Page 14 of 23
IM10.17-22 | AKI and CKD Management — SDL Guide (Part 2)
CKD Supportive Therapy — Comprehensive Management
CKD management is a multi-target intervention that simultaneously addresses cardiovascular risk reduction, slowing of GFR decline, and treatment of the complications that accumulate as nephron mass falls. This section covers the pharmacological management of each major complication domain in CKD, corresponding to IM10.20.
Provided image
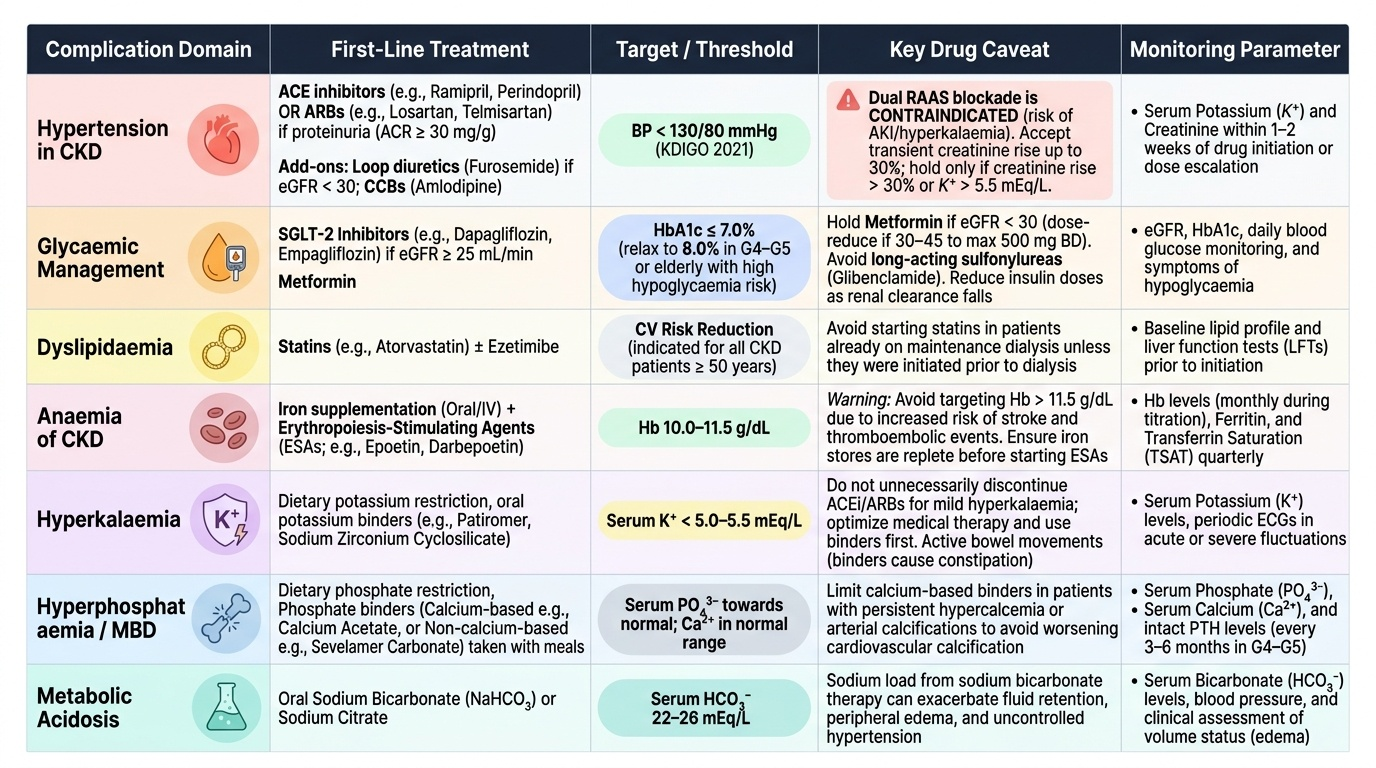
Hypertension in CKD: Target BP <130/80 mmHg (KDIGO 2021 update — applies regardless of proteinuria status). First-line agent with proteinuria (ACR >30 mg/g): ACE inhibitor (e.g., ramipril, perindopril) or ARB (e.g., losartan, telmisartan) — reduce intraglomerular pressure and proteinuria independent of BP effect. Titrate to maximum tolerated dose. Monitor potassium and creatinine within 1–2 weeks of initiation or dose increase. A transient rise in creatinine of up to 30% after starting ACE inhibitor/ARB is acceptable (indicates haemodynamic effect, not true worsening) — hold only if creatinine rises >30% or K⁺ >5.5 mEq/L. Dual RAAS blockade (ACE inhibitor + ARB) is CONTRAINDICATED (ONTARGET trial — increased AKI and hyperkalaemia). Additional agents: loop diuretics (furosemide — preferred over thiazides when eGFR <30); calcium channel blockers (amlodipine — well-tolerated, additive with RAAS blockade); beta-blockers (carvedilol, bisoprolol) for heart failure comorbidity.
