Page 10 of 23
IM10.12-16 | Renal Failure Diagnostic Testing — SDL Guide
Learning Objectives
- Select the appropriate diagnostic workup for renal failure based on the presumed aetiology category
- Interpret renal function tests, calcium, phosphorus, PTH, urine electrolytes, osmolality, anion gap, FENa, CrCl, and renal ultrasound findings
- Identify ECG changes characteristic of hyperkalaemia and correlate with serum potassium levels
- Describe the indications for and technique of arterial blood gas measurement
- Describe the indications for peripheral intravenous catheter insertion in renal failure management
INSTRUCTIONS
Diagnostic testing in renal failure is not a blanket panel but a targeted, hypothesis-driven sequence. This module covers the interpretation of each key test used in IM10.12–10.16 at the SH and KH levels, from basic renal function tests through ECG hyperkalaemia patterns to practical procedural indications.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 307–308 — AKI and CKD (textbook)
- API Textbook of Medicine, 10th ed., Ch. Nephrology — Investigations in Renal Disease (textbook)
- Davidson's Principles & Practice of Medicine, 23rd ed., Ch. 17 — Laboratory Assessment in Kidney Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The nurse hands you a set of blood results for a 58-year-old man admitted 6 hours ago with oliguria. Creatinine 3.8 mg/dL, potassium 6.8 mEq/L, bicarbonate 14 mEq/L, urea 98 mg/dL. The urinalysis report says 'granular casts noted.' The ECG printout shows peaked T-waves and a QRS width of 130 ms. Which of these findings represents the most immediate danger to the patient's life? The potassium-ECG combination — but only if you can read it correctly. How do you calculate the FENa to confirm that this is ATN rather than pre-renal? What does the bicarbonate of 14 tell you about the anion gap, and why does that matter for the treatment plan? And when the patient's oxygen saturation drops to 93% and he becomes more confused, what are the indications for an arterial blood gas, and why does the venous blood gas not suffice? The diagnostic workup of renal failure is not a matter of ordering every available test — it is a matter of interpreting each test correctly, in the right sequence, to answer the specific clinical question that it was ordered to answer. This module teaches you to do exactly that.
WHY THIS MATTERS
For the NMC competencies IM10.12 (SH), IM10.13 (KH), IM10.14 (SH), IM10.15 (P), and IM10.16 (P), you must be able to select the appropriate diagnostic workup based on the clinical hypothesis; interpret each renal investigation individually and as a pattern; identify life-threatening ECG findings from hyperkalaemia; and describe the indications for and procedural aspects of arterial blood gas sampling and peripheral IV catheter insertion. These competencies are tested in OSCEs (procedural and interpretation stations), written examinations (spot diagnosis ECG), and clinical vivas.
RECALL
From the previous modules, recall: (1) the pre-renal/intrinsic/post-renal classification and the expected laboratory profiles for each; (2) the KDIGO AKI staging criteria using serum creatinine; (3) the AEIOU indications for dialysis — the investigations in this module provide the specific thresholds that trigger each of the AEIOU criteria. Recall also that the anion gap = [Na⁺] − ([Cl⁻] + [HCO₃⁻]), normal 8–12 mEq/L; an elevated anion gap indicates accumulation of unmeasured anions such as lactate, ketones, or uraemic organic acids. In CKD, a normal anion gap (hyperchloraemic) metabolic acidosis occurs first (from impaired NH₄⁺ excretion), followed by a high anion gap metabolic acidosis in advanced disease (from accumulation of phosphate, sulphate, and organic acids).
