperviscosity (Hct >65% with symptoms) and must always include isovolaemic volume replacement.