Page 5 of 17
IM12.4-7 | Thyroid Clinical Evaluation — SDL Guide (Part 2)
Interpretation of Clinical Findings and Differential Diagnosis
The clinical findings from the history and examination should be synthesised into a prioritised differential diagnosis before investigations are ordered. This is not merely a list of possibilities — it is a structured ranking based on the symptom pattern, examination findings, and clinical probability. The NMC IM12.7 competency requires you to demonstrate this reasoning process explicitly. The strength of this framework is that it translates the history and examination data you have just collected into a clinically actionable shortlist, guiding the choice of investigations rather than requesting every thyroid test at once. A well-constructed differential diagnosis also prevents anchoring — the cognitive error of committing to the first diagnosis that comes to mind without systematically weighing the alternatives. The two axes that structure the thyroid differential are the direction of dysfunction and the specific aetiology within each direction, as detailed below.
Provided image
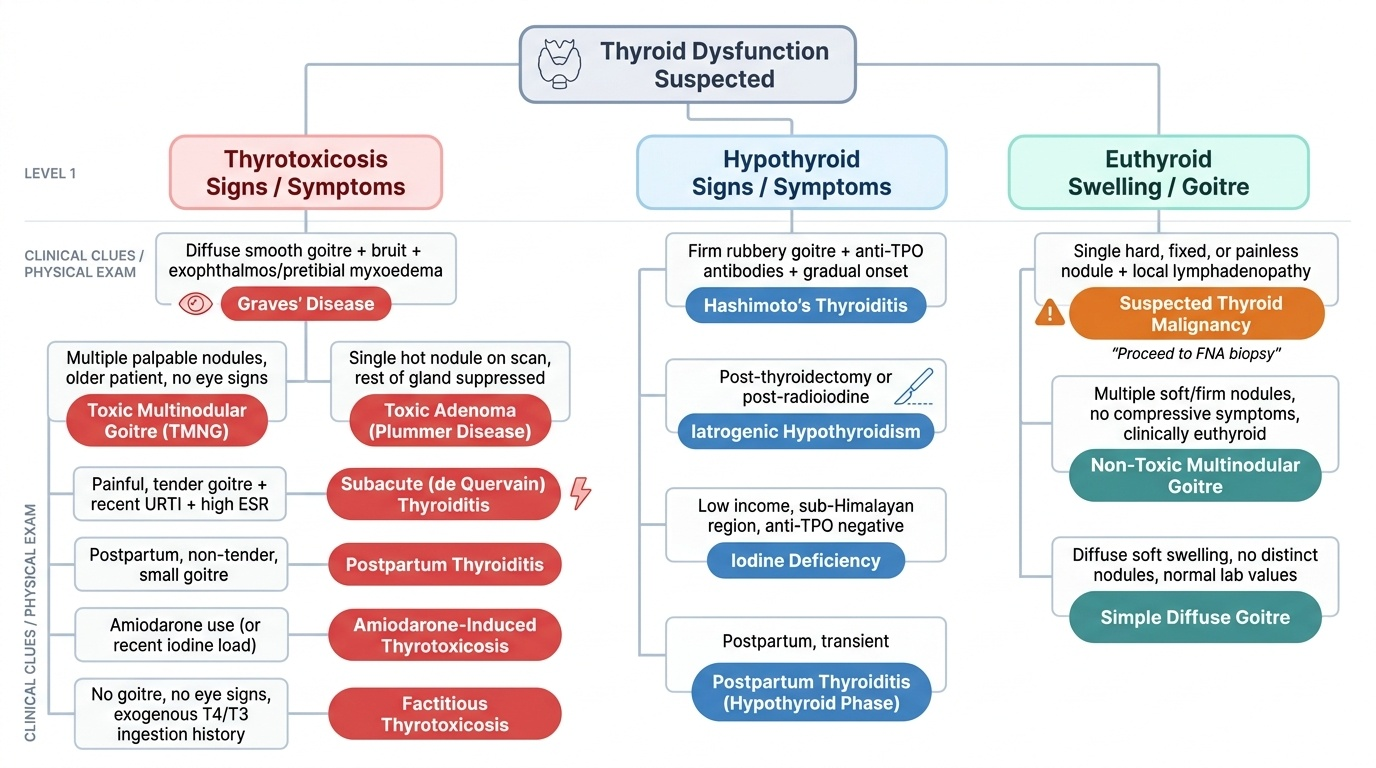
The clinical differential diagnosis framework for thyroid disease rests on two axes: (1) the direction of dysfunction (thyrotoxicosis vs hypothyroidism vs euthyroid goitre/nodule), and (2) within thyrotoxicosis, the aetiology (Graves vs toxic nodular vs thyroiditis vs other). The clinical examination findings directly address both axes.