Clinical Indication for Diagnostic Workup Selection
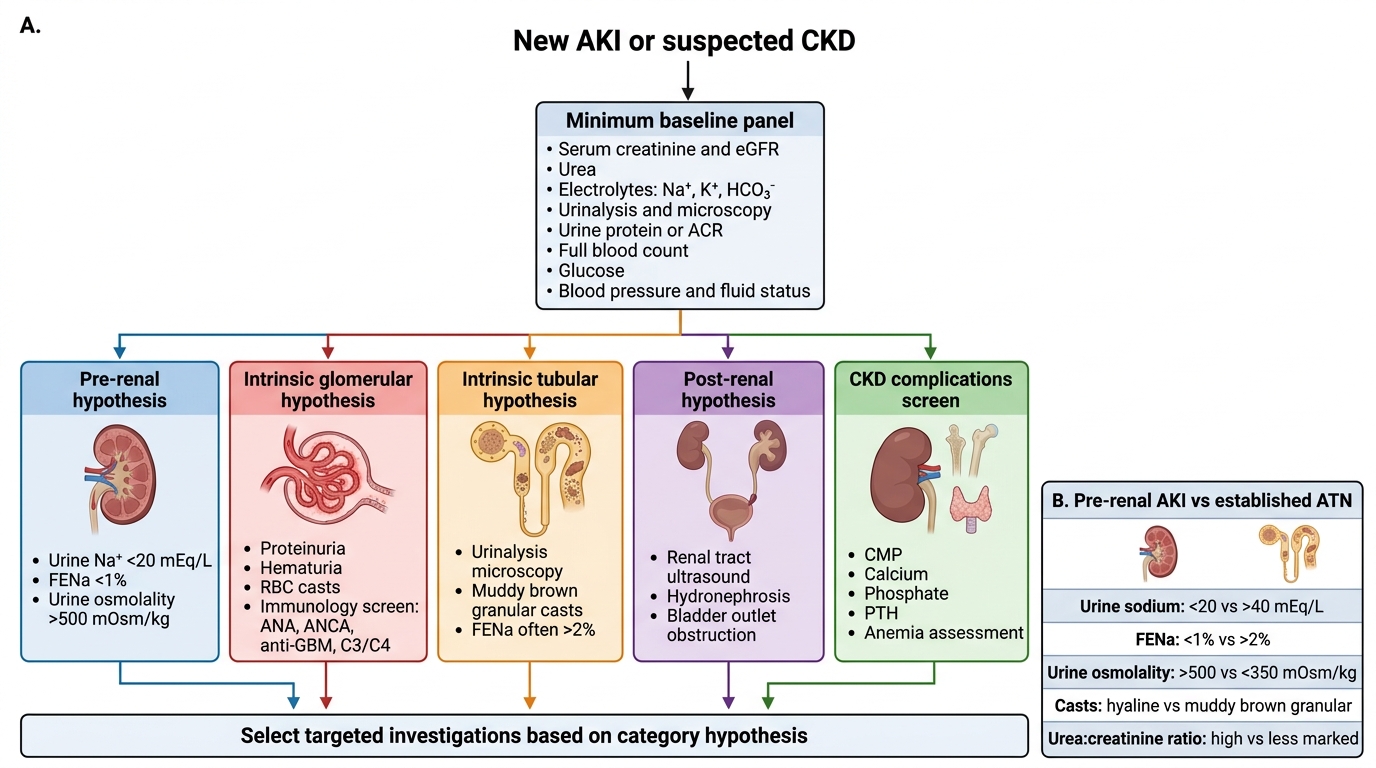
Diagnostic testing in renal failure serves four specific purposes: confirming the diagnosis and staging (is this AKI? which KDIGO stage?), localising the category and aetiology (pre-renal vs intrinsic vs post-renal — and the specific cause within each), monitoring for life-threatening complications (hyperkalaemia, metabolic acidosis, volume status), and guiding decisions about specific interventions (dialysis, immunosuppression, nephrotoxin dose adjustment).
The principle of hypothesis-driven investigation means that each test ordered should be selected because it will change or confirm the working diagnosis. The minimum essential first-line investigation panel in any patient with newly identified AKI or decompensated CKD comprises: serum creatinine and eGFR, serum electrolytes (Na⁺, K⁺, Cl⁻, HCO₃⁻), blood urea nitrogen (BUN or serum urea), full blood count (anaemia, infection), renal ultrasound (size, echogenicity, obstruction), and urinalysis with microscopy (casts, protein, blood). Beyond this baseline, investigations are selected by category hypothesis: suspected pre-renal → urine sodium, urine osmolality, FENa; suspected intrinsic glomerular → complement C3/C4, ANA, ANCA, anti-GBM, serum protein electrophoresis; suspected obstructive post-renal → ultrasound (already in baseline panel); suspected CKD complications → calcium, phosphate, PTH, 25-OHD, lipids, HbA1c.