Glycaemic management in CKD: HbA1c target <7.0% in most CKD patients; relax to <8.0% in G4–G5 or in elderly patients with hypoglycaemia risk (impaired glucagon response + reduced insulin clearance). Key drug considerations: (1) Metformin — hold at eGFR <30, dose-reduce at eGFR 30–45 (maximum 500 mg BD); (2) SGLT-2 inhibitors (dapagliflozin, empagliflozin) — first-line in CKD with T2DM or proteinuria (eGFR ≥25 for dapagliflozin per DAPA-CKD), primary renoprotective mechanism is tubuloglomerular feedback suppression; (3) GLP-1 receptor agonists (semaglutide, dulaglutide) — emerging renoprotective data, beneficial cardiovascular profile; (4) Sulfonylureas — use shorter-acting agents (gliclazide MR preferred), avoid glibenclamide (prolonged hypoglycaemia from active metabolite accumulation); (5) Insulin — reduce dose as CKD advances (reduced renal insulin clearance).
Dyslipidaemia in CKD: Cardiovascular risk is substantially elevated in CKD. KDIGO 2013 lipid guideline: statins ± ezetimibe in all CKD patients ≥50 years and in younger patients with cardiovascular disease or high cardiovascular risk. Atorvastatin and rosuvastatin are preferred (predominantly hepatically metabolised, safer in CKD). Do not start statins de novo in dialysis patients unless already established (the 4D and AURORA trials showed no benefit in incident dialysis, but statins already being taken should be continued).
Anaemia management: Correct iron first (IV iron if TSAT <20% or ferritin <100 ng/mL, or in dialysis patients); target ferritin 100–500 ng/mL and TSAT 20–40%. Add ESA if Hb <10 g/dL despite iron repletion; target Hb 10–11.5 g/dL (avoid ≥13 g/dL). ESA options in India: epoetin-alpha/beta SC 3× weekly or darbepoetin-alpha SC once every 1–2 weeks. ESA hyporesponsiveness (failure to reach target Hb despite escalating doses) must trigger a search for iron deficiency, infection/inflammation, occult blood loss, B12/folate deficiency, or PTH-mediated bone marrow suppression.
Hyperkalaemia management in CKD: Dietary restriction as above. For persistent elevation: loop diuretics (if residual renal function); sodium bicarbonate supplementation to correct acidosis (shifts K⁺ into cells); new potassium binders — patiromer or sodium zirconium cyclosilicate (ZS-9) for CKD outpatients (better tolerated than Resonium, no sorbitol-associated GI injury); dialysis if refractory or if indication for dialysis independently exists.
Hyperphosphataemia and CKD-MBD management: Dietary phosphate restriction + phosphate binders with meals. Calcium-based binders (calcium carbonate 500 mg TID with food) are first-line but limit total elemental calcium to <1.5 g/day — excess worsens vascular calcification. Non-calcium binders (sevelamer carbonate 800 mg TID with food, or lanthanum carbonate) preferred in patients with hypercalcaemia, Ca×PO₄ product >55, or existing vascular calcification. Cinacalcet (calcimimetic — sensitises calcium-sensing receptor on parathyroid cells; reduces PTH without raising Ca or PO₄) for secondary hyperparathyroidism in dialysis patients with PTH >300 pg/mL. Calcitriol or alfacalcidol for patients with low calcitriol and secondary hyperparathyroidism — titrate to suppress PTH but avoid hypercalcaemia. Monitor PTH, Ca, PO₄, and 25-OHD every 3–6 months in G3–G5.
