Page 11 of 17
IM12.12-14 | Thyroid Pharmacotherapy and Definitive Therapy — SDL Guide (Part 2)
Definitive Therapy for Thyrotoxicosis: Radioiodine and Surgery
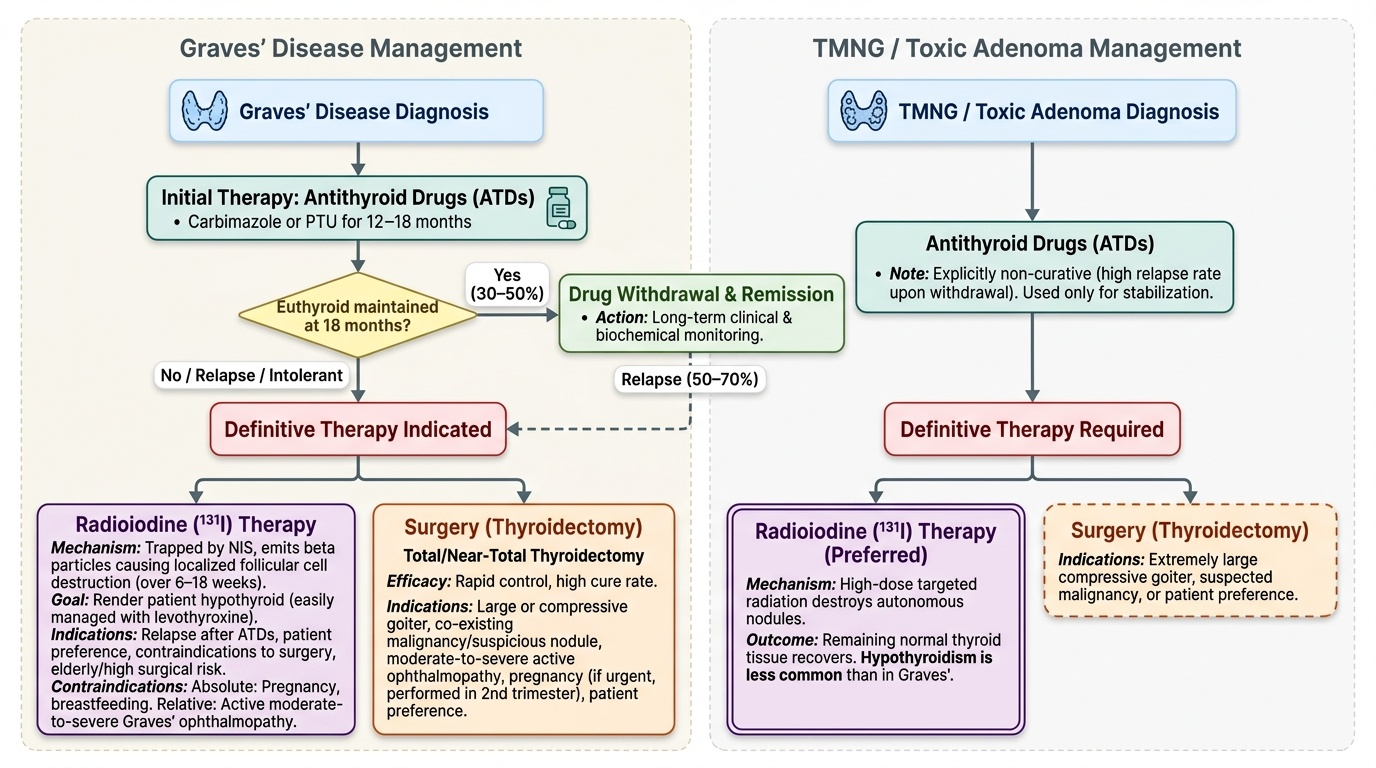
Antithyroid drugs are the initial treatment for most patients with thyrotoxicosis, but they are not curative for Graves disease (50–70% relapse rate after drug withdrawal) and are explicitly non-curative for toxic nodular goitre (TMNG and toxic adenoma always require definitive therapy). Definitive therapy — radioiodine ablation or thyroidectomy — is indicated in specific clinical situations and patient groups. The decision between the two modalities requires weighing efficacy, safety, speed of response, implications for fertility and pregnancy, the presence of co-existing malignancy, and patient preference. The NMC IM12.14 competency requires you to describe and discuss these indications precisely.