The clinical indication for an arterial blood gas (ABG) specifically is any one of: dyspnoea or hypoxia (SpO₂ <92%) in a patient with renal failure (pulmonary oedema, metabolic acidosis causing hyperventilation, or uraemic pleuritis), need to precisely quantify the degree of metabolic acidosis (for dialysis decision, bicarbonate therapy decision, or Kussmaul breathing assessment), or confusion with uncertain cause (hypoxia, CO₂ retention, or metabolic acidosis). A venous blood gas (VBG) is adequate for monitoring trends in acid-base in stable patients but overestimates pCO₂ by approximately 4–6 mmHg and underestimates pO₂ significantly — it cannot reliably assess oxygenation. A peripheral IV catheter is indicated in every patient with AKI requiring IV fluid resuscitation, IV medications (furosemide, insulin-dextrose for hyperkalaemia, calcium gluconate, IV antibiotics), or IV access for emergency interventions.
Investigation Selection Algorithm for AKI and CKD
Renal Function Tests — Creatinine, Urea, and Derived Indices
Serum creatinine is the most widely used clinical marker of GFR, but its limitations are critical to understand. Creatinine is produced by muscle metabolism at a relatively constant rate and is freely filtered at the glomerulus. At stable state, serum creatinine is inversely proportional to GFR — but it is affected by muscle mass (lower in women, elderly, malnourished patients — a creatinine of 1.0 mg/dL in a frail 80-year-old woman may represent an eGFR of 30 mL/min), dietary protein intake (high meat intake transiently raises creatinine), and medications (trimethoprim and cimetidine inhibit tubular secretion of creatinine, raising serum creatinine without affecting true GFR). The eGFR, calculated by the CKD-EPI equation, partially corrects for these variables using age and sex.
Provided image
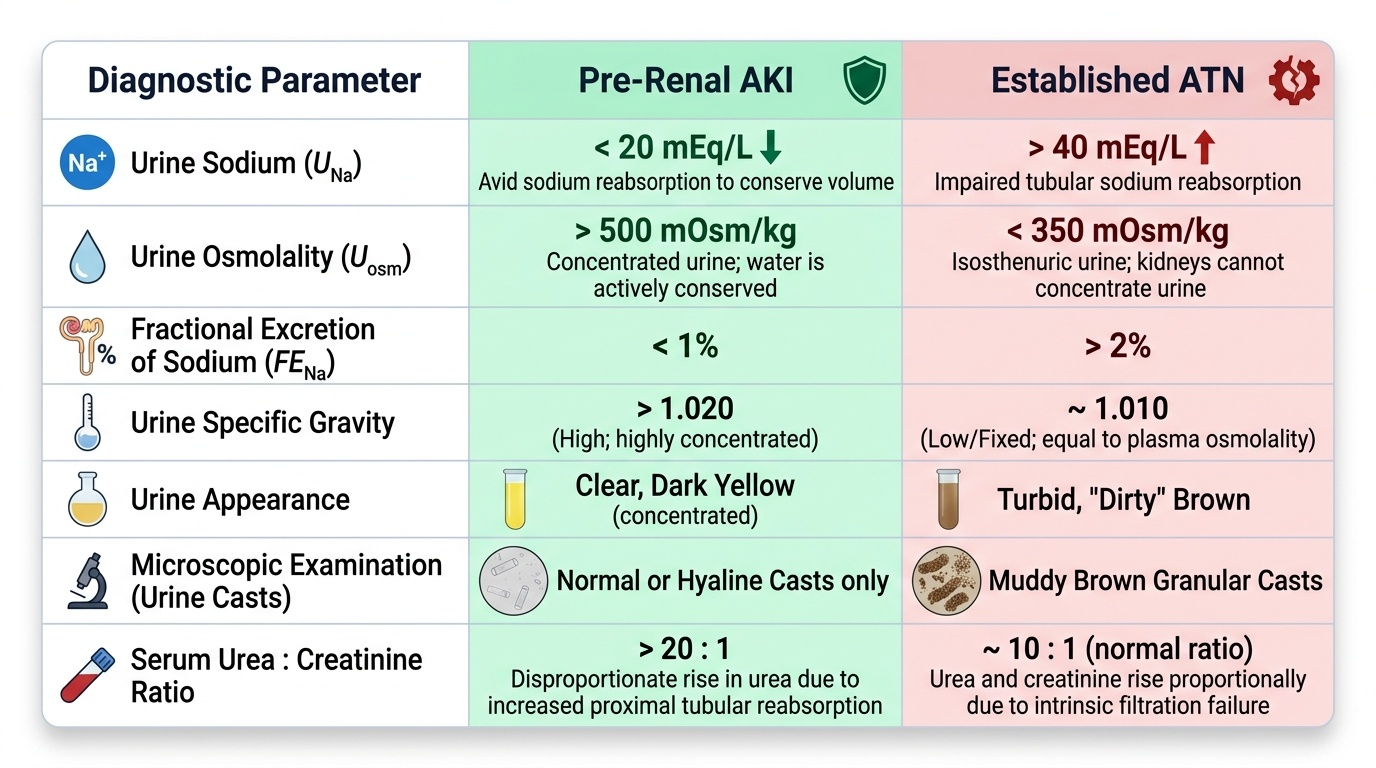
Serum urea (BUN) reflects the end-product of protein catabolism and is filtered, partially reabsorbed (50%), and partially tubularly secreted. In pre-renal AKI, urea reabsorption increases disproportionately as the tubule attempts to conserve sodium and water, raising the urea:creatinine ratio to >20:1 (normal ~10:1). This is a useful diagnostic clue: a urea:creatinine ratio >20 (using mg/dL units; or urea:creatinine >100 in µmol/L SI units) suggests pre-renal AKI, gastrointestinal haemorrhage (blood is digested to urea — GI bleed is a common cause of disproportionate urea elevation), or increased protein catabolism (steroids, catabolic illness). A ratio <10 in the context of AKI suggests intrinsic renal disease or reduced protein intake.
