Page 9 of 15
IM14.11-14 | Obesity Counselling and Treatment — SDL Guide (Part 2)
Pharmacotherapy for Obesity: Indications, Agents, and Side Effects
Pharmacotherapy for obesity is indicated when lifestyle modification alone, sustained for at least 3–6 months with adequate support, has not achieved clinically meaningful weight loss (≥5% of total body weight), and the patient's BMI meets the pharmacotherapy threshold. Using Asian-Indian cut-offs, pharmacotherapy is appropriate when BMI ≥ 27.5 kg/m² with at least one obesity-related comorbidity (T2DM, hypertension, dyslipidaemia, OSA, NAFLD), or BMI ≥ 32.5 kg/m² regardless of comorbidities. It is critical to emphasise to students that pharmacotherapy is always an adjunct to — never a replacement for — lifestyle modification; it must be combined with a structured dietary and physical activity programme, and its efficacy depends on this combined approach.
Provided image
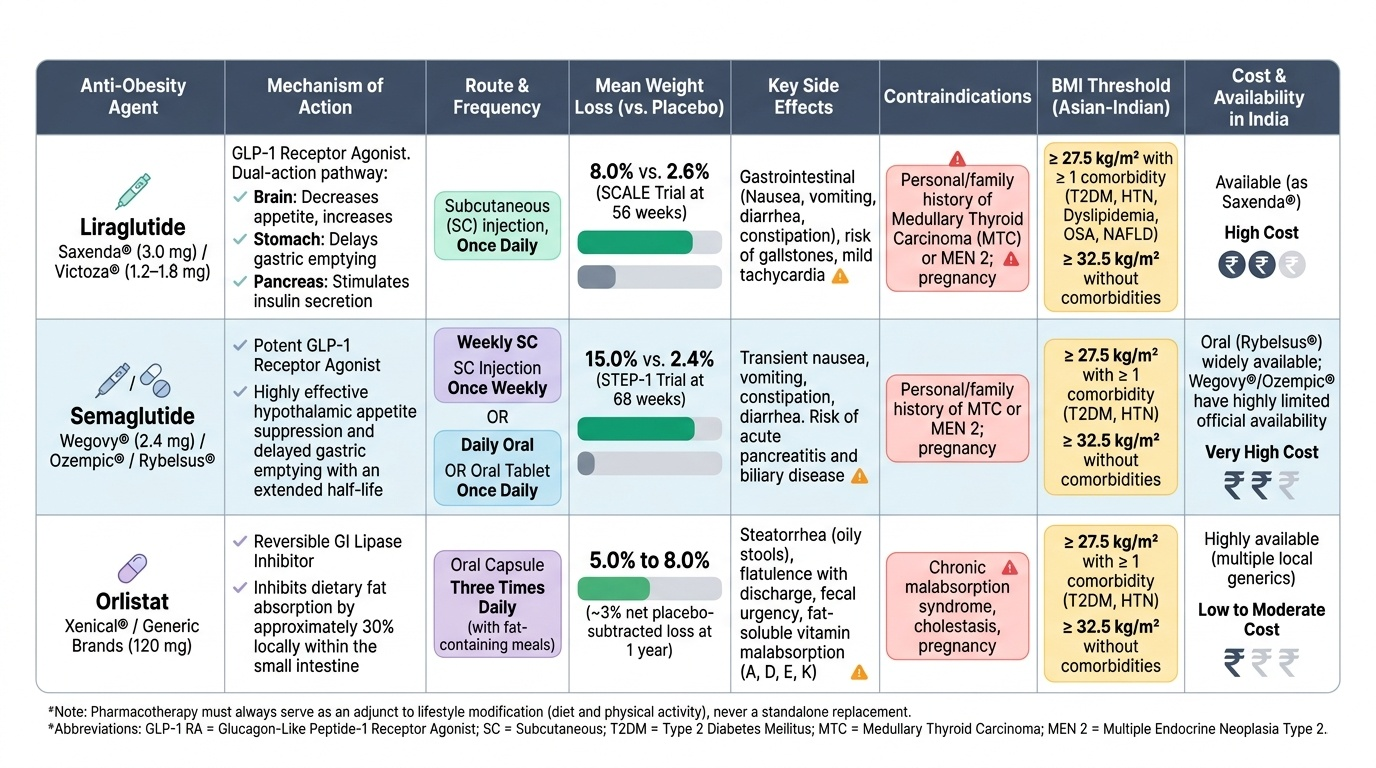
GLP-1 receptor agonists (GLP-1 RAs): the preferred anti-obesity pharmacotherapy in India
Glucagon-like peptide-1 (GLP-1) is an incretin hormone secreted by intestinal L-cells in response to food intake. It acts on GLP-1 receptors in the pancreas (stimulating insulin secretion and suppressing glucagon), the brain (hypothalamus — reducing appetite and increasing satiety), and the gastrointestinal tract (slowing gastric emptying — increasing time-to-next-hunger). This multi-site action makes GLP-1 RAs uniquely effective for both glycaemic control and weight reduction.
