Page 2 of 21
IM13.{1-4,15} | Oncology Foundations — SDL Guide (Part 2)
Natural History, Presentation, and Complications of Common Cancers
The natural history of a cancer describes its biological course from inception to advanced disease — the sequence of local growth, regional lymph node spread, haematogenous metastasis, and ultimately systemic failure. Understanding this sequence clarifies why early detection improves outcomes, why certain investigations are ordered (local vs. distant staging), and why complications occur when tumours invade or compress adjacent structures.
Most carcinomas follow a predictable progression: (1) dysplasia or carcinoma in situ (CIS) — pre-invasive proliferation within the epithelial basement membrane; (2) invasive carcinoma — penetration through the basement membrane with access to lymphatics and blood vessels; (3) regional lymph node metastasis — the first and most important spread route for most solid tumours, determining TNM stage; (4) haematogenous metastasis — dissemination through blood to target organs. The organs most commonly involved in haematogenous metastasis follow patterns determined by circulatory drainage and organ-specific factors: the lung (systemic venous drainage), liver (portal venous drainage from gastrointestinal primary tumours), bone (axial skeleton, pelvis, femur — via Batson's venous plexus), brain, and adrenal glands are the most frequent haematogenous metastatic sites. The mnemonic 'Lung, Liver, Lymph node, Bone, Brain' covers >80% of clinically significant metastatic sites.
Oral cavity and oropharyngeal cancer typically presents as a non-healing ulcer, exophytic mass, or leukoplakia/erythroplakia of the buccal mucosa, tongue, or floor of mouth. The chronology from precancerous lesion to invasive cancer spans months to years; the natural history without treatment is relentless local invasion and cervical lymph node metastasis (N1–N3), with distant metastasis occurring late.
Lung cancer — predominantly adenocarcinoma and squamous cell carcinoma in smokers — typically presents late because the lung parenchyma has no pain receptors. Common presenting features include persistent cough (>3 weeks), haemoptysis, dyspnoea, weight loss, and chest pain. Locally advanced disease causes superior vena cava (SVC) obstruction (SVC syndrome: facial and neck swelling, arm oedema, dilated collateral veins, headache — a recognised oncological emergency), Horner syndrome (Pancoast tumour: apical lung tumour invading the sympathetic chain), and hoarseness (left recurrent laryngeal nerve compression). The natural history is rapid: median survival without treatment for metastatic non-small cell lung cancer (NSCLC) is approximately 4–5 months.
Breast cancer natural history spans a longer pre-clinical phase: ductal carcinoma in situ (DCIS) may remain in situ for years before progressing to invasive ductal carcinoma. Spread follows predictable lymphatic routes — axillary nodes first (most important prognostic factor), then internal mammary and supraclavicular nodes. Haematogenous metastasis preferentially involves bone (osteolytic in ER-positive, mixed in HER2-positive breast cancer), lung, liver, and brain.
Gastric cancer has a long silent phase; most Indian patients present with advanced disease (T3–T4, N+) due to delayed health-seeking and lack of screening. Virchow node (left supraclavicular fossa lymphadenopathy) and Sister Mary Joseph nodule (periumbilical metastatic nodule) are classic clinical signs of disseminated upper gastrointestinal malignancy.
Cancer complications arise from three mechanisms: (1) local mass effect — SVC obstruction, cord compression (spinal metastasis), obstructive jaundice (hepatic or biliary metastasis), ureteric obstruction; (2) systemic metabolic effects — cachexia (cytokine-mediated wasting), anaemia, venous thromboembolism (Trousseau syndrome — migratory thrombophlebitis, particularly in mucin-secreting adenocarcinomas of the pancreas and gastrointestinal tract), hypercalcaemia, hyponatraemia (SIADH in SCLC); (3) paraneoplastic syndromes — remote immunological or humoral effects not caused by direct tumour invasion (detailed in a later section).