Provided image
Radioiodine therapy (¹³¹I):
Mechanism: Oral ¹³¹I is trapped by the sodium-iodide symporter (NIS) and concentrated in thyroid follicular cells (including autonomous nodules). The beta particles emitted by ¹³¹I cause localised radiation thyroiditis and follicular cell destruction — over 6–18 weeks, the gland shrinks and thyroid hormone production falls. The goal in Graves disease is to render the patient hypothyroid (this is the intended endpoint, not a complication — hypothyroidism is easily managed with levothyroxine, while persistent hyperthyroidism is the failure mode).
Indications for radioiodine:
- Graves disease: (1) after first or second relapse following antithyroid drugs; (2) patient choice (preferred option in the USA); (3) when long-term antithyroid drugs are not feasible (allergy, intolerance, non-compliance); (4) toxic adenoma or TMNG (radioiodine has a high success rate for focal autonomous disease); (5) elderly patients with Graves disease who cannot undergo surgery.
- Toxic adenoma: high-dose targeted ¹³¹I destroys the autonomous nodule; the remaining normally-regulated gland tissue recovers (unlike Graves, hypothyroidism is less common as the endpoint).
- TMNG: effective; may need higher doses.
Contraindications to radioiodine:
- Absolute: pregnancy (crosses placenta; fetal thyroid concentrates iodine from week 10–12; causes fetal hypothyroidism and ablates the fetal gland). Breastfeeding (excreted in breast milk). Active significant Graves ophthalmopathy (radioiodine can worsen ophthalmopathy by releasing TRAb and thyroid antigens; relative contraindication — may be used cautiously with concurrent corticosteroids in mild-moderate ophthalmopathy, but surgery or antithyroid drugs preferred in severe eye disease).
- Relative: Large goitre with obstructive symptoms (surgery preferred for rapid decompression); suspected thyroid malignancy (FNAC first); co-existing thyroid nodule requiring FNAC.
Pre-treatment preparation: Antithyroid drugs should be stopped 3–7 days before radioiodine to ensure the gland is iodine-avid (carbimazole reduces NIS expression). After radioiodine, symptom control with beta-blockers is continued. Pregnancy must be excluded before the procedure (mandatory urine or serum β-hCG). Women should avoid pregnancy for at least 6 months after ¹³¹I therapy (radiation safety); the same applies for men (advise to use contraception for 6 months post-treatment).
Thyroidectomy (surgical therapy):
Indications for surgery:
- Large goitre with compressive symptoms (dysphagia, stridor, dyspnoea, superior vena cava compression — surgery provides the fastest relief)
- Graves disease with active severe ophthalmopathy (surgery does not worsen ophthalmopathy, unlike radioiodine)
- Suspected malignancy (concurrent thyroid nodule requiring definitive histology; medullary thyroid carcinoma family history)
- Failure of, or contraindication to, radioiodine and antithyroid drugs
- Patient preference (particularly when rapid definitive cure is desired, or when pregnancy is planned in the near future — can conceive after surgery once euthyroid)
- Pregnancy — second trimester only (if antithyroid drugs cannot control Graves disease adequately; first and third trimester surgery carries increased risk of miscarriage and preterm delivery)
Types of thyroid surgery: Total thyroidectomy (removes both lobes and isthmus) is the procedure of choice for Graves disease — near-total thyroidectomy is an alternative. Hemithyroidectomy (lobectomy) is appropriate for a solitary adenoma confined to one lobe. Complications of thyroidectomy: recurrent laryngeal nerve (RLN) palsy (hoarseness — 1–2% risk in experienced hands), hypoparathyroidism (hypocalcaemia due to parathyroid gland injury or removal — transient in 5–10%, permanent in 1–2%), thyroid storm (if operated without achieving euthyroidism — requires adequate antithyroid drug preparation).
Pre-operative preparation: The patient MUST be rendered euthyroid before surgery with antithyroid drugs (4–8 weeks of carbimazole). Additionally, Lugol's iodine solution (potassium iodide) is given for 10–14 days before surgery to reduce thyroid vascularity (iodine blocks hormone synthesis via the Wolff-Chaikoff effect and causes involution of the gland, reducing operative blood loss). Beta-blockers are continued perioperatively. Failure to achieve pre-operative euthyroidism risks intraoperative or postoperative thyroid storm.
