Page 6 of 25
IM1.{8-14,26} | Heart Failure Clinical Evaluation — SDL Guide (Part 2)
Interpreting Findings: What Each Sign Means in Heart Failure
Interpreting the findings obtained during the structured examination requires mapping each sign to its haemodynamic mechanism and diagnostic significance. The integration of multiple signs allows estimation of the type of failure (left vs right, systolic vs diastolic), its severity, and the underlying aetiology. This section provides the interpretive framework — a sign-by-sign guide from mechanism to clinical significance.
Raised JVP — what it tells you and what it does not. An elevated JVP (>4 cm above the sternal angle) signifies elevated right atrial pressure. In the context of bilateral ankle oedema and a displaced apex beat, it confirms biventricular failure. In isolation, a raised JVP may reflect: (1) right ventricular failure secondary to left heart failure (commonest cause globally); (2) cor pulmonale (right heart failure from primary lung disease — COPD, pulmonary fibrosis, pulmonary hypertension); (3) cardiac tamponade (Beck's triad: raised JVP + hypotension + muffled heart sounds — here the JVP paradoxically rises with inspiration rather than falling — the reverse of normal — a sign called Kussmaul's sign); (4) constrictive pericarditis (raised JVP that rises on inspiration — Kussmaul's positive — with normal heart size on CXR, pericardial calcification, and rapid steep y descent); (5) superior vena cava obstruction (raised JVP without pulsation — no transmitted waveform). The waveform analysis distinguishes further: prominent v wave + pulsatile liver = tricuspid regurgitation; absent a wave = atrial fibrillation; cannon a wave = atrioventricular dissociation (complete heart block, VT).
Apex beat displacement and character interpretation. A displaced apex beat beyond the 5th ICS MCL indicates left ventricular enlargement (LV dilatation). Combined with a diffuse, poorly sustained (thrusting or heaving) character, it is consistent with dilated cardiomyopathy or volume-overloaded states (chronic AR, MR). A non-displaced heaving apex suggests LV pressure overload with hypertrophy but no dilatation — as in systemic hypertension or hypertrophic cardiomyopathy. An absent or impalpable apex in the expected position with a raised JVP and muffled heart sounds = pericardial effusion (cardiac tamponade). NYHA class can be cross-checked: if the apex is displaced and the patient reports dyspnoea on minimal exertion, NYHA Class III is likely.
Pulse character and its diagnostic implications. Interpreting the pulse character in heart failure requires distinguishing the abnormality, quantifying it where possible, and linking it to the underlying aetiology:
- Pulsus alternans (alternate strong/weak beats in sinus rhythm): severe LV systolic dysfunction, LV ejection fraction likely <30%. Quantify: systolic BP on strong beat minus BP on weak beat (if >10 mmHg, clinically significant).
- Pulsus paradoxus (>10 mmHg inspiratory fall in systolic BP): cardiac tamponade (most specific), severe cardiac asthma, constrictive pericarditis, massive pulmonary embolism. Always confirm with sphygmomanometry.
- Collapsing pulse (rapid upstroke + rapid collapse, water-hammer quality): aortic regurgitation, severe anaemia, arteriovenous fistula, hyperthyroidism, patent ductus arteriosus. Elevated pulse pressure (>60 mmHg) confirms.
- Plateau (slow-rising, narrow pulse pressure) pulse: severe aortic stenosis — correlates with the gradient across the valve.
- Irregularly irregular pulse: atrial fibrillation — extremely common in HF; assess for an apical-radial pulse deficit (apical rate > radial rate = beats not generating enough stroke volume to be palpated at the wrist, confirming rapid AF with inadequate ventricular filling).
Heart sounds and murmurs — diagnostic integration (IM1.13). The two key added sounds in HF are S3 and S4. S3 (heard in early diastole; "Ken-tucky" cadence at the apex) is the most specific physical sign of elevated LV filling pressure and reduced LVEF — it should be sought carefully with the bell at the apex in left lateral decubitus. Its presence in a dilated cardiomyopathy patient does not change the diagnosis, but its disappearance with treatment (diuresis) is a useful response marker. S4 (heard in late diastole, presystolic; "Ten-nes-see" cadence at the apex) signals diastolic dysfunction and impaired LV compliance — most common in hypertensive heart disease. An aortic ejection systolic murmur at the right 2nd ICS radiating to the carotids identifies aortic stenosis as a potential aetiology of HF (pressure overload, LVH). A pan-systolic murmur at the apex radiating to the axilla identifies mitral regurgitation — which may be the primary valvular problem (rheumatic, prolapse, chordal rupture) or a secondary finding in dilated cardiomyopathy (functional MR from annular dilatation). An early diastolic decrescendo murmur at the left sternal border (Erb's point, 3rd ICS LSB), best heard with the patient sitting forward in full expiration, identifies aortic regurgitation. A mid-diastolic rumbling murmur at the apex with an opening snap identifies mitral stenosis — the rheumatic aetiology that remains prevalent in India.
