Page 4 of 21
IM13.7-10 | Cancer Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit, document, and present a structured oncological history that captures aetiology, risk factors, duration, and evolution of symptoms
- Perform a systematic general and local physical examination to establish diagnosis, assess tumour extent, lymph node spread, and complications
- Demonstrate breast examination, rectal examination, and cervical examination/Pap smear on a mannequin with correct technique
- Generate a differential diagnosis from presenting symptoms and clinical features, and identify the most likely diagnosis
INSTRUCTIONS
Clinical evaluation is the entry point of all oncological care. A thorough history and examination — when performed systematically — allow the experienced clinician to generate a working diagnosis, stage the tumour locally, and direct investigations efficiently. This skills module guides you through the structured oncological history, the systematic physical examination (general and site-specific), and the practical techniques for breast, rectal, and cervical examinations.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 68 — Approach to the Patient with Cancer (textbook)
- API Textbook of Medicine, 10th ed., Section on Clinical Oncology (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 11 — Clinical Evaluation of the Cancer Patient (textbook)
- NICE Clinical Knowledge Summary: Suspected Cancer — Recognition and Referral (NG12, 2023 update) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are a third-year resident in the general medicine outpatient clinic. Your next patient is Meena, a 52-year-old woman who has come with a 3-month history of altered bowel habit — alternating loose stools and constipation — and a sensation that her bowel is not fully emptying. She looks thin and anaemic. You notice on her face the faint jaundice of hepatic involvement and the pallor of a chronic blood loss anaemia. You have 15 minutes. Where do you start? Do you focus on the bowel? On the weight loss? On the family history? On her medications? The answer is all of the above — but in a systematic, purposeful order that maps the cardinal oncological features: the symptom itself, its risk context, its tempo, its spread, and its impact on the patient's functional status. This module teaches you that structure, so that 15 minutes produces a complete oncological picture rather than a disorganised collection of facts.
WHY THIS MATTERS
NMC competencies IM13.7 to IM13.10 are written at the SH (Skill and Habit) level — meaning you are expected to perform these clinical skills competently, not merely know them in theory. A well-elicited oncological history reduces time to diagnosis, prevents costly over-investigation, identifies patients who need urgent referral under national cancer control guidelines, and establishes the rapport necessary for the difficult conversations that follow a cancer diagnosis. Breast examination, rectal examination, and cervical examination with Pap smear are procedural competencies you will perform throughout your career — in both screening and symptomatic contexts.
RECALL
Activate your prior knowledge. Recall the components of a standard systematic history from your Year 1 clinical skills training: presenting complaint, history of presenting complaint (onset, duration, character, radiation, aggravating and relieving factors, associated symptoms), past medical and surgical history, drug history, family history, social history, and a review of systems. Now overlay oncological thinking: which presenting complaints are red-flag symptoms requiring urgent two-week-wait referral? What aspects of the family history are specifically cancer-relevant (first-degree relatives, bilateral tumours, early age at diagnosis)? What occupational and environmental exposures are carcinogenic? Which performance status score is most commonly used to capture functional capacity in cancer patients? With this scaffold in place, let us build the oncological clinical evaluation.
Eliciting the Oncological History
The oncological history is a targeted elaboration of the standard systematic history, structured to answer four essential clinical questions: What is the presenting syndrome? What is the likely tumour site? What is the extent of spread? What is the patient's capacity to tolerate treatment? Each of these questions maps directly onto a part of the history and examination, ensuring that no clinically critical information is missed.