Liraglutide (Saxenda® at 3.0 mg/day for obesity; Victoza® at 1.2–1.8 mg/day for T2DM): subcutaneous injection, once daily. The pivotal SCALE trial demonstrated 8% mean weight loss vs 2.6% with placebo at 56 weeks. Approved for obesity management (BMI ≥30, or ≥27 with comorbidities — using Western thresholds; apply Asian-Indian thresholds in practice). Additional cardiovascular benefit demonstrated in the LEADER trial (liraglutide 1.8 mg reduced MACE in T2DM patients).
Semaglutide (Ozempic® 0.5–2 mg weekly for T2DM; Wegovy® 2.4 mg weekly for obesity): subcutaneous injection, once weekly. Substantially greater weight loss than liraglutide: the STEP-1 trial (semaglutide 2.4 mg for obesity without diabetes) demonstrated 15% mean weight loss at 68 weeks vs 2.4% for placebo — the greatest weight loss achieved by any pharmacological agent approved to date. SUSTAIN-6 and SELECT trials demonstrated cardiovascular benefit. An oral semaglutide formulation (Rybelsus®, 3–14 mg daily) is approved for T2DM and is under study for obesity.
Side effects of GLP-1 RAs: predominantly gastrointestinal — nausea (most common, 30–40%, typically transient during dose escalation), vomiting, diarrhoea, constipation, dyspepsia. These are managed by slow dose titration (starting at 0.6 mg/day for liraglutide and escalating monthly). Contraindicated in personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN2), as GLP-1 receptors are expressed on thyroid C-cells; rodent studies showed C-cell hyperplasia (human relevance unclear, but contraindication is maintained). Pancreatitis has been reported; use with caution in patients with prior pancreatitis.
Orlistat (Xenical® 120 mg three times daily with meals):
Orlistat is a pancreatic and gastric lipase inhibitor — it prevents the digestion and absorption of approximately 30% of dietary fat. This produces both caloric deficit (unabsorbed fat = unabsorbed calories) and modest weight loss: approximately 2.5–3.5 kg more than placebo in meta-analyses at 12 months. It is the only anti-obesity drug approved for long-term use in adolescents (≥12 years) as well as adults. Mechanism does not involve any central nervous system effects, which is an advantage in patients with psychiatric comorbidities.
Side effects of orlistat: entirely gastrointestinal and related to unabsorbed fat passing through the colon — steatorrhoea (oily, loose stools), faecal urgency, faecal incontinence (particularly if a high-fat meal is consumed), and oily spotting on underwear. These side effects are predictably worse when dietary fat intake is high — the GI side effects serve as an inadvertent 'negative reinforcer' for high-fat eating. Important: orlistat impairs absorption of fat-soluble vitamins (A, D, E, K) — supplement multivitamins containing fat-soluble vitamins taken at least 2 hours apart from the orlistat dose. Also impairs absorption of some drugs (levothyroxine, anticoagulants, antiepileptics — dose monitoring required).