Respiratory and peripheral signs. Fine bilateral basal crepitations (fine, inspiratory, not clearing with cough, heard in the lowest 2–3 intercostal spaces posteriorly) reflect pulmonary oedema — transudation of fluid into the alveoli from elevated pulmonary capillary wedge pressure. Unilateral crepitations suggest pneumonia or pulmonary infarction rather than HF. Bilateral pleural effusions (dullness to percussion, absent breath sounds at the bases) are a sign of chronic heart failure with sodium and water retention. Peripheral pitting oedema — bilateral, symmetrical, pitting (leaves an impression for >5 seconds) — reflects elevated right atrial pressure and systemic venous congestion. A pulsatile hepatomegaly confirms tricuspid regurgitation. Tender hepatomegaly without pulsatility is congestive hepatopathy from right heart failure.
IMGAE_NEEDED: table of cardiac signs and their diagnostic significance in heart failure: columns — sign, underlying mechanism, diagnostic implication, associated aetiology; rows include raised JVP, Kussmaul sign, pulsus paradoxus, pulsus alternans, S3, S4, displaced apex, parasternal heave, pan-systolic murmur at apex, diastolic murmur at LSB, basal crepitations, bilateral pitting oedema
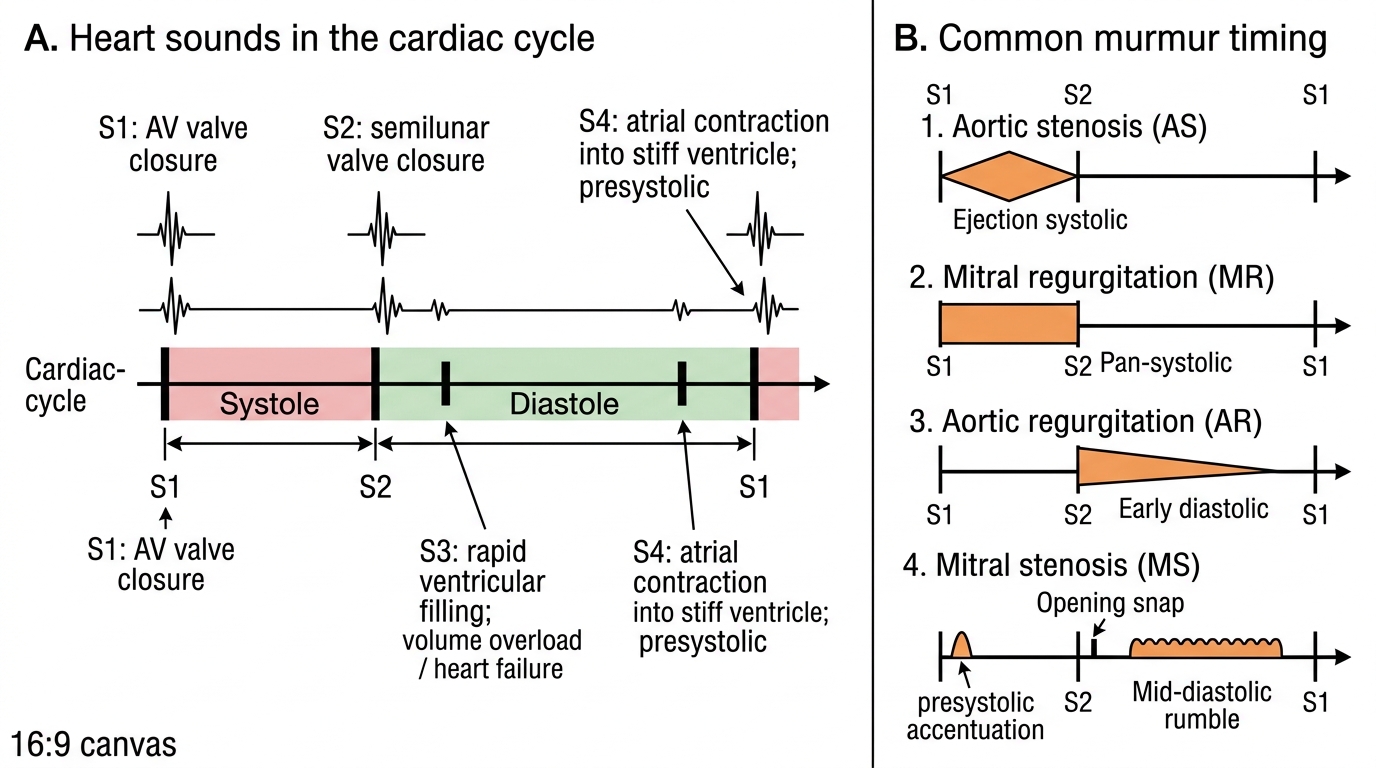
Heart Sounds and Murmur Timing in the Cardiac Cycle
SELF-CHECK
A 52-year-old woman with known rheumatic heart disease is examined. Auscultation reveals a low-pitched, rumbling mid-diastolic murmur at the cardiac apex preceded by an opening snap. The murmur is best heard with the bell of the stethoscope, in the left lateral decubitus position. Which finding would you ALSO expect on examining her JVP waveform?
A. Absent a wave due to atrial fibrillation
B. Giant a wave due to elevated right atrial pressure from pulmonary hypertension
C. Rapid steep y descent consistent with constrictive pericarditis
D. Low-amplitude JVP consistent with reduced right atrial pressure
Reveal Answer
Answer: B. Giant a wave due to elevated right atrial pressure from pulmonary hypertension