Creatinine clearance (CrCl) estimates GFR using the Cockcroft-Gault formula: CrCl = [(140 − age) × weight (kg)] / [72 × serum creatinine (mg/dL)] × 0.85 for females. Though largely replaced by eGFR in clinical practice, Cockcroft-Gault remains the standard for drug dose adjustment in renal failure — most pharmacokinetic studies establishing dose-reduction thresholds were conducted using Cockcroft-Gault, not CKD-EPI. The key applications are: aminoglycoside dosing, vancomycin dosing, and drug labelling for agents like metformin (stop <30 mL/min) and enoxaparin (dose-reduce or monitor anti-Xa levels).
Urine electrolytes and osmolality are the biochemical counterparts of the clinical volume assessment. In pre-renal AKI, the tubules are intact and conserving sodium maximally: urine sodium is low (<20 mEq/L) and urine osmolality is high (>500 mOsm/kg) and urine specific gravity is high (>1.020). In established ATN, tubular function is lost — sodium conservation fails, urine sodium rises (>40 mEq/L), and the urine is dilute (osmolality <350 mOsm/kg, specific gravity ~1.010). The fractional excretion of sodium (FENa) integrates these: FENa (%) = [(urine Na × plasma creatinine) / (plasma Na × urine creatinine)] × 100. FENa <1% = pre-renal (tubular function intact, conserving sodium); FENa >2% = ATN (tubular function lost). Important caveat: FENa is unreliable in: patients on diuretics (forced sodium excretion → spuriously elevated FENa), non-oliguric ATN (FENa may be 1–2%), and acute contrast nephropathy (contrast causes vasoconstriction but tubular function may still be preserved early — FENa may be <1%). In these situations, fractional excretion of urea (FEUrea) is an alternative: FEUrea <35% suggests pre-renal even in patients on diuretics.
SELF-CHECK
A patient with AKI has the following urine values: urine sodium 12 mEq/L, urine creatinine 240 mg/dL, serum sodium 138 mEq/L, serum creatinine 3.6 mg/dL. What is the FENa, and what does it indicate?