Provided image
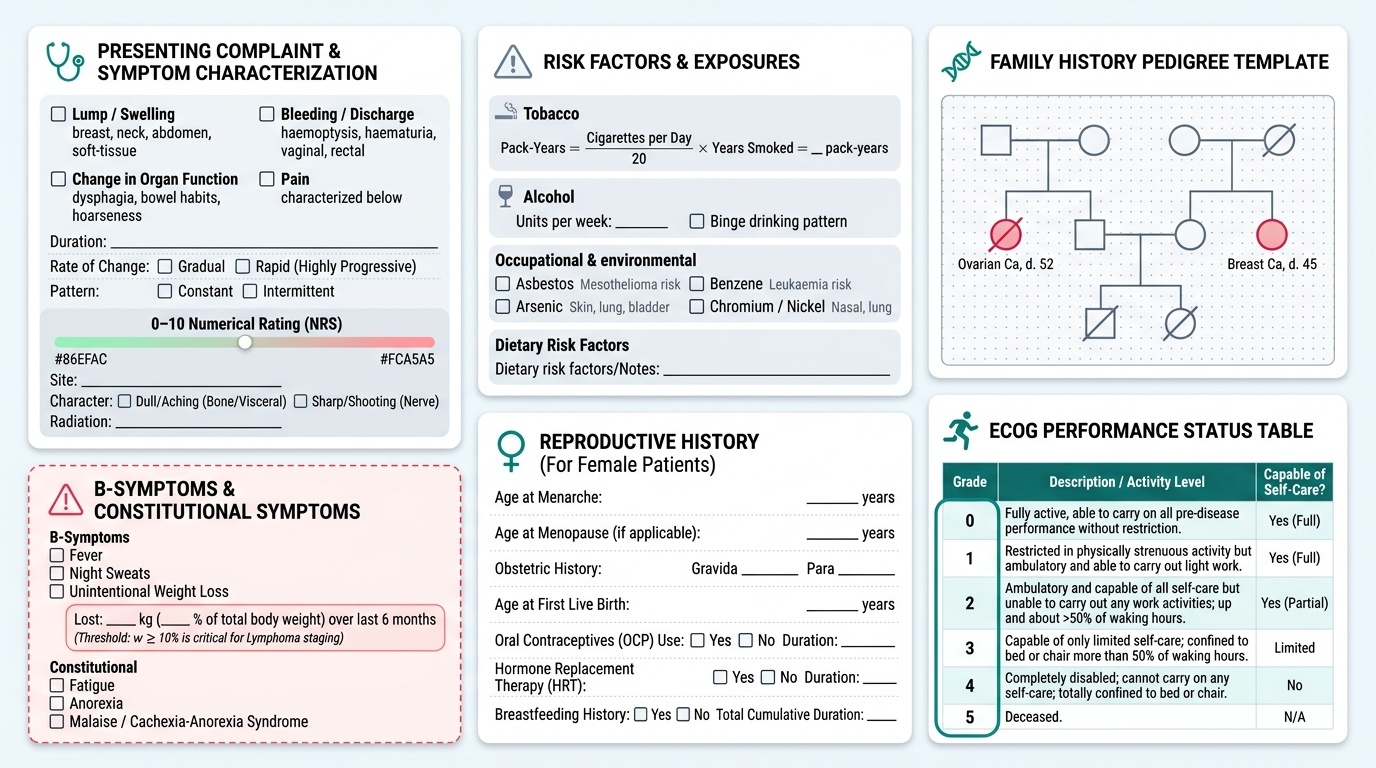
Presenting complaint and history of presenting illness should document the symptom in its full temporal and qualitative detail. For most cancers, the presenting complaint falls into one of four categories: (1) a lump or swelling (breast mass, neck node, abdominal mass, soft-tissue sarcoma); (2) a bleeding or discharge (haemoptysis, rectal bleeding, haematuria, postmenopausal vaginal bleeding, nipple discharge); (3) a change in organ function (dysphagia, change in bowel habit, dysuria, hoarseness, dyspnoea); or (4) constitutional symptoms — the so-called 'B symptoms' (fever, night sweats, unintentional weight loss >10% body weight over 6 months — important in lymphoma staging), or more broadly: weight loss, fatigue, anorexia, and malaise (the classic cancer constitutional syndrome, often termed cachexia-anorexia syndrome). Document the exact duration, rate of change (gradual or rapid? — rapidly progressive disease often suggests haematological malignancy, aggressive lymphoma, or metastatic solid tumour), and whether the symptom is constant or intermittent. Pain is a cardinal symptom: characterise its site, character (dull aching = bone/visceral; sharp shooting = nerve compression), radiation (e.g., pancreatic cancer pain radiates to the back), severity (0–10 Numerical Rating Scale), and aggravating/relieving factors.