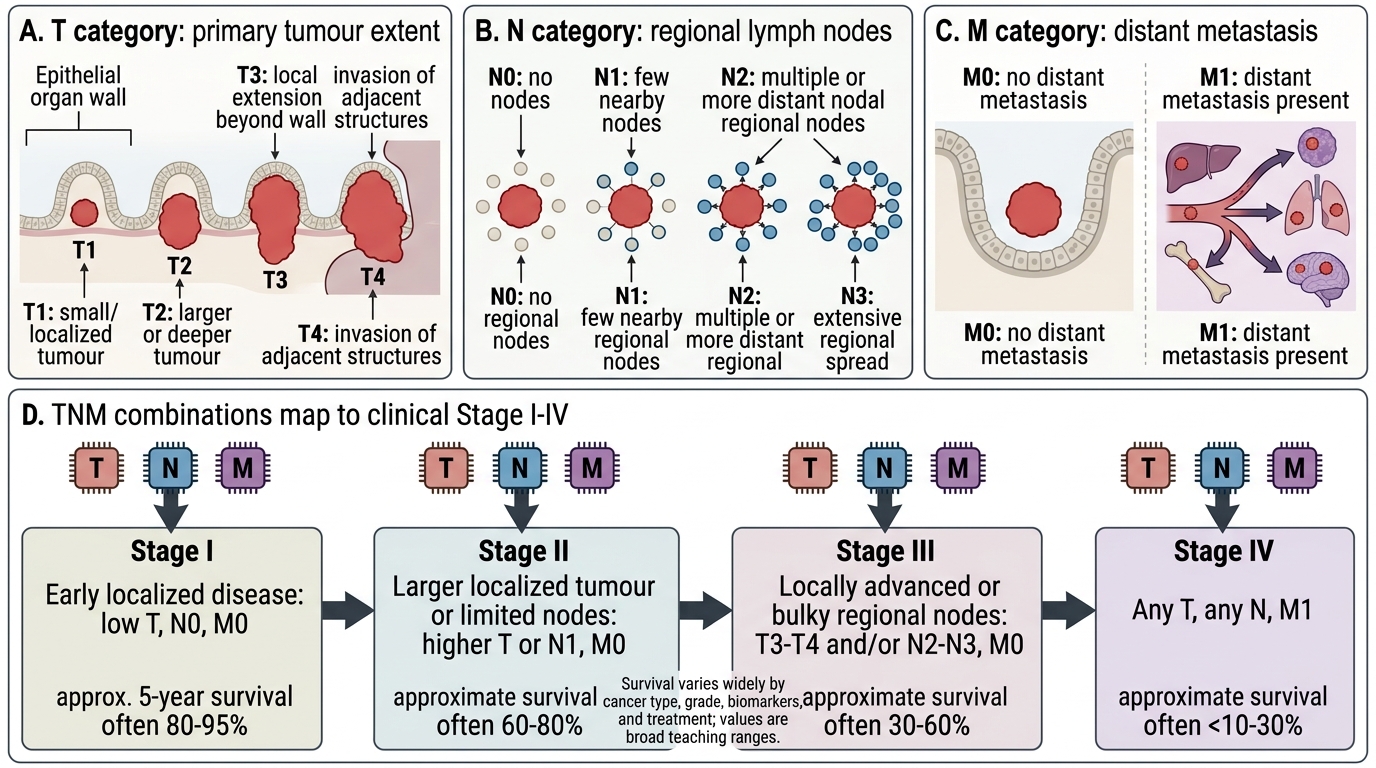
TNM Staging Framework and Clinical Stage Mapping
SELF-CHECK
A 58-year-old man with known lung cancer develops progressive facial swelling, dilated veins over the anterior chest wall, and severe headache worse on bending forward. His arms are oedematous. Which oncological emergency does this presentation represent?
A. Hypercalcaemia of malignancy
B. Superior vena cava (SVC) obstruction syndrome
C. Tumour lysis syndrome
D. Spinal cord compression
Reveal Answer
Answer: B. Superior vena cava (SVC) obstruction syndrome
This is the classic presentation of SVC obstruction: facial and neck oedema, arm swelling, dilated chest wall collateral veins (venous engorgement bypassing the obstructed SVC), and positional headache. The most common cause in India is lung cancer (right-sided hilar or mediastinal mass compressing the SVC). Management includes elevation of the head, corticosteroids to reduce oedema, and urgent oncological intervention (radiotherapy or endovascular stenting). Hypercalcaemia causes confusion, polyuria, and constipation; tumour lysis causes hyperuricaemia and acute kidney injury; cord compression causes back pain and lower limb weakness.