The described murmur is mitral stenosis (MS) — mid-diastolic, rumbling, low-pitched, with an opening snap, best heard at the apex in left lateral decubitus with the bell. MS obstructs flow from the left atrium, causing elevated pulmonary venous and pulmonary arterial pressure. Chronic pulmonary hypertension leads to right ventricular hypertrophy and, subsequently, elevated right atrial pressure. In sinus rhythm, the high right atrial pressure is transmitted as a prominent (giant) a wave in the JVP, reflecting forceful right atrial contraction against increased RV afterload. An absent a wave occurs when atrial fibrillation develops (frequent in longstanding MS), not when the patient is in sinus rhythm. A rapid steep y descent is the sign of constrictive pericarditis, not MS. The JVP is not low — it is elevated.
Applied Practice: Integrated Bedside Case with Differential Diagnosis
The highest-level skill in this module is integrating the history and examination findings into a differential diagnosis, prioritising the most likely diagnosis, and identifying the key clinical pointers that support or refute each candidate (IM1.14). This section presents a worked bedside case designed to model the clinical reasoning process you will be expected to perform in your clinical examination and on the ward.
Worked Case. Mr. Arvind Kumar, a 60-year-old retired government officer from Pondicherry, presents with progressive breathlessness over 8 months. He reports dyspnoea on climbing one flight of stairs (previously climbed three flights without difficulty). He has been sleeping on three pillows for the past 6 weeks and woke gasping twice last month (PND). His ankles have been swollen for 3 months. He has no chest pain, no fever. Past history: type 2 diabetes mellitus for 10 years on metformin, hypertension for 12 years (antihypertensives not specified), no known cardiac disease, no history of rheumatic fever, non-smoker, no alcohol. On examination: BP 148/92 mmHg, HR 88 bpm, RR 20/min, SpO2 94% on air. General: moderately breathless at rest, no central cyanosis, no jaundice. JVP 7 cm above the sternal angle at 45°; HJR positive. Pulse: regular, small-volume, no pulsus alternans or paradoxus. Apex beat: 6th ICS, 2 cm lateral to the mid-clavicular line, diffuse and sustained. Parasternal: no heave. Auscultation: normal S1 and S2; S3 present at apex in left lateral decubitus (bell); no murmurs. Lung bases: bilateral fine crepitations to mid-zones posteriorly. Abdomen: liver edge 3 cm below the right costal margin, non-tender, non-pulsatile. Lower limbs: bilateral pitting oedema to the mid-calf, 2+.