Metabolic acidosis in CKD: Sodium bicarbonate supplementation (starting at 0.5–1.0 mEq/kg/day, titrated to serum bicarbonate >22 mEq/L) slows CKD progression by reducing acid-mediated tubulointerstitial injury (the AURA and other trials). Avoid in volume-overloaded patients (sodium load). Baking soda (sodium bicarbonate powder) is an inexpensive and widely available supplementation option in India.
SELF-CHECK
A 55-year-old patient with CKD G3b/A3 and eGFR 38 mL/min/1.73 m² is started on ramipril 5 mg/day. At the 2-week review, serum creatinine has risen from 1.8 to 2.3 mg/dL and potassium from 4.8 to 5.3 mEq/L. What is the appropriate response?
A. Stop ramipril immediately as the rise in creatinine indicates worsening kidney disease
B. Continue ramipril — a creatinine rise up to 30% is acceptable as a haemodynamic effect of RAAS blockade
C. Switch ramipril to an ARB to avoid the creatinine rise
D. Add a potassium supplement to counteract the ACE inhibitor effect
Reveal Answer
Answer: B. Continue ramipril — a creatinine rise up to 30% is acceptable as a haemodynamic effect of RAAS blockade
A creatinine rise up to 30% after starting an ACE inhibitor or ARB in CKD is expected and acceptable — it reflects the intended haemodynamic effect (reduced efferent arteriolar tone → lower intraglomerular pressure), not true nephrotoxicity. The creatinine has risen from 1.8 to 2.3 mg/dL = a 28% rise — within the acceptable threshold. Potassium of 5.3 mEq/L is also within acceptable limits (hold only if K⁺ >5.5 mEq/L). Stopping ramipril at this point deprives the patient of the most important nephroprotective treatment in proteinuric CKD. Switching to an ARB provides the same haemodynamic effect. A potassium supplement would be dangerous — ACE inhibitors already raise potassium.
CLINICAL PEARL
The NSAID-free prescribing principle must be actively enforced in every patient with CKD and AKI. NSAIDs block renal prostaglandin production, causing afferent arteriolar vasoconstriction that reduces GFR dramatically — even a single dose of ibuprofen in a volume-depleted CKD patient can precipitate acute-on-chronic renal failure. In India, NSAIDs are widely available over the counter and are frequently self-prescribed for back pain, arthritis, and fever. Every patient with CKD must be explicitly told: 'No ibuprofen, no diclofenac, no naproxen — ever. Not even one tablet. For pain, use paracetamol at the lowest effective dose.' This message needs reinforcement at every visit, because patients often receive NSAIDs from pharmacies, other prescribers, or traditional practitioners without being aware they have been told to avoid them.
Indications for Dialysis and Renal Replacement Therapy
The decision to initiate renal replacement therapy (RRT) is one of the most consequential clinical decisions in nephrology — both in the acute setting (AKI) and in the long-term management of ESRD (CKD G5). Knowing the indications, the modalities, and the timing is the substance of IM10.21 and IM10.22 at the KH level. This is also among the most examined topics in final-year vivas and written papers. The critical conceptual point that underpins all RRT decision-making is that dialysis is a supportive measure — it maintains homeostasis while the kidney either recovers (in AKI) or while the patient awaits transplantation or continues on long-term maintenance therapy (in ESRD). It does not treat the underlying disease, and the decision to initiate it should be driven by clinical criteria — not by arbitrary creatinine or urea thresholds. The AEIOU mnemonic captures five categories of clinical indication, each with specific quantitative thresholds and clinical signs that trigger the decision. The four modalities of RRT — intermittent haemodialysis, peritoneal dialysis, continuous renal replacement therapy, and kidney transplantation — each have distinct mechanisms, patient populations, and settings where they are preferred.