Cancer Prevention and Screening
Cancer prevention operates at three levels — primary (preventing cancer from developing), secondary (detecting cancer or its precursors early through screening), and tertiary (preventing complications and recurrence in diagnosed cases). For final-year clinical students in India, the most operationally relevant competency is knowing which screening tests exist, their evidence base, target populations, and limitations — as defined by NMC IM13.15.
Provided image
Primary prevention strategies target modifiable risk factors. Tobacco cessation is the highest-yield single intervention: stopping smoking at any age reduces lung cancer risk substantially, and oral cancer risk decreases within 5 years of stopping smokeless tobacco. HPV vaccination (bivalent Cervarix or quadrivalent Gardasil — administered in the 9–14 year age window before sexual debut) prevents approximately 70% (bivalent) to 90% (nonavalent) of cervical cancers. India's national immunisation programme included HPV vaccine for adolescent girls in a phased rollout from 2023. Hepatitis B vaccination is already part of the Universal Immunisation Programme; its full impact on HCC incidence will be seen over the next two decades. H. pylori test-and-treat in high-risk populations (family history of gastric cancer) reduces gastric cancer risk.
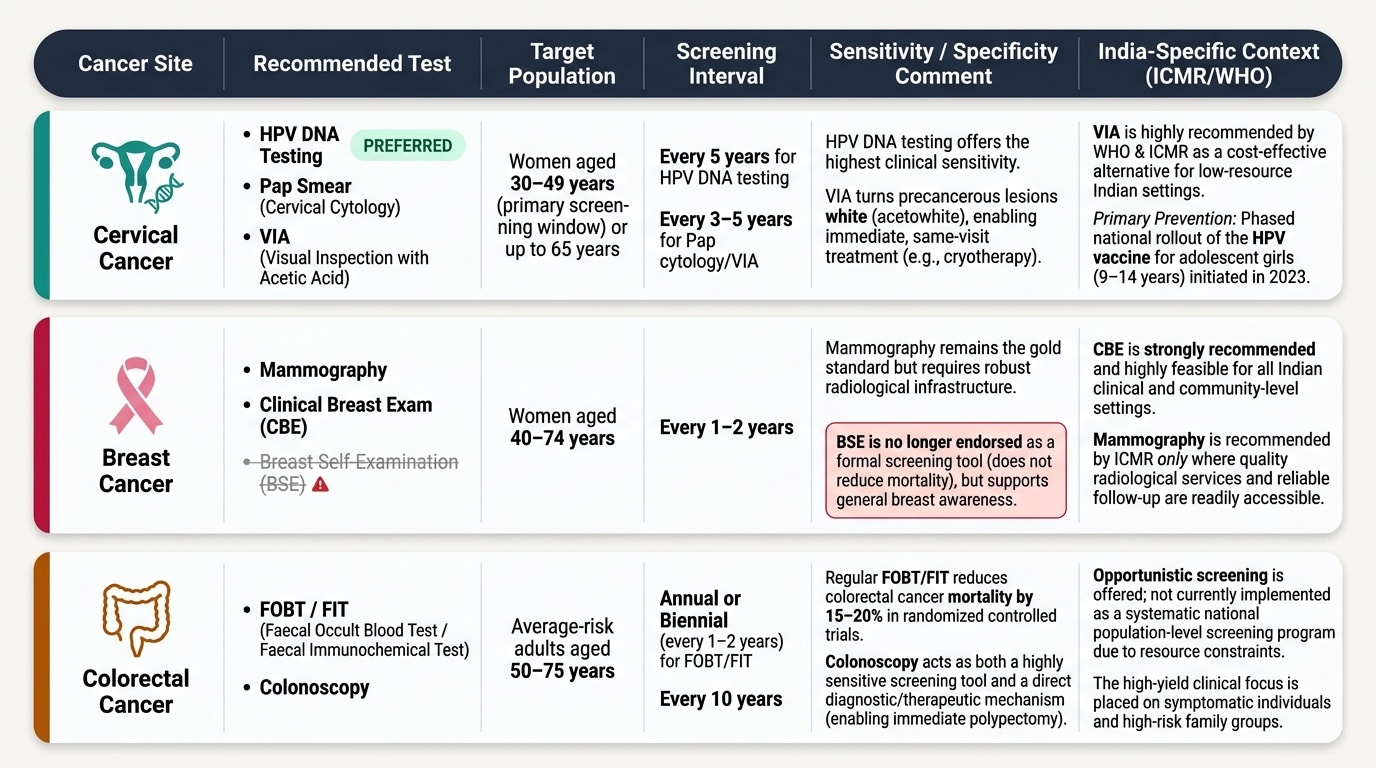
Secondary prevention (screening) aims to detect cancer at a stage where curative treatment is feasible. Key screening programmes and their evidence:
- Cervical cancer: Pap smear (cervical cytology) and visual inspection with acetic acid (VIA) — the latter is recommended by WHO and ICMR as a cost-effective alternative for low-resource Indian settings. VIA turns precancerous lesions white and allows same-visit treatment (cryotherapy). HPV DNA testing (high-risk types) is now endorsed as the preferred cervical cancer screening test and can be done every 5 years.
- Breast cancer: clinical breast examination (CBE) — feasible in all Indian settings; mammography — recommended every 1–2 years for women aged 40–74 in those with access to adequate radiological services (ICMR guidelines). Breast self-examination (BSE) is no longer endorsed as a formal screening tool but supports health-seeking behaviour.