Differential diagnosis, prioritised (IM1.14):
- Heart failure with reduced ejection fraction (HFrEF) secondary to hypertensive cardiomyopathy — Most likely diagnosis. The displaced, diffuse, sustained apex beat indicates LV dilatation. S3 is the most specific sign of elevated LV filling pressure and systolic dysfunction. Bilateral raised JVP with HJR indicates right heart failure secondary to the left. Biventricular failure is confirmed by the combination of pulmonary oedema (bilateral crepitations to mid-zones, orthopnoea, PND) and systemic venous congestion (raised JVP, hepatomegaly, bilateral oedema). Longstanding hypertension (12 years) is the most likely aetiology. HFrEF is defined as LVEF ≤40%; HFmrEF as 41–49%; HFpEF as ≥50% — echocardiography is required to classify.
- Heart failure with preserved ejection fraction (HFpEF) secondary to hypertensive diastolic dysfunction — Important to consider, particularly given the hypertensive history. HFpEF would show normal LVEF on echo with diastolic dysfunction markers. The displaced apex, however, strongly favours LV dilatation and HFrEF rather than the concentric LVH of HFpEF. Echocardiography is the definitive investigation.
- Ischaemic cardiomyopathy — Common aetiology in a diabetic, hypertensive, middle-aged man. The absence of chest pain does not exclude silent ischaemia in a diabetic patient (autonomic neuropathy reduces pain perception). Requires coronary evaluation once stabilised.
- Dilated cardiomyopathy (idiopathic) — Characterised by LV dilatation and reduced systolic function without a specific aetiology. The hypertension here provides a clear causal attribution, but if BP has always been well-controlled, idiopathic DCM must be considered.
- Valvular heart disease — No murmur heard (reduces probability of significant valvular pathology as the primary cause), but functional MR (annular dilatation from LV dilatation) can be pan-systolic and relatively soft; echocardiography is essential.
Summary of examination-to-diagnosis mapping for this case:
| Clinical finding | Haemodynamic meaning | Diagnostic implication |
|---|---|---|
| Raised JVP 7 cm + HJR | Elevated RAP, right heart congestion | Right ventricular failure / biventricular failure |
| Displaced diffuse apex 6th ICS | LV dilatation | Volume/pressure overload, DCM, HFrEF |
| S3 at apex | Elevated LV filling pressure | LVEF likely reduced; HFrEF |
| Bilateral crepitations | Pulmonary oedema | Elevated PCWP, left heart failure |
| Bilateral pitting oedema + hepatomegaly | Systemic venous congestion | Right heart failure |
| No murmurs | Valvular disease less likely as primary cause | Look for functional MR on echo |
NYHA Classification in this case: The patient has dyspnoea on climbing one flight of stairs (less-than-ordinary exertion) and symptoms at rest (orthopnoea, PND) → NYHA Class III–IV. Immediate hospitalisation and pharmacological management is indicated.
The worked case illustrates the core principle: no single sign is diagnostic. It is the pattern of multiple concordant signs — a displaced apex + S3 + raised JVP + bilateral oedema + bilateral crepitations — assembled from a systematic history and examination, that generates the confident bedside diagnosis of biventricular heart failure. Each element independently contributes specificity; their concordance is near-diagnostic.