Indications for Dialysis — The AEIOU Framework (AKI and CKD G5):
- A — Acidosis: Severe metabolic acidosis (pH <7.1 or HCO₃⁻ <10 mEq/L) refractory to bicarbonate supplementation. In CKD, the indication applies when acidosis cannot be managed with oral bicarbonate. In AKI, it applies when the acidosis rate of worsening outpaces the liver's compensatory gluconeogenesis and the lungs' respiratory compensation.
- E — Electrolyte disturbance: Hyperkalaemia refractory to medical management (calcium gluconate, insulin/dextrose, Resonium) — specifically K⁺ >6.5 mEq/L with ECG changes or K⁺ >7.0 mEq/L regardless of ECG. Hypo- or hypernatraemia (Na <115 or >165 mEq/L) refractory to safe correction.
- I — Intoxication: Dialysable toxins include: salicylates (aspirin overdose — haemodialysis removes it efficiently; indication: salicylate >7.2 mmol/L with severe acidosis or encephalopathy), methanol and ethylene glycol (toxic alcohols; haemodialysis removes the compound and its toxic metabolites — formic acid from methanol, oxalate from ethylene glycol), lithium (toxicity in psychiatric patients — high volume of distribution but haemodialysis indicated for levels >4 mEq/L or severe encephalopathy), and valproate (selected severe overdoses). Note: organophosphate poisoning is NOT managed with dialysis (atropine + pralidoxime); paracetamol is NOT routinely dialysed (N-acetylcysteine is the antidote).
- O — Overload: Fluid overload causing pulmonary oedema refractory to IV furosemide (particularly in anuric AKI or advanced CKD where diuretics are ineffective). This is an indication for ultrafiltration via CRRT (fluid removal) even in the absence of other dialysis indications.
- U — Uraemia: Symptomatic uraemia — pericarditis (a pericardial friction rub in an AKI/CKD patient is a dialysis indication without waiting for further deterioration), uraemic encephalopathy (confusion, asterixis, seizures from uraemia), uraemic bleeding (GI or other bleeding from platelet dysfunction refractory to DDAVP and cryoprecipitate), and intractable nausea/vomiting preventing adequate nutrition. An arbitrary serum urea threshold (e.g., >150–200 mg/dL or creatinine >10 mg/dL) is NOT a dialysis indication in itself — the clinical syndrome of uraemia, not the number, triggers the decision.
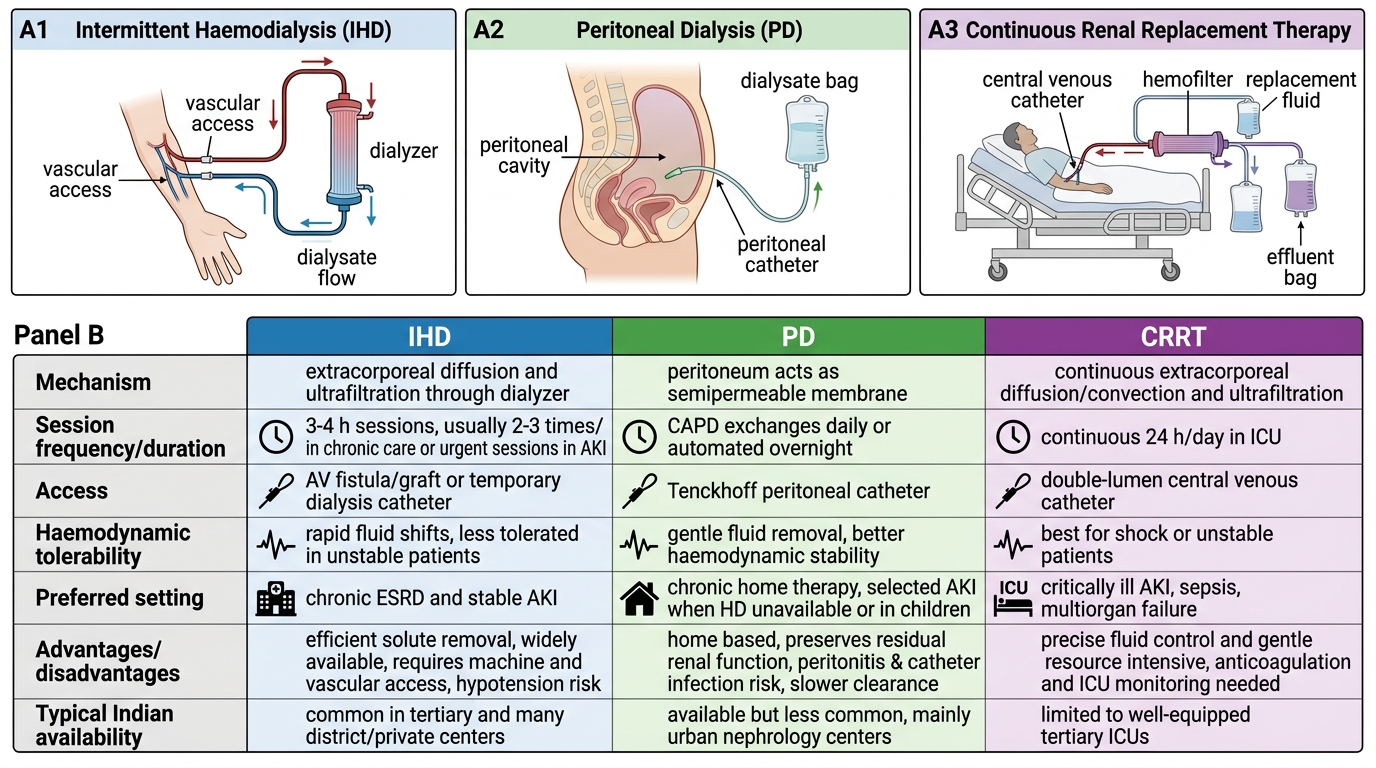