- Colorectal cancer: faecal occult blood test (FOBT/FIT) — annual or biennial testing reduces CRC mortality by 15–20% in randomised trials; colonoscopy is the gold-standard diagnostic tool for positive FOBT and for surveillance in Lynch syndrome and FAP kindreds.
- Oral cancer: visual inspection for pre-malignant lesions (leukoplakia, erythroplakia, OSMF) by primary health workers — particularly important given India's tobacco burden; now included in ASHA worker training under national oral health programmes.
- Prostate cancer: prostate-specific antigen (PSA) testing is controversial — it reduces prostate cancer mortality but leads to significant over-diagnosis and over-treatment of indolent cancers. ICMR does not currently recommend population-level PSA screening; it is offered to informed men aged 50+ or 40+ with family history after shared decision-making.
- Lung cancer: low-dose CT (LDCT) chest — the NLST trial showed 20% mortality reduction in high-risk smokers (≥30 pack-years, ages 55–74); recommended in eligible high-risk smokers in the USA; not yet part of India's national programme.
Tumour markers in screening and monitoring: Most tumour markers lack sufficient sensitivity and specificity for population-level screening but have utility in monitoring treatment response and detecting recurrence. Key markers: AFP (hepatocellular carcinoma, testicular non-seminomatous germ cell tumours), β-hCG (choriocarcinoma, testicular cancer), PSA (prostate cancer), CA 125 (epithelial ovarian cancer — monitoring), CEA (colorectal cancer — monitoring, not screening), CA 19-9 (pancreatic cancer — monitoring). The exception is AFP plus ultrasound surveillance every 6 months in cirrhotic patients — this is a guideline-endorsed secondary prevention strategy with evidence for detecting HCC at resectable stage.
SELF-CHECK
A 38-year-old woman in a rural primary health centre presents for a routine checkup. She is sexually active and has never had cervical cancer screening. Which is the most appropriate and feasible first-line cervical cancer screening test recommended for low-resource Indian settings by WHO and ICMR?