Risk factor history systematically covers modifiable and inherited exposures. For tobacco: quantify in pack-years (cigarettes smoked per day ÷ 20 × years smoked; or for bidis/smokeless tobacco, document the equivalent daily quantity and duration). For alcohol: use units per week and note binge drinking patterns. For occupational exposures: ask about asbestos (construction, shipbuilding, insulation — mesothelioma risk), benzene (petroleum, chemicals — leukaemia), arsenic (mining, groundwater in West Bengal and North-East India — skin, lung, bladder cancer), chromium, nickel, vinyl chloride. For dietary history: processed/red meat consumption (colorectal cancer risk), aflatoxin exposure (grain storage practices — hepatocellular carcinoma risk in some regions). For reproductive history in women: age at menarche, parity, age at first full-term pregnancy (nulliparity → higher breast and ovarian cancer risk), breastfeeding history (protective for breast cancer), age at menopause, and use of exogenous hormones (combined OCP — slight breast cancer risk increase; combined HRT — breast and endometrial cancer risk).
Family history must be taken in a structured pedigree format at minimum for first-degree relatives: document each first-degree relative (parents, siblings, children), their age, cancer diagnosis (with site confirmed, not just 'cancer'), and age at diagnosis. Red flags for a hereditary cancer syndrome include: ≥2 first-degree relatives with the same or related cancer, any relative with cancer at an unusually young age (<50 for colorectal cancer, <40 for breast cancer), bilateral or multifocal disease (bilateral breast cancer, bilateral renal cell carcinoma), multiple primary cancers in one individual, and male breast cancer (strongly suggests BRCA2). Document the ethnic background (Ashkenazi Jewish ancestry has a high frequency of BRCA founder mutations; certain South Asian communities have elevated BRCA2 and Lynch syndrome frequencies).
Performance status assessment using the ECOG (Eastern Cooperative Oncology Group) Performance Status scale (0–4) or the equivalent Karnofsky Performance Status (KPS) scale (0–100%) is a mandatory component of the oncological assessment. Performance status predicts treatment tolerance, quality of life, and overall survival, and determines eligibility for clinical trials and chemotherapy regimens:
| ECOG PS | Description | KPS equivalent |
|---|---|---|
| 0 | Fully active, no restrictions | 100% |
| 1 | Restricted in strenuous activity; ambulatory, light work | 80–90% |
| 2 | Ambulatory, capable of self-care; up >50% of waking hours | 60–70% |
| 3 | Limited self-care; confined to bed/chair >50% of waking hours | 40–50% |
| 4 | Completely disabled; cannot carry on self-care | 10–30% |
ECOG PS ≥2 is often the threshold at which standard cytotoxic chemotherapy becomes more harmful than beneficial; PS 3–4 patients are typically managed with best supportive/palliative care.
General and Systemic Physical Examination in Cancer
Physical examination in oncology serves two linked purposes: first, to characterise the primary lesion (site, size, surface, consistency, fixity, transillumination, pulsatility); second, to detect evidence of regional spread (lymphadenopathy, direct extension) and distant metastasis (hepatomegaly, ascites, pleural effusion, bony tenderness, neurological deficits). Examination must be both general and site-specific — the general examination often reveals distant spread before the patient reports it.
The general examination should systematically assess: (1) nutritional and functional status — document weight and BMI; cachexia is clinically apparent as temporal wasting, loss of muscle mass in the thenar eminences and interossei, prominent ribs and clavicles; (2) pallor — mucosal pallor in the conjunctivae, tongue, and nail beds indicates anaemia, which in cancer may result from bone marrow infiltration (leucoerythroblastic film), bleeding, haemolysis, or anaemia of chronic disease; (3) jaundice — scleral icterus visible at bilirubin >35 µmol/L; in cancer, this indicates biliary obstruction (pancreatic head cancer, cholangiocarcinoma), hepatic metastasis, or haemolysis; (4) lymphadenopathy — examine all nodal chains systematically: submental, submandibular, anterior and posterior cervical, supraclavicular (Virchow's node on the left = Troisier sign — upper abdominal primary; scalene node on right = right lung/mediastinal primary), axillary (anterior, posterior, central, and apical groups), epitrochlear, inguinal (horizontal and vertical groups), and popliteal nodes; document size in centimetres, consistency (soft/rubbery/hard/fixed/matted), tenderness (benign reactive nodes are tender; metastatic and lymphomatous nodes are typically non-tender), and mobility; (5) clubbing — present in lung cancer (especially squamous cell), mesothelioma, hepatocellular carcinoma; (6) skin — spider naevi, palmar erythema, gynaecomastia (liver failure from hepatic metastasis or HCC); paraneoplastic dermatoses: acanthosis nigricans (gastric adenocarcinoma), dermatomyositis (lung, ovarian, colorectal), Leser-Trélat sign (sudden eruption of multiple seborrhoeic keratoses — gastrointestinal cancer).