Thyrotoxicosis differential — clinical clues:
| Clinical finding | Suggested aetiology |
|---|---|
| Diffuse smooth goitre + bruit + exophthalmos/pretibial myxoedema | Graves disease (most likely) |
| Multiple palpable nodules, older patient, no eye signs | Toxic multinodular goitre (TMNG) |
| Single hot nodule on scan, rest of gland suppressed | Toxic adenoma (Plummer disease) |
| Painful, tender goitre + recent URTI + high ESR | Subacute (de Quervain) thyroiditis |
| Postpartum, non-tender, small goitre | Postpartum thyroiditis |
| Amiodarone use (or recent iodine load) | Amiodarone-induced thyrotoxicosis |
| No goitre, no eye signs, exogenous T4/T3 ingestion history | Factitious thyrotoxicosis |
Hypothyroidism differential — clinical clues:
| Clinical finding | Suggested aetiology |
|---|---|
| Firm rubbery goitre + anti-TPO antibodies + gradual onset | Hashimoto thyroiditis (most common) |
| Post-thyroidectomy or post-radioiodine | Iatrogenic hypothyroidism |
| Low income, sub-Himalayan region, anti-TPO negative | Iodine deficiency |
| Postpartum, transient | Postpartum thyroiditis (hypothyroid phase) |
| Amiodarone or lithium use | Drug-induced hypothyroidism |
| Low TSH + low FT4 | Secondary hypothyroidism (pituitary/hypothalamic) — check pituitary MRI |
Euthyroid goitre / thyroid nodule differential:
- Simple (colloid) goitre: Diffuse, soft, non-tender; euthyroid; common in adolescent girls; may respond to iodine if mildly deficient.
- Multinodular goitre: Multiple palpable nodules; euthyroid or mildly toxic; increasing in prevalence with age.
- Thyroid adenoma: Solitary smooth, mobile, firm or soft nodule; follicular adenoma most common; FNAC to exclude malignancy.
- Thyroid carcinoma: Hard, fixed, rapidly growing nodule; associated hoarseness; cervical lymphadenopathy; history of irradiation or family history of MEN2/familial medullary carcinoma. Four main types: papillary (most common, 80%, excellent prognosis), follicular (iodine-deficient areas, vascular invasion distinguishes from adenoma on histology), medullary (calcitonin-secreting, C-cells, MEN2 association), anaplastic (aggressive, older patients, worst prognosis).
- Thyroglossal duct cyst: Midline swelling that moves both on swallowing AND on tongue protrusion — the distinguishing examination finding.
Generating a prioritised differential — clinical reasoning model: After completing the history and examination, state: (1) the most likely diagnosis with supporting clinical evidence, (2) two to three alternative diagnoses, and (3) the one red-flag diagnosis you must exclude first (usually malignancy in a nodule, or thyroid storm in a severely thyrotoxic patient). Example: 'Most likely Graves disease — young woman with tachycardia, tremor, weight loss, diffuse smooth goitre with bruit, lid retraction, and bilateral proptosis. Alternatives: toxic multinodular goitre (less likely — no nodularity, young age), Hashitoxicosis (less likely — usually brief, no bruit or exophthalmos). No red flags for malignancy. Thyroid storm criteria not currently met but monitor closely.'
SELF-CHECK
A 52-year-old man presents with a 3-month history of tremor, weight loss, and diarrhoea. He takes amiodarone for paroxysmal AF diagnosed 6 months ago. On examination: irregularly irregular pulse 118 bpm, bilateral palpable thyroid nodules, no exophthalmos, no bruit. Which diagnosis should be placed FIRST in the differential?
A. Graves disease — most common cause of hyperthyroidism
B. Toxic multinodular goitre complicated or precipitated by amiodarone-induced thyrotoxicosis
C. Subacute thyroiditis — amiodarone causes thyroid inflammation
D. Thyroid carcinoma with functioning metastases
Reveal Answer
Answer: B. Toxic multinodular goitre complicated or precipitated by amiodarone-induced thyrotoxicosis
This patient has multiple palpable nodules (multinodular goitre), is older (52 years), is male, has no eye signs, and no bruit — this profile fits toxic multinodular goitre rather than Graves disease. Amiodarone contains 37% iodine by weight and can precipitate thyrotoxicosis in patients with pre-existing nodular thyroid disease (jod-Basedow phenomenon — iodine load activates autonomous nodules). Amiodarone-induced thyrotoxicosis type I (excess iodine activating autonomous tissue) is the most clinically relevant diagnosis here. Graves disease is less likely — no diffuse smooth goitre, no bruit, no exophthalmos, and older male. Subacute thyroiditis is painful and associated with viral URTI prodrome, not present here. Functioning metastases are rare and would not present this way.