Choice between radioiodine and surgery — a practical framework:
| Clinical scenario | Preferred modality | Rationale |
|---|---|---|
| Graves disease, first relapse, no contraindications | Radioiodine (or patient choice) | Effective, outpatient, no surgical risk |
| Graves disease + severe ophthalmopathy | Surgery (or carbimazole long-term) | RAI worsens eye disease |
| Large compressive goitre | Surgery | Decompression required |
| Suspected malignancy | Surgery | Histology needed |
| Pregnancy (2nd trimester, drug failure) | Surgery (2nd trimester only) | RAI contraindicated in pregnancy |
| Toxic adenoma | Radioiodine | Focal ablation, low hypothyroid risk |
| TMNG | Radioiodine or surgery | Both effective; size and presence of nodules may favour surgery |
| Patient planning pregnancy soon | Surgery | Pregnancy safe ~6 weeks post-op |
SELF-CHECK
A 42-year-old woman with Graves disease has just completed 18 months of carbimazole therapy. Her TRAb remains positive at the end of treatment. She is asking about her options. She has Grade 2 Graves ophthalmopathy (active, moderate-to-severe with clinical activity score 4/7). Which definitive therapy is most appropriate?
A. Radioiodine ablation — most convenient and effective for Graves disease
B. Continue carbimazole for another 12 months before reassessing
C. Total thyroidectomy — preferred when active moderate-to-severe Graves ophthalmopathy is present, as radioiodine can worsen eye disease
D. No further treatment — persistent TRAb is expected and does not require intervention
Reveal Answer
Answer: C. Total thyroidectomy — preferred when active moderate-to-severe Graves ophthalmopathy is present, as radioiodine can worsen eye disease
Active moderate-to-severe Graves ophthalmopathy is a contraindication (or strong relative contraindication) to radioiodine. Radioiodine releases thyroid antigens and potentially increases TRAb levels in the short term, which can exacerbate or trigger worsening of Graves ophthalmopathy. Surgery (total thyroidectomy) removes the antigenic target (the thyroid gland) and has no adverse effect on Graves ophthalmopathy — it is the preferred modality in this clinical scenario. Continuing carbimazole does not address the risk of relapse (which is predicted by persistent TRAb) and is not a definitive approach. Persistent TRAb predicts relapse and mandates a definitive therapy decision.
Thyroid Storm and Myxoedema Coma Management