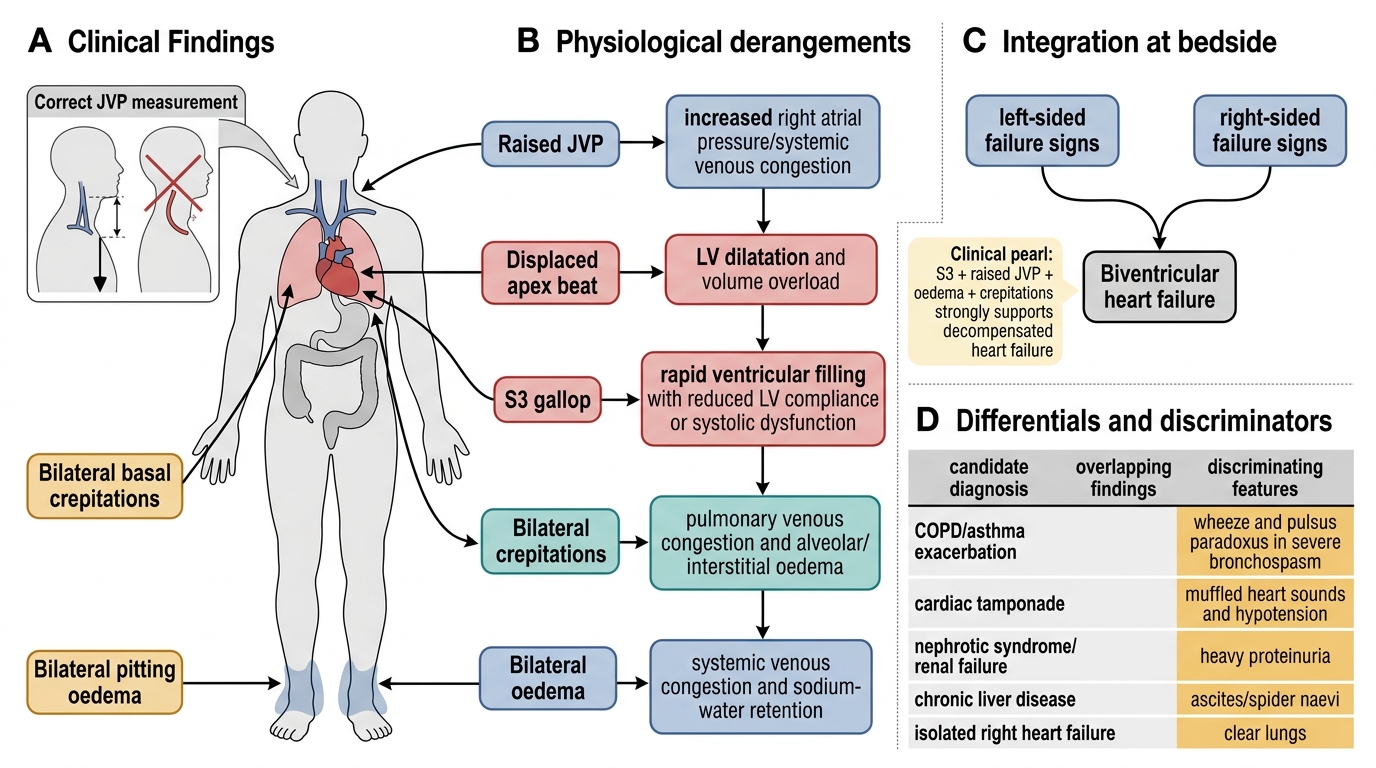
Bedside Reasoning Map for Biventricular Heart Failure
CLINICAL PEARL
The three most discriminating physical signs for elevated left ventricular filling pressure — the haemodynamic hallmark of decompensated heart failure — are: (1) the third heart sound (S3), which has the highest specificity for elevated LV filling pressure and reduced LVEF of any physical sign; (2) a raised JVP, which, when combined with bilateral oedema and pulmonary crepitations, makes the diagnosis of biventricular failure nearly certain at the bedside; and (3) a positive hepatojugular reflux, which adds sensitivity to JVP measurement, particularly when the JVP is only borderline elevated.
A critical bedside technique pitfall: JVP is routinely underestimated when the examiner measures the curved surface distance along the neck instead of the true vertical height from the sternal angle. If the JVP is being measured with a ruler running along the neck, it is wrong — always drop a vertical plumb line from the uppermost pulsation to a horizontal plane at the sternal angle.
And a diagnostic trap: pulsus paradoxus is NOT specific to cardiac tamponade — it also occurs in severe bronchospasm (asthma, COPD exacerbation) and may be absent in tamponade complicated by pre-existing pulmonary hypertension (which increases right-heart stiffness). Never diagnose tamponade on pulsus paradoxus alone; always seek the full Beck's triad and confirm with echocardiography.
Self-Assessment: Testing Your CVS Examination Skills
The self-assessment section consolidates the clinical examination and interpretation skills taught in this module. Work through each question and scenario independently before reading the explanation. These scenarios are calibrated to final-year MBBS level and the OSCE formats used in clinical examinations. The goal is not merely to identify the correct answer but to reconstruct the reasoning chain: which examination finding points to which haemodynamic mechanism, and how does that mechanism integrate into the diagnosis.