A. Liquid-based cytology (LBC) Pap smear
B. Colposcopy with directed biopsy
C. Visual inspection with acetic acid (VIA)
D. HPV serology (IgG anti-HPV antibodies)
Reveal Answer
Answer: C. Visual inspection with acetic acid (VIA)
Visual inspection with acetic acid (VIA) is the WHO and ICMR-endorsed first-line cervical cancer screening strategy for low-resource settings in India. VIA is inexpensive, requires no laboratory infrastructure, gives immediate results, and allows same-visit treatment of positive lesions (screen-and-treat). Liquid-based cytology and colposcopy require specialised laboratory processing or equipment unavailable in rural PHCs. HPV serology does not test for current infection or pre-cancerous lesions and has no role in screening. HPV DNA testing is being scaled up but VIA remains the pragmatic cornerstone of India's cervical cancer screening programme.
Self-Assessment: Integrating Oncology Foundations
Having covered epidemiology, genetic mechanisms, infection-related cancers, natural history, and prevention, you are now asked to synthesise these foundations through brief integrative scenarios. These exercises reflect the clinical reasoning expected at the NMC KH (Knowledge and Understanding applied to clinical scenarios) level for IM13.1–13.4 and IM13.15.
Scenario A: A 40-year-old woman is found to have breast cancer. Her mother and two maternal aunts had breast or ovarian cancer. She asks whether her daughters should be tested. What is the key gene to be discussed, and what is the appropriate counselling approach?
Analysis: The family history strongly suggests a BRCA1 or BRCA2 germline mutation (or other high-penetrance gene such as PALB2). The proband should be offered genetic counselling and germline testing. If a pathogenic variant is found, cascade testing is offered to first-degree relatives (daughters included). Daughters aged ≥18 can be tested and counselled about risk-reducing options (enhanced surveillance, chemoprevention with tamoxifen, or risk-reducing salpingo-oophorectomy/bilateral mastectomy after childbearing is complete). Psychological support is an integral part of this process.
Scenario B: A 55-year-old man who has had chronic hepatitis B for 20 years and established liver cirrhosis attends follow-up. His AFP is 65 ng/mL (previously 15 ng/mL) and abdominal ultrasound shows a new 2 cm arterialised hepatic nodule. What is the most likely diagnosis and what additional imaging is needed?
Analysis: The combination of cirrhosis, rising AFP, and a new arterialised lesion on ultrasound is highly characteristic of hepatocellular carcinoma (HCC). In cirrhotic patients, the AASLD/EASL guidelines allow diagnosis of HCC without biopsy for nodules ≥1 cm that show arterial enhancement and venous washout on dynamic contrast-enhanced MRI or CT (the hallmark vascular pattern of HCC). The next step is multiphase CT or MRI liver; if the typical vascular pattern is present, HCC can be diagnosed and staged without biopsy. His aetiology is HBV — a reminder that HBV vaccination and antiviral therapy (tenofovir or entecavir) reduce HCC incidence even in those with established cirrhosis.
Scenario C: A 32-year-old woman with cervical cancer is asked by her family whether her younger siblings (aged 14–20) should receive HPV vaccination. What is your advice?
Analysis: Yes — absolutely. Siblings aged 9–14 are in the optimal vaccination window before sexual exposure. For those aged 15–20, vaccination is still beneficial but requires 3 doses (versus 2 doses for those under 15). HPV vaccination does not treat existing infection but prevents future high-risk HPV acquisition. Given the proband's history of cervical cancer (likely HPV-attributable), counselling younger family members about vaccination and screening is a direct, preventable public health intervention.