Modalities of Renal Replacement Therapy:
- Intermittent haemodialysis (IHD): Most common RRT modality for chronic ESRD. Sessions typically 3–4 hours, 3× per week (more frequent if residual renal function absent). Requires arteriovenous fistula (AVF — the gold standard permanent access, created 3–6 months in advance), AV graft, or tunnelled central venous catheter as vascular access. AVF should be planned early in CKD G4 to allow maturation time. In AKI, temporary dialysis access via non-tunnelled or tunnelled central venous catheter (right internal jugular preferred; left internal jugular second choice; femoral last resort — highest infection risk).
- Peritoneal dialysis (PD): Uses the peritoneum as the dialysis membrane; dialysate instilled into the peritoneal cavity, allowed to dwell, then drained. Continuous ambulatory PD (CAPD) = 4 manual exchanges/day; automated PD (APD) via machine overnight. Advantages: home-based, preserves residual renal function longer, no need for vascular access, preferred in patients with cardiovascular instability. Contraindications: prior extensive abdominal surgery, active abdominal infection, respiratory compromise (increased intra-abdominal pressure worsens breathing).
- Continuous renal replacement therapy (CRRT): Indicated in haemodynamically unstable patients (hypotensive, vasopressor-dependent) who cannot tolerate the rapid fluid shifts of IHD. Provides slow, continuous fluid and solute removal over 24 hours. Modalities: CVVH (continuous venovenous haemofiltration), CVVHD (continuous haemodialysis), CVVHDF (continuous haemodiafiltration). Preferred in ICU settings for AKI. Requires continuous anticoagulation (unfractionated heparin or regional citrate anticoagulation).
- Kidney transplantation: The optimal long-term RRT for eligible ESRD patients. Provides superior quality of life and survival compared to dialysis. Living-donor transplant outcomes are better than deceased-donor. Early referral to transplant centre is essential — ideally when eGFR reaches 20 mL/min ('pre-emptive transplant listing'). In India, the Transplantation of Human Organs Act (THOA 1994, amended 2011) governs deceased-donor donation and living-related/unrelated donor transplantation with ZTCC/authorisation committee oversight.
Comparison of Dialysis Modalities