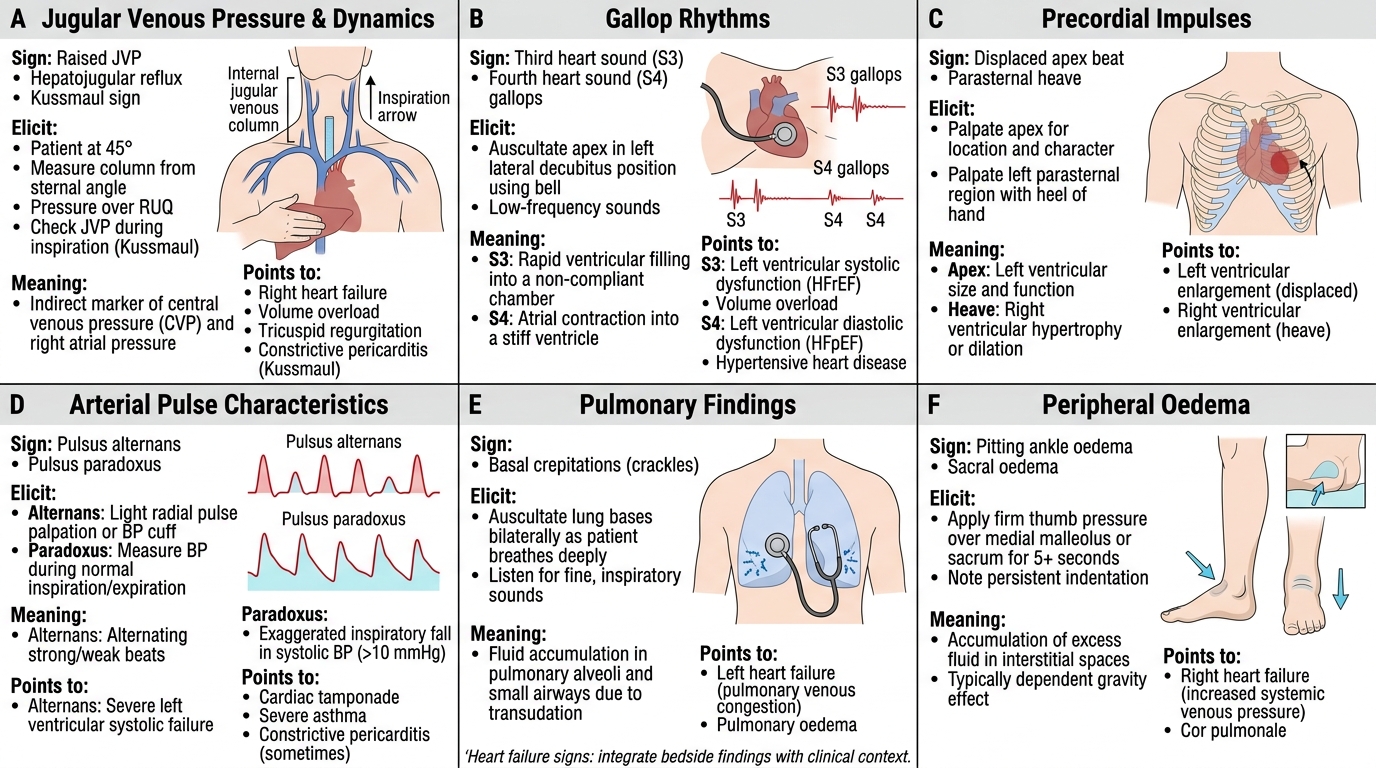
Provided image
Self-assessment scenario 1: Examination interpretation. You are examining a 70-year-old man with known aortic stenosis. On auscultation you find a harsh grade IV/VI ejection systolic murmur at the aortic area, radiating to the carotid arteries. His pulse is slow-rising with a small volume. Systolic BP is 108 mmHg; diastolic is 82 mmHg (pulse pressure 26 mmHg). The apex beat is in the 5th ICS at the MCL, heaving in character, not displaced. There is no S3. JVP is 2 cm above the sternal angle. What does this combination tell you about the severity and stage of the disease? Is there evidence of heart failure?
Analysis: This is a typical pressure-overload LVH without LV dilatation or decompensation. A slow-rising, small-volume pulse with narrow pulse pressure and a non-displaced but heaving apex are the classic signs of severe, compensated aortic stenosis — the ventricle is hypertrophied but not dilated, and the ejection fraction is maintained (no S3, no raised JVP, no peripheral oedema). This represents LVEF-preserved "pre-failure" or early HFpEF. The severity of AS is estimated clinically by the pulse character, the BP, the intensity of A2 (likely reduced or absent in severe AS — check), and the late-peaking character of the systolic murmur. Echocardiography with Doppler will quantify the mean gradient and AVA.