A. FENa 0.35%; pre-renal AKI — tubules conserving sodium normally
B. FENa 2.4%; ATN — tubules unable to conserve sodium
C. FENa 0.35%; ATN — tubular injury causing sodium wasting
D. FENa 2.4%; pre-renal — tubuloglomerular feedback activated
Reveal Answer
Answer: A. FENa 0.35%; pre-renal AKI — tubules conserving sodium normally
FENa = [(urine Na × plasma creatinine) / (plasma Na × urine creatinine)] × 100 = [(12 × 3.6) / (138 × 240)] × 100 = [43.2 / 33,120] × 100 = 0.13% — just under 0.35% using approximation; the answer closest to the correct calculation is option A at FENa <1%, indicating pre-renal AKI. The kidney is avidly conserving sodium (low urine Na = 12 mEq/L), consistent with intact tubular function responding to reduced perfusion. FENa <1% = pre-renal (tubular function intact, sodium reabsorption intact). FENa >2% = ATN (tubular function lost). This patient needs volume resuscitation, not further investigation for intrinsic disease.
Calcium, Phosphorus, PTH, and Anion Gap Interpretation
Beyond the core renal function tests, several additional biochemical investigations are essential in renal failure — each answering a specific clinical question related to complications management.
Calcium and Phosphorus: In CKD, as GFR falls, phosphate retention and reduced calcitriol production lower ionised calcium (hypocalcaemia). Measure serum total calcium and serum phosphate together. Correct serum calcium for albumin: corrected Ca = measured Ca + 0.8 × (4.0 − serum albumin in g/dL); a hypoalbuminaemic patient's true calcium is higher than the measured value. The calcium-phosphate product (Ca × PO₄, in mg²/dL²) is an important risk marker: a product >55 mg²/dL² is associated with extraskeletal and vascular calcification — this is the threshold that mandates intensification of phosphate-lowering treatment. Hypercalcaemia in CKD-MBD suggests tertiary hyperparathyroidism (autonomous PTH secretion), aluminium toxicity (from aluminium-based antacids — now uncommon), or excessive vitamin D supplementation. Hypocalcaemia in acute renal failure (particularly in rhabdomyolysis) results from calcium precipitation into injured muscle and may worsen cardiac function.
Serum PTH: Measure intact PTH (iPTH) by second-generation ECLIA or ELISA assay. In secondary hyperparathyroidism of CKD, PTH rises progressively from G3 onwards. Target PTH levels in CKD differ by stage: for G3–G4, maintain PTH within the 2–9× upper limit of normal (to prevent both bone disease and adynamic bone disease from over-suppression); for dialysis patients (G5D), the KDIGO target is iPTH 2–9× ULN (approximately 150–600 pg/mL, institution-dependent). Markedly elevated PTH (>800–1000 pg/mL) with hypercalcaemia and hyperphosphataemia in a dialysis patient suggests tertiary hyperparathyroidism requiring surgical parathyroidectomy.