Other pharmacotherapy (for reference):
- Naltrexone/bupropion (Contrave®): combined opioid antagonist/dopamine-norepinephrine reuptake inhibitor; acts on hypothalamic reward circuits to reduce cravings; approved in several countries; may increase blood pressure, not approved in India.
- Phentermine/topiramate (Qsymia®): sympathomimetic amine + anticonvulsant; significant weight loss but cardiovascular concerns (palpitations, hypertension) and teratogenicity (topiramate is Category X in pregnancy).
Pharmacotherapy decision-making:
- First-line choice: if the patient has T2DM + obesity — GLP-1 RA (addresses both conditions, adds cardiovascular benefit, most evidence in Indian populations)
- If no diabetes and cost is a barrier: orlistat (generic versions available, cheaper)
- If patient has significant comorbidities limiting activity and early large weight loss is a priority: semaglutide (greatest weight loss)
- All pharmacotherapy should be stopped if <5% weight loss achieved after 3 months at optimal dose — non-response should trigger reassessment of secondary causes, dietary adherence, and bariatric surgery candidacy
SELF-CHECK
A 52-year-old man with BMI 36 kg/m² (obese by Asian-Indian criteria), type 2 diabetes on metformin, and hypertension has been on a structured lifestyle programme for 5 months with only 2% weight loss. He asks about medication options. He has no personal or family history of thyroid cancer. Which pharmacotherapy is most appropriate as first-line addition?
A. Orlistat 120 mg with each meal, as it has the largest evidence base and no cardiovascular concerns
B. A GLP-1 receptor agonist (liraglutide or semaglutide), as it addresses both obesity and diabetes with additional cardiovascular benefit
C. Naltrexone/bupropion combination, as it acts centrally on reward circuits to reduce cravings
D. No pharmacotherapy — lifestyle modification should continue for at least another 6 months before adding medication
Reveal Answer
Answer: B. A GLP-1 receptor agonist (liraglutide or semaglutide), as it addresses both obesity and diabetes with additional cardiovascular benefit
In a patient with T2DM + obesity who has not achieved adequate weight loss with lifestyle modification (3–6 months is adequate trial), GLP-1 receptor agonists are the evidence-based first-line pharmacotherapy. They address both glycaemia and weight, with proven cardiovascular benefit in high-risk patients (LEADER, SUSTAIN-6, SELECT trials). GLP-1 RAs also have the largest absolute weight loss data (semaglutide 2.4 mg: ~15% body weight). Orlistat has more modest weight loss (~2.5–3.5 kg over placebo) and no glycaemic benefit. Naltrexone/bupropion is not approved in India and has blood pressure concerns. The patient has already had 5 months of lifestyle modification — pharmacotherapy threshold is met (BMI ≥27.5 with comorbidities, and >3 months of lifestyle programme). There is no rationale for further delay.
Bariatric Surgery: Indications, Procedures, and Outcomes
Bariatric surgery achieves greater and more sustained weight loss than any non-surgical intervention for severe obesity, and — uniquely — can achieve remission of type 2 diabetes through mechanisms that are partially independent of weight loss itself. It is not a treatment of last resort but a treatment appropriate for patients who meet the defined criteria and whose obesity-related health burden warrants the expected risk-benefit balance of the procedure. The evidence base is robust: the Swedish Obese Subjects (SOS) study, a prospective cohort of over 4,000 participants, demonstrated 20-year sustained weight loss of 18–23% with bariatric surgery vs 0% in matched controls, and significant reduction in T2DM incidence, cardiovascular events, cancer incidence, and all-cause mortality.