Self-assessment scenario 2: Differential sign interpretation. During a ward round you note a patient with bilateral neck vein distension, hypotension (BP 88/60 mmHg), and muffled heart sounds. The JVP rises on inspiration. There are no crepitations and no peripheral oedema. What is the most likely diagnosis? What is the single most important bedside diagnostic test, and what is the life-saving intervention?
Analysis: This is the classic presentation of cardiac tamponade — Beck's triad (raised JVP, hypotension, muffled heart sounds) + Kussmaul's sign (JVP rises on inspiration, the opposite of normal) + pulsus paradoxus (should be confirmed on sphygmomanometry). The absence of crepitations or oedema distinguishes this from biventricular failure. The single most important bedside test is a 12-lead ECG to show electrical alternans (alternating QRS axis height/morphology in 50% of tamponade cases), followed immediately by bedside echocardiography (pericardial effusion with RV diastolic collapse). The life-saving intervention is pericardiocentesis — ultrasound-guided needle drainage of the pericardial fluid.
Self-assessment scenario 3: Murmur timing. A 35-year-old woman from rural Tamil Nadu presents with exertional dyspnoea and an audible murmur. On examination: mid-diastolic rumble at the apex with an opening snap; tapping apex beat in the 5th ICS MCL; loud S1. She has a malar flush. Her JVP shows a prominent a wave. She is in sinus rhythm. What is the diagnosis, and what does the loud S1 tell you about the severity of the valve lesion?
Analysis: This is rheumatic mitral stenosis — the opening snap (high-pitched sound in early diastole), mid-diastolic rumble at the apex (best heard in left lateral decubitus with the bell), tapping apex (non-displaced; the valve leaflets are immobile in severe MS, transmitting a "tapping" impulse), loud S1 (pliable, mobile leaflets close with a snap — loud S1 is a sign of mobile leaflets, paradoxically suggesting mild-to-moderate rather than severe MS; as the disease advances and leaflets calcify, S1 softens and the opening snap-to-S2 interval shortens), and malar flush ("mitral facies" from low cardiac output and peripheral vasoconstriction). The prominent a wave in the JVP indicates pulmonary hypertension from the longstanding obstruction. The closer the opening snap is to S2, the higher the left atrial pressure and the more severe the stenosis.
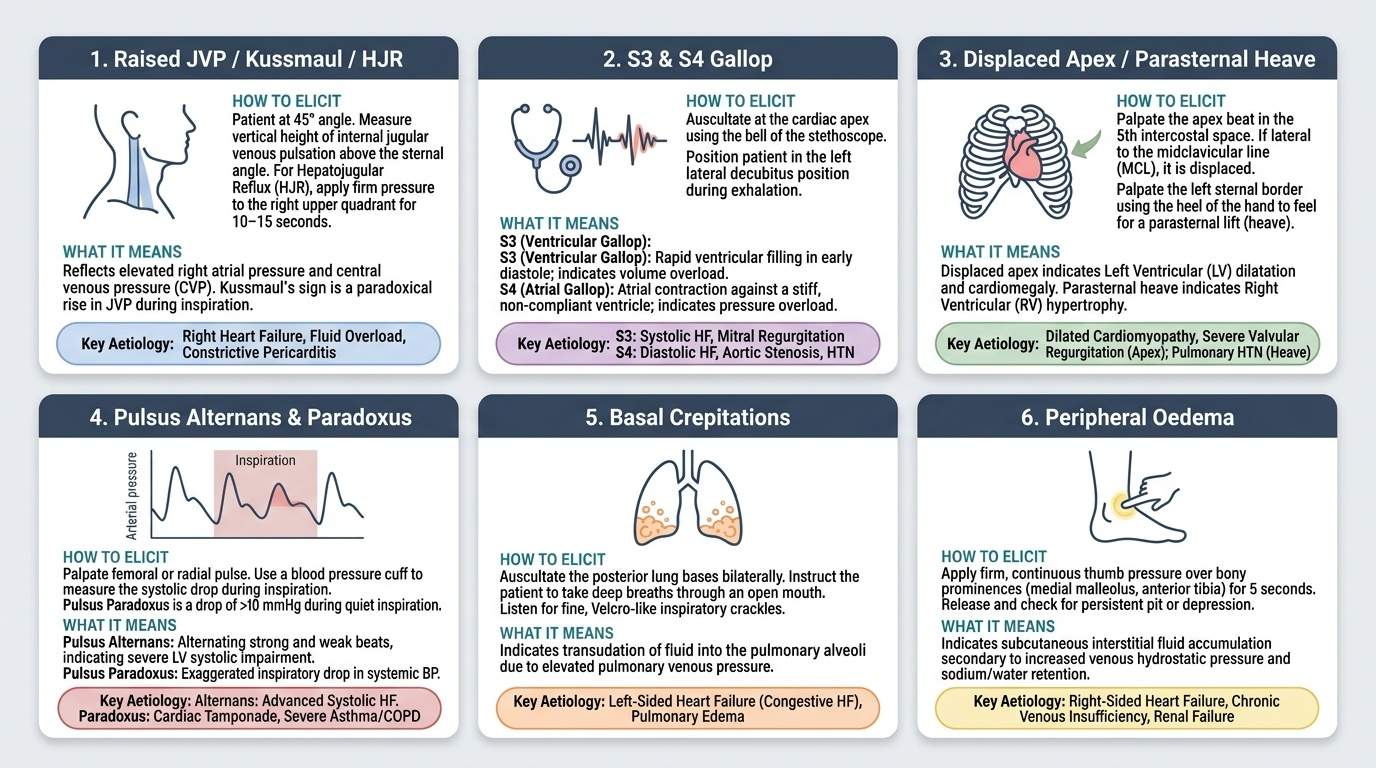
Key Physical Signs of Heart Failure
SELF-CHECK