The abdominal examination in suspected gastrointestinal, hepatic, or pelvic malignancy requires particularly systematic technique. Inspection first: asymmetry, visible peristalsis, dilated veins (caput medusae in portal hypertension from liver metastasis), umbilical nodule (Sister Mary Joseph nodule — peritoneal spread from intra-abdominal cancer). Palpation: begin in all four quadrants before moving to the epigastrium; assess the liver (size, consistency — smooth in hepatitis/normal, irregular/nodular in metastasis or HCC, tender in acute congestion), spleen (cross the abdomen from right iliac fossa — splenomegaly in lymphoma, CML, myelofibrosis), and any discrete masses (note position relative to bony landmarks, size, shape, surface, consistency, mobility with respiration). Percussion: dullness in flanks shifting with position = ascites (malignant ascites from peritoneal carcinomatosis). Auscultation: succussion splash (pyloric obstruction from gastric cancer).
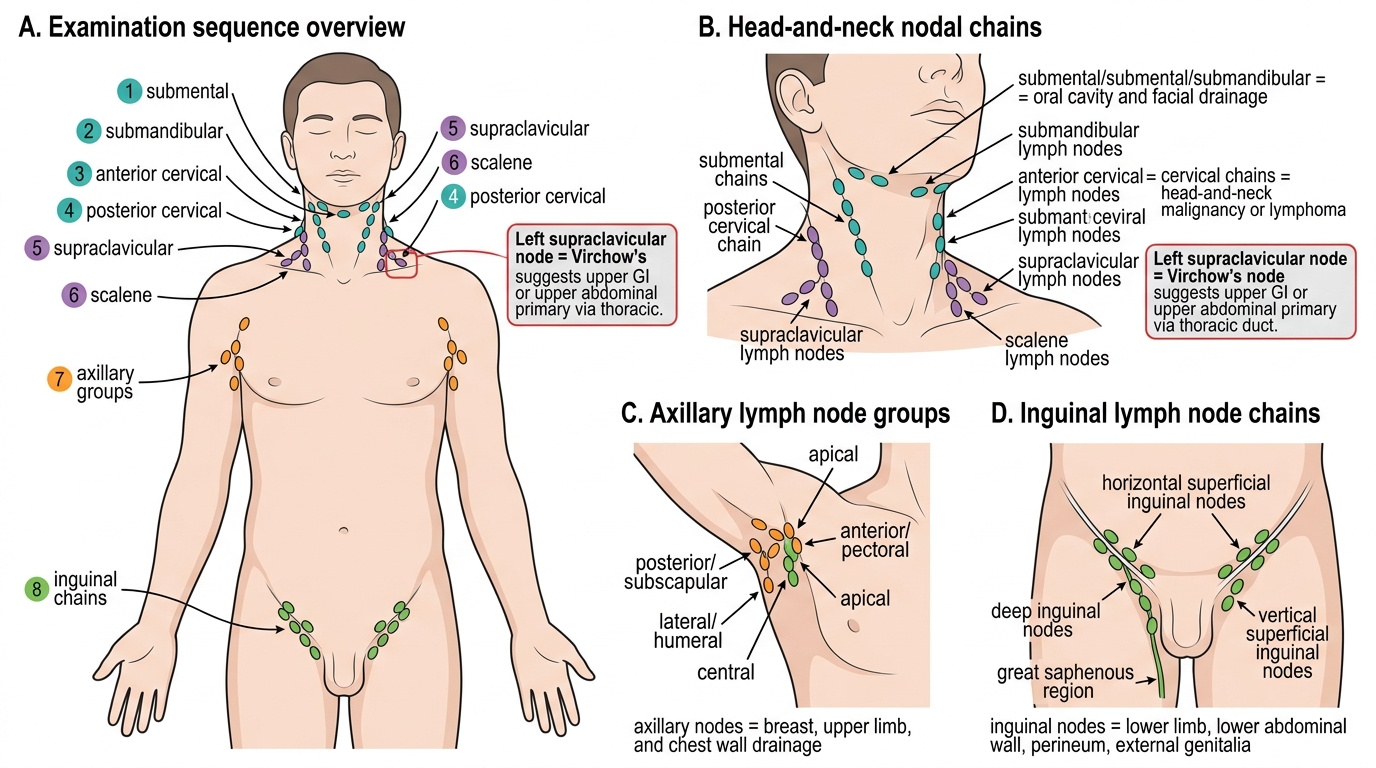
Clinical Lymph Node Examination Sequence
SELF-CHECK
During a general physical examination, you palpate a firm, non-tender, 2 cm lymph node in the left supraclavicular fossa of a 60-year-old man with dysphagia and weight loss. This clinical finding is known as Virchow's node. What is the most likely source of the primary malignancy?