Applied Practice: Case-Based Clinical Reasoning
This section applies the history and examination skills in simulated clinical encounters, mirroring the format of the OSCE and supervised clinical assessments you will face in final year. For each scenario, work through the diagnostic reasoning steps before reading the analysis. Focus on generating a prioritised differential diagnosis, not just identifying a single answer — the ability to reason through alternatives and state your clinical evidence is what separates a competent clinician from a memoriser.
Before the scenarios, a brief review of the most commonly tested clinical sign clusters:
Signs of thyrotoxicosis (exam-critical): Resting tachycardia; irregularly irregular pulse (AF); warm, moist, fine-tremulous hands; onycholysis (Graves); lid retraction and lid lag (any thyrotoxicosis); exophthalmos/proptosis (Graves only); diffuse smooth goitre with bruit (Graves); pretibial myxoedema (Graves only); proximal myopathy (difficulty rising from chair); hyperreflexia.
Signs of hypothyroidism (exam-critical): Bradycardia; dry, coarse, cold skin; periorbital puffiness (mucoid oedema); loss of outer third of eyebrow (Hertoghe sign); firm rubbery goitre (Hashimoto) or no goitre; slow monotonous speech; 'hung-up' slow-relaxing ankle jerks; carpal tunnel signs (Tinel, Phalen); pericardial effusion (muffled heart sounds, raised JVP in severe cases).
Scenario A: A 24-year-old female medical student presents to the OPD complaining of 'heart racing' for 6 weeks. She has lost 5 kg in 2 months without dieting. She is irritable, sweats excessively even in air-conditioned rooms, and her hands shake when she writes. On examination: heart rate 104 bpm (regular), BP 136/62 mmHg, fine resting tremor of outstretched hands, warm moist palms. Neck examination reveals a diffuse smooth goitre with an audible bruit. Eyes: bilateral lid retraction with scleral show, 3 mm bilateral proptosis. Reflexes: brisk. Generate a prioritised differential.
Analysis: Thyrotoxicosis is the diagnosis — tachycardia, tremor, weight loss, heat intolerance, widened pulse pressure (136/62 — elevated systolic, low diastolic), warm moist palms, hyperreflexia. Aetiology: Graves disease — diffuse smooth goitre with bruit + bilateral proptosis (Graves-specific ophthalmopathy, not seen in other causes). Differential: Hashitoxicosis (brief, no bruit or proptosis), toxic adenoma (single nodule, no eye signs). Red flag: none for malignancy; assess for thyroid storm features (high-grade fever, altered consciousness, AF) — currently absent.
Scenario B: A 42-year-old woman is referred by her GP for fatigue, weight gain of 8 kg over 12 months, and feeling 'slowed down'. She also reports heavy periods and constipation. On examination: pulse 52 bpm (regular), BP 108/76 mmHg. Skin dry, cold. Face: periorbital puffiness, sparse outer-third eyebrows. Neck: firm, rubbery, non-tender, moderately enlarged, homogeneous bilateral thyroid. Reflexes: slow relaxing ankle jerks bilaterally. Voice: slightly hoarse. Generate a prioritised differential.
Analysis: Hypothyroidism — bradycardia, cold dry skin, periorbital puffiness, Hertoghe sign (outer eyebrow loss), slow-relaxing reflexes, hoarse voice, constipation, menorrhagia, weight gain. Aetiology: Hashimoto thyroiditis — firm, rubbery, homogeneous goitre in a middle-aged woman with classic hypothyroid features. Differential: iodine deficiency hypothyroidism (less likely in urban India; no antimicrobial antibody expected), iatrogenic (no history of surgery/RAI). Hoarseness must be interpreted carefully — in hypothyroidism, hoarseness results from mucoid deposition in the larynx, not recurrent laryngeal nerve invasion; if malignancy were suspected, a hard fixed nodule and cervical lymphadenopathy would accompany it.