A 48-year-old man with known ischaemic cardiomyopathy is being followed up in the cardiology clinic. On examination, his pulse is regular with a rate of 92 bpm. You notice that the radial pulse alternates between stronger and weaker beats in every other cycle, in regular sinus rhythm. His JVP is 6 cm above the sternal angle and basal crepitations are present. Which sign does this alternating pulse represent, and what is its clinical significance?
A. Pulsus paradoxus; confirms cardiac tamponade
B. Bigeminy; confirms frequent ventricular ectopics
C. Pulsus alternans; indicates severely impaired left ventricular systolic function
D. Pulsus bisferiens; indicates hypertrophic obstructive cardiomyopathy
Reveal Answer
Answer: C. Pulsus alternans; indicates severely impaired left ventricular systolic function
Pulsus alternans describes alternating strong and weak beats occurring in regular sinus rhythm. It reflects severe LV systolic dysfunction — the failing ventricle cannot maintain a consistent stroke volume on a beat-to-beat basis. It is typically associated with an LVEF well below 30% and indicates advanced HFrEF. It should be distinguished from bigeminy (premature ventricular contractions, which produce an irregular rhythm) and pulsus paradoxus (inspiratory drop in systolic BP, seen in tamponade and severe bronchospasm). Pulsus bisferiens is a double-peaked pulse seen in HOCM or combined AR and AS — a different character altogether, not alternating amplitude.
SELF-CHECK
During a cardiovascular examination for suspected heart failure, you wish to detect a third heart sound (S3). Which of the following techniques will maximise your ability to hear it?
A. Diaphragm of the stethoscope, aortic area, patient sitting forward
B. Bell of the stethoscope, mitral area (cardiac apex), patient in left lateral decubitus position
C. Diaphragm of the stethoscope, pulmonary area, patient supine
D. Bell of the stethoscope, tricuspid area, patient sitting upright
Reveal Answer
Answer: B. Bell of the stethoscope, mitral area (cardiac apex), patient in left lateral decubitus position
S3 is a low-frequency sound generated in early diastole by rapid ventricular filling in a dilated, non-compliant left ventricle. Because it is low-frequency, it is best heard with the bell (which transmits low frequencies) rather than the diaphragm. The mitral area (cardiac apex, 5th ICS MCL) overlies the LV — the chamber generating the S3. The left lateral decubitus position brings the LV closer to the chest wall, amplifying the sound. Sitting forward accentuates aortic regurgitation (early diastolic murmur). The aortic area and pulmonary area are not appropriate locations for S3.