Serum 25-hydroxyvitamin D: Measures vitamin D stores (not the active form). In CKD, deficiency of 25-OHD is common (reduced sunlight exposure, dietary restriction) and is a substrate deficiency for the renal 1α-hydroxylase that converts 25-OHD to 1,25-dihydroxyvitamin D (calcitriol). Supplement to ≥30 ng/mL before starting calcitriol analogues.
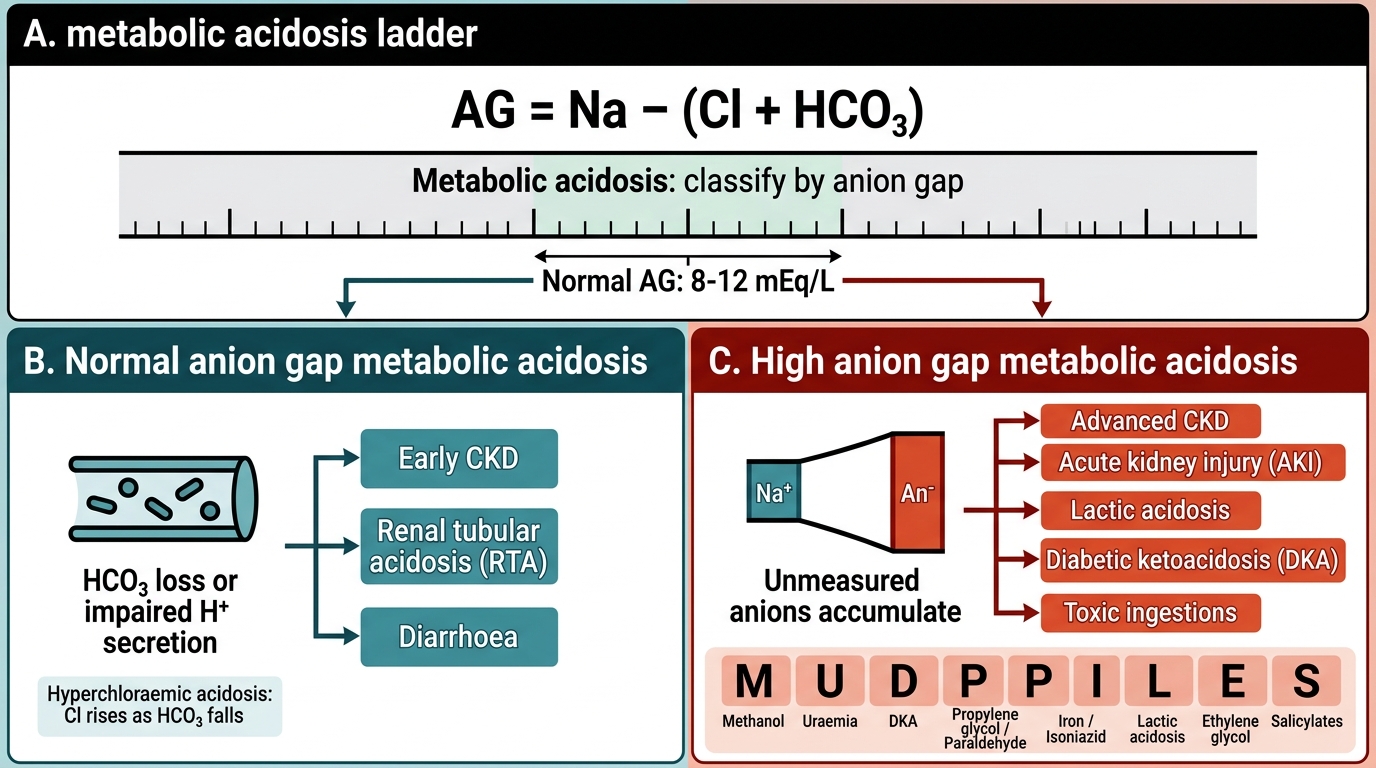
Anion gap (AG) and metabolic acidosis interpretation: AG = [Na⁺] − ([Cl⁻] + [HCO₃⁻]); normal 8–12 mEq/L (with albumin correction: add 2.5 mEq/L per 1 g/dL below normal albumin of 4.0 g/dL). Metabolic acidosis is common in both AKI and advanced CKD. Two distinct patterns occur:
- Normal AG (hyperchloraemic) metabolic acidosis: occurs in early-to-moderate CKD (G2–G4) from impaired ammonium (NH₄⁺) excretion without accumulation of unmeasured anions. AG is normal; HCO₃⁻ is low; Cl⁻ is elevated. Also seen in distal renal tubular acidosis (RTA type 1), proximal RTA (type 2), and diarrhoea. The urine anion gap (UAG = urine Na + urine K − urine Cl) helps distinguish renal from GI bicarbonate loss: positive UAG (>0) = renal origin (inadequate NH₄⁺ excretion); negative UAG (<0) = GI origin (GI loss, diarrhoea).
- Elevated AG metabolic acidosis (HAGMA): occurs in advanced CKD (G4–G5) and AKI from accumulation of phosphate, sulphate, hippurate, and uraemic organic acids. Also the pattern in lactic acidosis (sepsis, metformin toxicity), ketoacidosis (DKA — important differential in diabetic CKD), and toxic alcohol ingestion. The MUDPILES mnemonic covers the differential: Methanol, Uraemia, Diabetic ketoacidosis, Propylene glycol, Isoniazid/Iron, Lactic acidosis, Ethanol (toxic alcohols), Salicylates.
The degree of metabolic acidosis in AKI/CKD is clinically important: a bicarbonate <15 mEq/L with pH <7.2 represents a dangerous acidaemia. Acidosis drives potassium out of cells (each 0.1 unit fall in pH raises serum potassium by approximately 0.3–0.5 mEq/L), worsening hyperkalaemia. Acidosis also contributes to peripheral vasodilatation and myocardial depression. A bicarbonate <10 mEq/L or pH <7.1 refractory to bicarbonate supplementation is an indication for emergency dialysis (the 'A' in AEIOU).
Anion Gap Metabolic Acidosis Ladder