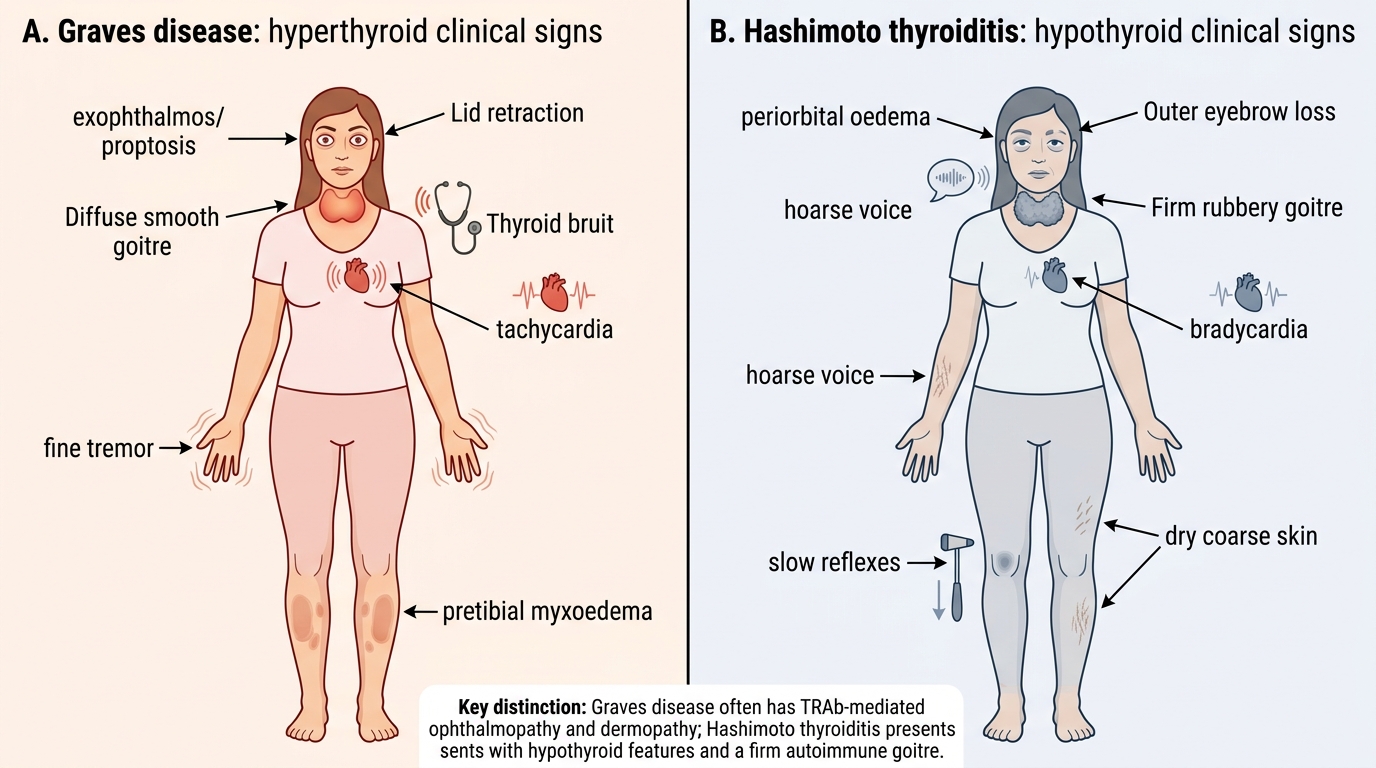
Clinical Signs: Graves Disease vs Hashimoto Thyroiditis
SELF-CHECK
A 38-year-old woman with known Graves disease is found to have bilateral exophthalmos. Her husband reports that her eyes are 'bulging'. This sign (exophthalmos/proptosis) is specific to Graves disease and NOT seen in other causes of hyperthyroidism. What is the mechanism?
A. Elevated TSH directly stimulates orbital fat cell proliferation in any thyrotoxic state
B. TSH receptor antibodies (TRAb) activate TSH receptors on orbital fibroblasts, causing glycosaminoglycan deposition, orbital inflammation, and volume increase that pushes the eyeball forward
C. Excess T3 directly causes orbital muscle hypertrophy in all forms of thyrotoxicosis
D. Lid retraction from sympathetic overactivation creates the false appearance of proptosis in Graves disease
Reveal Answer
Answer: B. TSH receptor antibodies (TRAb) activate TSH receptors on orbital fibroblasts, causing glycosaminoglycan deposition, orbital inflammation, and volume increase that pushes the eyeball forward
Graves ophthalmopathy is caused by TRAb/TSI acting on TSH receptors expressed on orbital fibroblasts. TRAb activation triggers these fibroblasts to proliferate and produce excessive glycosaminoglycans (hyaluronic acid), causing orbital fat and muscle volume expansion. The resulting increase in intraorbital tissue volume displaces the eyeball anteriorly — true proptosis measurable by exophthalmometry (Hertel >21 mm). This is unique to Graves disease because only TRAb (not TSH from a pituitary, nor T3/T4 directly) activates orbital fibroblasts. Lid retraction (option D) is a separate sign — it causes a false appearance of proptosis in minor cases, but true proptosis is an anatomical displacement confirmed by measurement. In non-Graves thyrotoxicosis (toxic adenoma, TMNG), TSH is suppressed and TRAb is absent — lid retraction may be present (sympathetic overactivation), but exophthalmos is not.