A. Lymphoma originating in the mediastinum
B. Left axillary breast cancer
C. Upper gastrointestinal (oesophageal or gastric) cancer
D. Lung cancer in the left upper lobe
Reveal Answer
Answer: C. Upper gastrointestinal (oesophageal or gastric) cancer
Virchow's node (Troisier sign) is a left supraclavicular lymph node enlarged by metastatic spread via the thoracic duct, which drains into the left subclavian vein. The thoracic duct collects lymph from the entire abdomen; therefore, this node most commonly signals an upper gastrointestinal primary — most classically gastric cancer, followed by oesophageal, pancreatic, and other upper abdominal malignancies. In this man, dysphagia and weight loss with a left supraclavicular node makes oesophageal or gastric cancer the priority diagnosis. Mediastinal lymphoma tends to present with bilateral neck nodes and a mediastinal mass, not an isolated Virchow's node.
Breast Examination Technique
Breast examination is a core procedural skill, assessed in the MBBS practical examination and performed throughout your career in both symptomatic and screening contexts. The NMC competency IM13.9 requires you to demonstrate the correct technique on a mannequin. The procedure has three stages: inspection, palpation, and lymph node assessment. Ensure privacy, chaperone presence, and verbal consent before beginning.
Inspection is performed with the patient sitting upright in three positions: (1) arms by sides (resting), (2) arms raised above the head (stretches Cooper's ligaments — skin tethering and nipple deviation become apparent), and (3) hands pressed firmly on hips (contracts pectoralis major — fixation to the muscle revealed). Look systematically for: (a) asymmetry in size and shape — mild natural asymmetry is common; new asymmetry is significant; (b) skin changes — peau d'orange (orange-peel dimpling from lymphatic oedema — classic in inflammatory breast cancer or skin involvement by tumour), skin tethering or dimpling (Cooper's ligament involvement by underlying tumour), skin nodules or ulceration; (c) nipple changes — retraction, inversion (recent onset is significant; longstanding inversion may be normal), deviation, eczematoid change (Paget's disease — eczematous rash of the nipple–areola complex indicative of underlying ductal carcinoma in situ or invasive cancer); (d) dilated subcutaneous veins over one breast (increased vascularity from a tumour).
Palpation is performed with the patient supine, ipsilateral arm raised above the head (flattens breast tissue against the chest wall). Use the flat of the fingers (pads of index, middle, and ring fingers), not the fingertips. Palpate all four quadrants plus the axillary tail (tail of Spence) in a systematic pattern — vertical strip, radial, or concentric circle technique — to ensure no segment is missed. When a lump is detected, characterise: site (use clock face and distance from nipple: e.g., 'upper outer quadrant, 3 cm from nipple at 2 o'clock'), size (in centimetres), shape (regular vs. irregular), surface (smooth vs. lobulated vs. irregular), consistency (soft/firm/hard — malignant tumours are typically hard, cystic lumps are fluctuant), edges (well-defined vs. ill-defined), mobility (freely mobile vs. fixed to overlying skin or deep fascia/pectoralis muscle — fixation implies advanced local disease), and tenderness (cyclical tenderness = fibrocystic change; non-tender hard mass = malignancy until proven otherwise). Examine the nipple for discharge — note colour (bloodstained discharge from a single duct = intraductal papilloma or carcinoma; milky bilateral = prolactinoma; green-black multiduct = fibrocystic change).