Thyroid storm and myxoedema coma represent the extreme ends of the thyroid dysfunction spectrum — both are life-threatening medical emergencies requiring immediate, structured, multi-drug intervention. Although management of these emergencies extends beyond the core IM12.12–14 competency set, the pharmacological principles involved draw directly on the drugs covered in this module.
Provided image
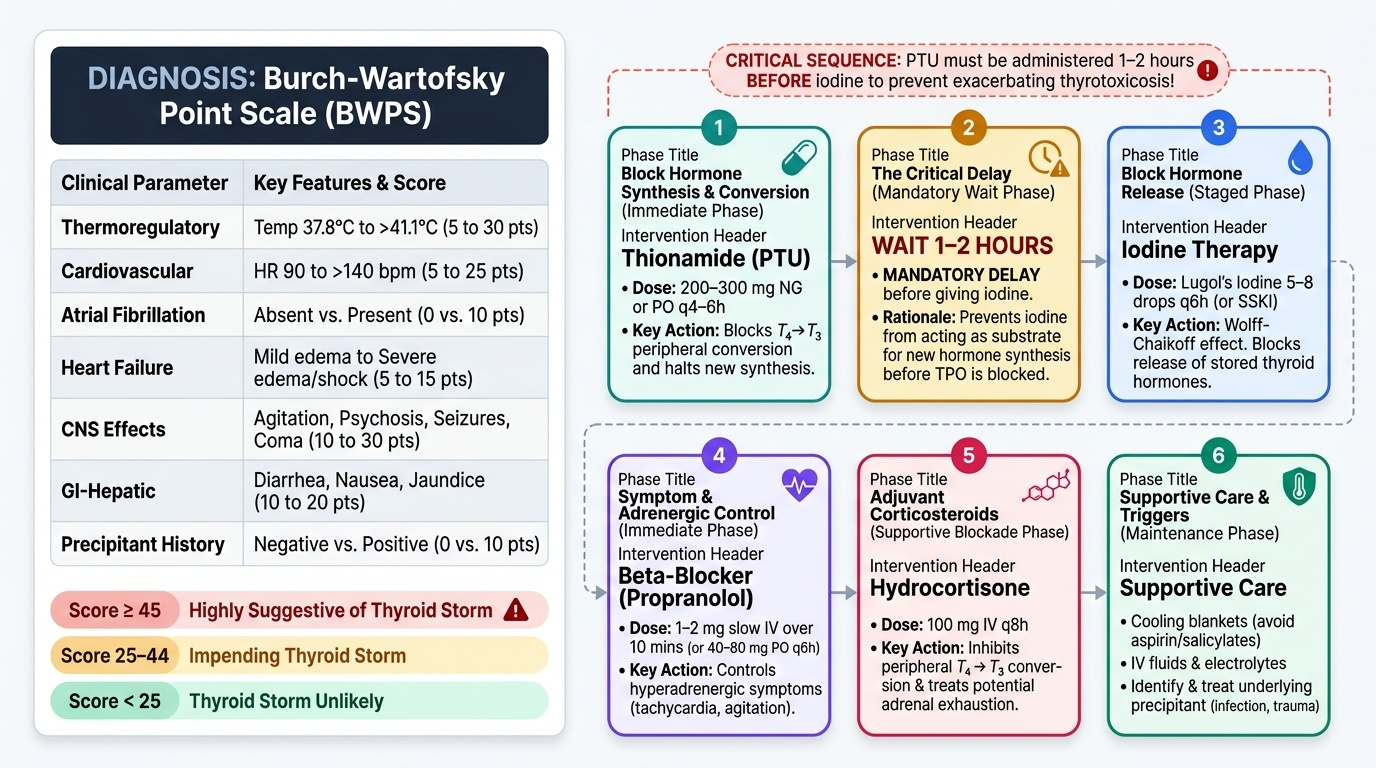
Thyroid storm — Burch-Wartofsky scoring and pharmacological management:
Thyroid storm (thyrotoxic crisis) is an acute, life-threatening exacerbation of thyrotoxicosis characterised by extreme metabolic derangement from uncontrolled excess T3/T4. The Burch-Wartofsky Point Scale (BWPS) is the validated scoring tool: it assigns points for temperature, heart rate, AF, heart failure, CNS effects (agitation, psychosis, seizure, coma), GI dysfunction, and precipitant. A score ≥45 = thyroid storm (highly suggestive); 25–44 = impending storm. Triggers include infection, surgery, trauma, radioiodine, and iodine-containing contrast.
Pharmacological management of thyroid storm (the sequence matters):
1. Thionamide — PTU first: Give PTU 200–300 mg orally or via nasogastric tube every 4–6 hours. PTU is preferred over carbimazole in thyroid storm because it ALSO inhibits peripheral deiodination (reducing T4→T3 conversion), providing a faster reduction in active T3. Carbimazole can be used if PTU is unavailable.
2. Iodine — AFTER PTU (1–2 hours later): Give Lugol's iodine solution (5–8 drops every 6 hours) or potassium iodide (SSKI). Iodine inhibits thyroglobulin proteolysis (blocking release of stored hormone — the Wolff-Chaikoff effect) AND inhibits new hormone synthesis. Iodine must be given after PTU — if given before, the excess iodine can provide substrate for further hormone synthesis by a TPO that has not yet been blocked.
3. Beta-blocker — propranolol: Give IV propranolol 1–2 mg slowly over 10 minutes (or oral 40–80 mg every 6 hours if the patient can swallow). Controls adrenergic symptoms (tachycardia, AF, tremor) and — uniquely among beta-blockers — also inhibits peripheral T4→T3 conversion (large doses). Target heart rate reduction. Avoid in asthma (use diltiazem instead); use with caution in decompensated heart failure.
4. Corticosteroids: Give IV hydrocortisone 100 mg every 8 hours (or IV dexamethasone 2 mg every 6 hours). Two rationales: (a) concurrent relative adrenal insufficiency is common in thyroid storm (accelerated cortisol clearance by excess T3); (b) corticosteroids independently inhibit peripheral T4→T3 conversion, reducing active T3 levels.