Indications for bariatric surgery in India (modified for Asian-Indian BMI thresholds):
The Obesity Surgery Society of India (OSSI) and OMAI guidelines use Asian-Indian cut-offs:
- BMI ≥ 37.5 kg/m² without obesity-related comorbidities
- BMI ≥ 32.5 kg/m² with one or more major obesity-related comorbidities: T2DM, hypertension, OSA, NAFLD/NASH, dyslipidaemia, osteoarthritis with functional limitation
- Metabolic surgery for T2DM: BMI ≥ 27.5 kg/m² in patients with poorly controlled T2DM despite optimal medical therapy is an emerging indication (recommended in the 2nd Diabetes Surgery Summit guidelines), particularly when HbA1c remains ≥8% on multiple agents.
- Prerequisites: documented failure of structured lifestyle modification programme (typically 6 months), psychological evaluation, and absence of contraindications.
- Contraindications: reversible endocrine cause of obesity (must be treated first), active substance abuse, uncontrolled psychiatric illness, inability to comply with post-operative dietary requirements, pregnancy, and irreversible medical conditions limiting life expectancy.
Major bariatric procedures and their mechanisms:
Roux-en-Y Gastric Bypass (RYGB):
The gold-standard procedure. A small gastric pouch (~30 mL) is created by stapling the stomach; the small bowel is divided and the distal limb is brought up to anastomose with the gastric pouch (the Roux limb), bypassing the rest of the stomach and the duodenum/proximal jejunum. Mechanisms of weight loss: (1) restriction (small pouch = early satiety), (2) malabsorption (bypassed proximal bowel = reduced caloric absorption), (3) gut hormone changes — GLP-1 secretion is dramatically increased after RYGB (food delivered directly to distal ileum bypassing proximal gut), producing potent incretin effect and contributing to T2DM remission independent of weight loss. Expected weight loss: 30–35% total body weight at 2 years. T2DM remission rates: 60–80%.
Laparoscopic Sleeve Gastrectomy (LSG):
Currently the most frequently performed bariatric procedure worldwide, including in India. The stomach is stapled vertically, removing ~80% of its greater curvature and creating a sleeve-shaped tube (approximately 100–150 mL). Mechanism: predominantly restrictive (smaller stomach = early satiety + reduced caloric intake), with secondary gut hormone effects (removal of ghrelin-producing gastric fundus reduces hunger signals). Expected weight loss: 25–30% total body weight at 2 years. T2DM remission rates: 50–60%. Advantages over RYGB: simpler procedure, fewer long-term nutritional complications, no anastomosis (reduced leak risk), reversible (in principle). Limitations: no malabsorptive component; can have GORD (gastro-oesophageal reflux) as a complication, particularly if hiatus hernia is present.
Laparoscopic Adjustable Gastric Banding (LAGB):
A silicone band is placed around the upper stomach, creating a small pouch. Adjustable via a subcutaneous port. Purely restrictive. Less effective long-term (highest re-operation rate), falling out of favour in favour of LSG and RYGB.
Biliopancreatic Diversion with Duodenal Switch (BPD-DS):
The most aggressive bariatric procedure, combining sleeve gastrectomy with a long intestinal bypass (only 50–100 cm of common channel for nutrient absorption). Maximum weight loss (40–45% TBW) and T2DM remission rates (90%+), but highest nutritional complication risk (protein malnutrition, fat-soluble vitamin deficiency, bone loss). Reserved for severe super-obesity (BMI ≥50).
Post-operative care and nutritional support:
All bariatric procedures require lifelong nutritional monitoring and supplementation. After RYGB and BPD-DS, mandatory lifelong supplementation includes: iron (oral or IV), calcium (calcium citrate preferred as absorption does not require acid), vitamin D, vitamin B12 (oral or intramuscular), folate, and fat-soluble vitamins. Protein intake ≥60–80 g/day is essential to prevent lean muscle mass loss. 'Dumping syndrome' (early or late) can occur after RYGB — rapid gastric emptying causing vasomotor symptoms (flushing, palpitations, diarrhoea after a large or high-sugar meal) — managed by dietary modification (small frequent meals, avoiding high-sugar items). DEXA scanning for bone density at baseline and annually.