Lymph node assessment: with the patient sitting, examine the axilla with the examiner supporting the patient's ipsilateral arm to relax the pectoralis major. Palpate the anterior group (pectoralis minor), posterior group (subscapularis), central group, medial group (against chest wall), and apical group (below clavicle). Then examine the supraclavicular fossa bilaterally and the infraclavicular fossa. Document number, size, and consistency of any palpable nodes.
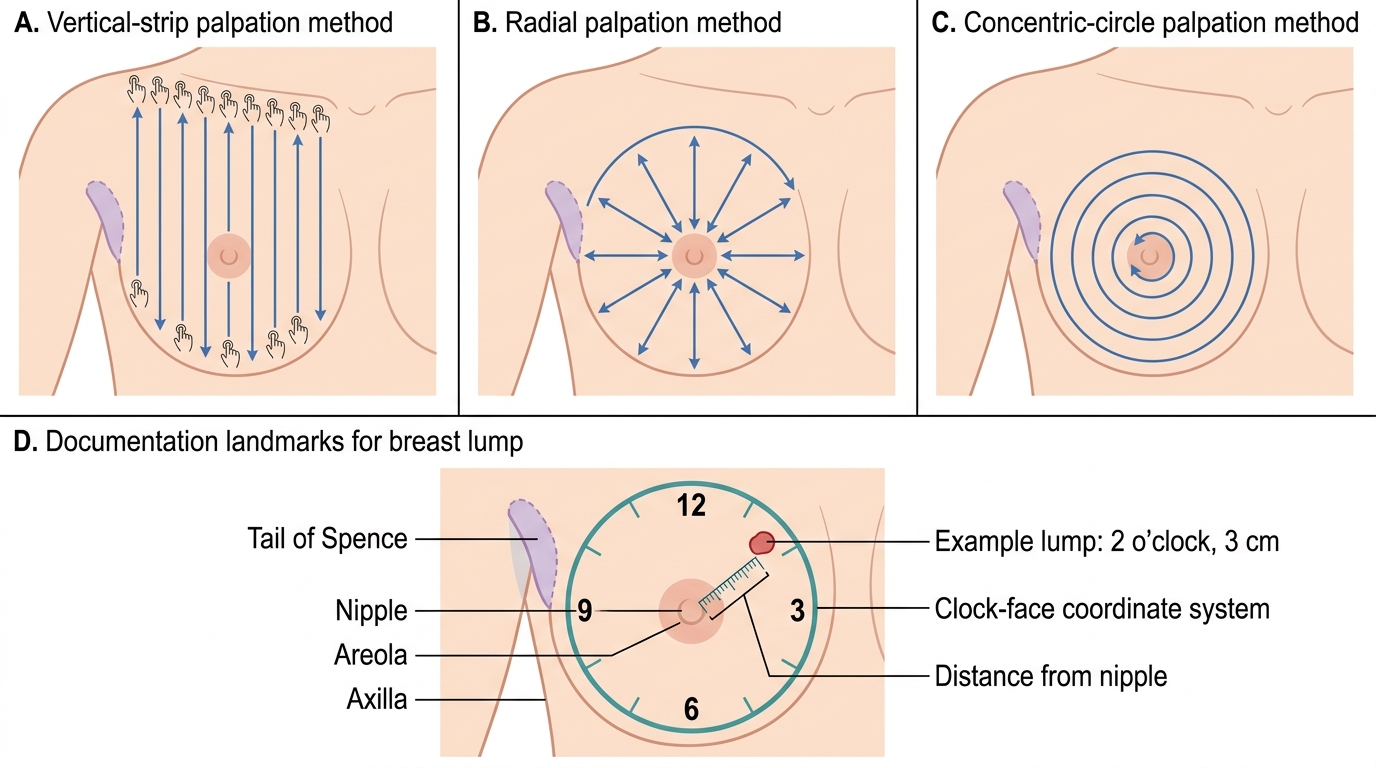
Breast Examination Palpation Patterns and Lump Documentation