5. Supportive care: IV fluids (significant volume deficit from sweating, diarrhoea, and hyperthermia); active cooling (paracetamol + tepid sponging — NOT aspirin, which displaces T4 from TBG and transiently worsens thyrotoxicosis); high-calorie nutrition; monitoring for and treating precipitating infection.
6. ICU admission: Thyroid storm has a mortality rate of 10–30% even with treatment; ICU-level monitoring is mandatory.
Myxoedema coma — pharmacological management:
Myxoedema coma is the most severe form of hypothyroidism: altered consciousness, hypothermia, bradycardia, hypotension, hypoventilation (CO₂ retention), and myxoedematous features. Mortality remains 20–40% even with treatment.
Treatment sequence:
1. Airway and ventilation first: Intubation and mechanical ventilation if GCS is significantly impaired or PaCO₂ is rising.
2. Hydrocortisone before thyroid hormone: Give IV hydrocortisone 100 mg every 8 hours immediately. In myxoedema coma, concurrent adrenal insufficiency must be assumed and treated first — starting T4 first accelerates cortisol clearance and can precipitate life-threatening adrenal crisis.
3. IV levothyroxine: Give IV levothyroxine 200–500 µg as a loading dose, then 50–100 µg/day IV until the patient can take oral medication. IV formulation is used because gut motility is often severely impaired in myxoedema (oral absorption unreliable). Some authorities add small doses of IV liothyronine (T3) for faster action, but this is controversial and carries cardiac risk.
4. Active rewarming: Passive (warm blankets) rather than active external rewarming (which can cause peripheral vasodilation and worsening hypotension) is preferred. Correct hypothermia gradually.
5. Precipitant identification and treatment: The trigger for myxoedema coma must be identified and treated — most commonly infection (sepsis, pneumonia), cold exposure, sedative/analgesic drugs, or discontinuation of levothyroxine.
SELF-CHECK
A patient with thyroid storm is being treated in the ICU. The treating team plans to give Lugol's iodine to block thyroid hormone release. At what point in the management sequence should Lugol's iodine be given, and why?
A. Before any other treatment — iodine blocks hormone synthesis most rapidly
B. Simultaneously with the antithyroid drug for maximum combined effect
C. At least 1–2 hours AFTER administering propylthiouracil (PTU), to ensure TPO is already inhibited before iodine is given
D. Lugol's iodine is contraindicated in thyroid storm and should not be used
Reveal Answer
Answer: C. At least 1–2 hours AFTER administering propylthiouracil (PTU), to ensure TPO is already inhibited before iodine is given
Lugol's iodine must be given at least 1–2 hours AFTER PTU (or carbimazole) has been administered. The reason is sequencing of mechanism: if iodine is given first, the additional iodine substrate floods the gland and can actually stimulate further hormone synthesis in the unblocked thyroid (the enzyme TPO remains active and can organify the excess iodine). PTU must first block TPO (preventing new hormone synthesis) before iodine is introduced. Once TPO is blocked, the iodine provides the additional benefit of inhibiting thyroglobulin proteolysis (blocking release of stored hormone — the acute Wolff-Chaikoff effect). Giving iodine before the thionamide is a dangerous and well-documented error in thyroid storm management.
Self-Assessment: Treatment Decision Integration
This final section consolidates the pharmacological and treatment decision competencies from this module through structured clinical scenarios. For each case, work through the treatment algorithm independently before reading the analysis. The scenarios are designed to require you to integrate drug selection (carbimazole vs PTU, levothyroxine dosing), the indication for definitive therapy, and the management of acute complications — the full spectrum of IM12.12, IM12.13, and IM12.14. Pay particular attention to the clinical reasoning behind drug sequencing and patient-specific adjustments — these are the most commonly examined aspects of thyroid pharmacotherapy in both written and clinical examinations. Each scenario has been constructed to test a decision point where the wrong choice causes direct patient harm, reinforcing the principle that pharmacological precision in thyroid disease is not academic but clinically consequential. The three rules highlighted below are the most commonly examined in undergraduate and postgraduate assessments and should be recalled automatically in the relevant clinical context.