CLINICAL PEARL
The most critical distinction in thyroid clinical examination is between Graves disease and all other causes of thyrotoxicosis. Only Graves disease produces exophthalmos (proptosis), a thyroid bruit, and pretibial myxoedema — because these three signs are caused specifically by TRAb acting on orbital fibroblasts, intrathyroidal vasculature, and cutaneous fibroblasts respectively. Lid retraction and lid lag are caused by sympathetic overactivation and are present in ALL forms of thyrotoxicosis. A student who reports 'Graves disease' based only on tachycardia and lid retraction has made an unsupported inference — the definitive clinical diagnosis requires either the bruit, exophthalmos, or pretibial myxoedema (confirmed by TRAb). Similarly, the most commonly missed clinical sign of hypothyroidism is the slow-relaxing ('hung-up') ankle jerk — it is one of the most sensitive physical signs but requires deliberate testing with attention to the relaxation phase, which most students overlook by checking only for presence or absence of the jerk.
Self-Assessment: Clinical Examination Integration
You have now completed the core clinical evaluation module for thyroid disease, covering history-taking, examination technique, sign interpretation, and differential diagnosis generation. The following self-assessment scenarios are designed to test whether you can integrate these skills into a structured clinical response — the format you will use in your OSCE station and in clinical vivas. For each question, formulate your answer independently before reading the analysis. Pay attention to the reasoning process — which clinical features led you to each conclusion — rather than simply identifying the correct diagnosis.
When presented with a thyroid clinical scenario in an examination, use this structured response framework: (1) State the likely diagnosis based on the dominant symptom cluster; (2) List the supporting clinical signs from both history and examination; (3) Name one or two alternative diagnoses and the finding that would distinguish them; (4) Identify any red-flag features and what they would prompt. This framework ensures completeness and demonstrates the diagnostic reasoning that distinguishes a KH/SH level response from a K-level factual recitation.
Question 1: A 65-year-old man is brought to the Emergency Department confused and hypothermic. His temperature is 34.8°C, heart rate 44 bpm, BP 90/60 mmHg, respiratory rate 8 breaths/min. He is drowsy, with periorbital oedema, macroglossia, and dry coarse skin. His wife reports he stopped taking his 'thyroid tablet' 8 weeks ago. What is the diagnosis and what is the immediate life-threatening concern?
Analysis: Myxoedema coma — the most severe form of hypothyroidism, a medical emergency. Features present: hypothermia (the defining temperature abnormality), bradycardia, hypotension, respiratory depression (low RR, CO₂ retention), altered consciousness, periorbital oedema, macroglossia (mucopolysaccharide deposition in the tongue). Precipitant: discontinuation of levothyroxine. Immediate threat: respiratory failure from hypoventilation and CO₂ narcosis (intubation may be required); cardiovascular collapse. Treatment: IV levothyroxine (or liothyronine) + IV hydrocortisone (concurrent adrenal insufficiency must be treated first or it may precipitate adrenal crisis) + supportive care (active rewarming, IV glucose, assisted ventilation as needed).
Question 2: During an OSCE station, you examine a 26-year-old woman with a 2 cm smooth, mobile, non-tender nodule in the right lobe of the thyroid. She is euthyroid. There are no palpable cervical lymph nodes. The examiner asks: 'What is your differential diagnosis and what investigation would you order first?' Give your structured response.
Analysis: Differential — most likely: (1) benign follicular adenoma (most common solitary nodule, typically colloid); (2) dominant nodule in early multinodular goitre; less likely: (3) thyroid cyst (smooth, fluctuant on palpation); (4) thyroid carcinoma (papillary — must be excluded). Red-flag features absent (no hoarseness, no lymphadenopathy, not hard or fixed). First investigation: Thyroid ultrasound (characterises the nodule — solid vs cystic, echogenicity, calcification, margins, vascularity — and classifies risk using ACR-TIRADS scoring). If TIRADS high-risk or solid hypoechoic with irregular margins → ultrasound-guided FNAC (Bethesda cytology classification). TSH should also be ordered — if suppressed, proceed to radionuclide scintigraphy to assess whether the nodule is functioning (hot/autonomous) or non-functioning (cold, higher malignancy risk).