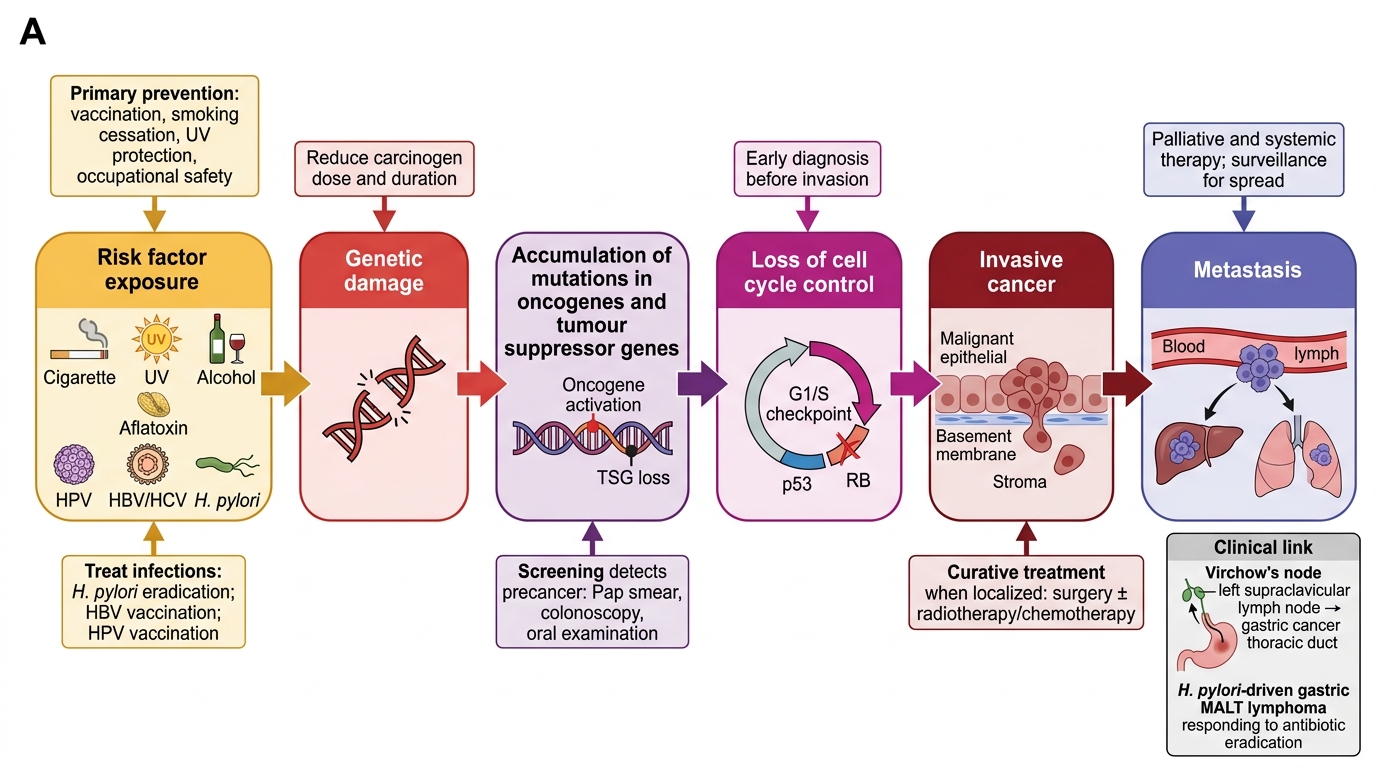
Carcinogen Exposure to Metastatic Cancer: Prevention Targets
CLINICAL PEARL
Two high-yield clinical pearls for oncology foundations:
First, Virchow's node (a firm, non-tender left supraclavicular lymph node, also called Troisier sign) is the clinical hallmark of disseminated upper abdominal malignancy — most commonly gastric cancer — spreading via the thoracic duct to the left subclavian venous junction. Finding this node on examination should trigger urgent investigation for a primary intraabdominal or thoracic tumour, not a lymphoma workup alone.
Second, regarding infection and cancer: H. pylori eradication therapy cures low-grade gastric MALT lymphoma in approximately 75–80% of early-stage (localised, t(11;18)-negative) cases — making it one of the very few cancers whose initial management is an antibiotic regimen (triple therapy: PPI + amoxicillin + clarithromycin, or quadruple regimen in clarithromycin-resistant areas) rather than chemotherapy or radiotherapy. This dramatic biological response is possible because gastric MALT lymphoma is antigen-driven — the B-cell clone is maintained by chronic H. pylori stimulation, and eliminating the antigen allows the immune system to eliminate the lymphoma. Students frequently forget this and jump to chemotherapy; always test for H. pylori first in gastric MALT lymphoma.