Before the scenarios, a concise summary of the three key treatment decision rules:
- Rule 1 — First trimester pregnancy + hyperthyroidism = PTU (not carbimazole; embryopathy risk)
- Rule 2 — Graves ophthalmopathy (active, moderate-to-severe) + need for definitive therapy = Surgery (not radioiodine; worsens ophthalmopathy)
- Rule 3 — Thyroid storm sequence = PTU first → iodine 1–2h later → propranolol → hydrocortisone (iodine given before PTU = dangerous error)
Scenario A: A 48-year-old woman with Graves disease has relapsed after two courses of carbimazole over 5 years. She has no significant ophthalmopathy (NOSPECS grade 1), no significant goitre, and no cardiac disease. She is not pregnant and has completed her family. Which definitive therapy do you recommend and what pre-treatment is required?
Analysis: Radioiodine ablation is appropriate: second relapse of Graves disease in a non-pregnant woman with minimal ophthalmopathy and no contraindications. Pre-treatment: ensure euthyroidism before administration (β-hCG negative, no active ophthalmopathy to worsen). Stop carbimazole 3–7 days before radioiodine (to restore NIS expression and maximise uptake). Continue beta-blockers for symptom control. Post-treatment: expect euthyroidism or hypothyroidism within 6–12 weeks; monitor TSH monthly for first 3 months, then 3-monthly. Start levothyroxine when TSH rises above normal or when hypothyroid symptoms develop.
Scenario B: A 68-year-old man with heart failure (NYHA Class II) and paroxysmal AF is found to have TSH 18 mIU/L and FT4 7.2 pmol/L. His physician plans to start levothyroxine. What dose and monitoring plan do you prescribe?
Analysis: This is overt primary hypothyroidism in an elderly patient with significant cardiac comorbidity (heart failure + AF). The standard dose calculation (1.6 µg/kg) cannot be used here — start low and slow: levothyroxine 25 µg/day. The rationale: sudden normalisation of thyroid hormone in this patient could precipitate AF exacerbation, angina, or heart failure decompensation by increasing myocardial oxygen demand and heart rate. Titrate by 25 µg every 6–8 weeks, targeting TSH in the normal range. Communication: take in the morning on an empty stomach; separate from his AF medications (if he takes digoxin, note that levothyroxine increases digoxin clearance — digoxin levels may need adjustment; if he takes warfarin, T4 accelerates warfarin catabolism, potentially reducing INR — recheck INR after dose changes). Monitor: TSH + ECG after 6 weeks and after each dose change.
Scenario C: A 16-year-old girl is started on carbimazole 20 mg/day for Graves disease. Four weeks later she attends the Emergency Department with a 2-day history of fever, sore throat, and aphthous ulcers. Carbimazole was identified as the likely cause of agranulocytosis. ANC = 0.2 × 10⁹/L. What is the immediate management?
Analysis: This is carbimazole-induced agranulocytosis. Immediate management: (1) Stop carbimazole immediately — do not restart it or switch to PTU (partial cross-reactivity of agranulocytosis exists). (2) Admit to hospital; reverse barrier nursing. (3) CBC with differential daily until ANC recovers. (4) Broad-spectrum antibiotics if fever persists (empirically cover gram-negative organisms — neutropenic sepsis protocol). (5) Consider granulocyte colony-stimulating factor (G-CSF — filgrastim) to accelerate neutrophil recovery if ANC <0.5 × 10⁹/L with fever/sepsis. (6) Definitive therapy for Graves disease after recovery: either radioiodine or surgery (antithyroid drugs are no longer an option). (7) Patient must be educated never to take carbimazole or PTU again.
CLINICAL PEARL
The three high-yield pharmacological traps in thyroid treatment that appear in every examination and cause real clinical errors: (1) Carbimazole in first-trimester pregnancy — causes aplasia cutis and other embryopathies; use PTU in first trimester, switch to carbimazole in second trimester. (2) Iodine before thionamide in thyroid storm — gives the unblocked gland iodine substrate, potentially worsening the crisis; always give PTU/carbimazole at least 1–2 hours before Lugol's iodine. (3) Starting levothyroxine without cortisol cover in secondary hypothyroidism — accelerates cortisol clearance and precipitates adrenal crisis in a patient whose pituitary cannot increase ACTH; always give hydrocortisone first. These three rules are not abstractions — each is the residue of a case where getting the sequence wrong caused serious harm.