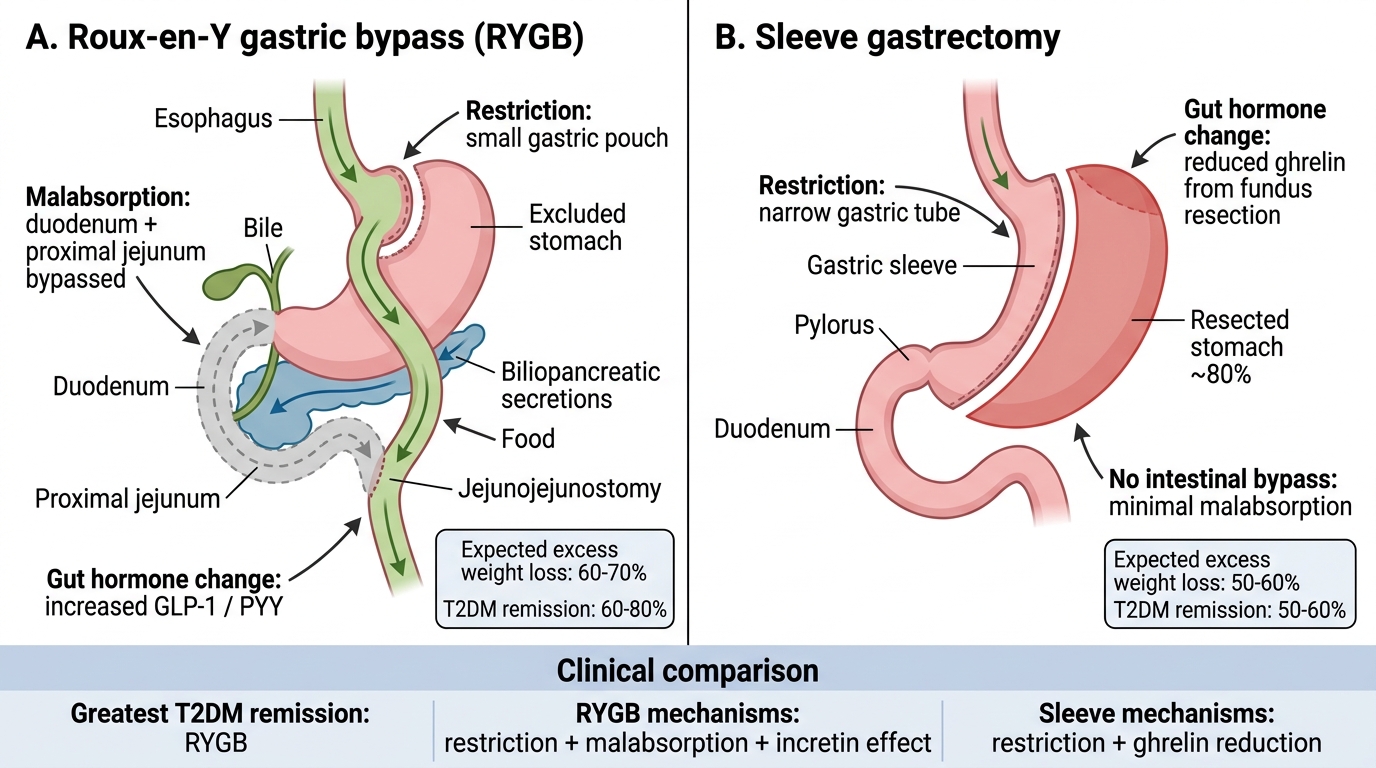
Bariatric Surgery: RYGB vs Sleeve Gastrectomy
SELF-CHECK
A 46-year-old man with BMI 38 kg/m², type 2 diabetes (HbA1c 10.2% despite metformin + insulin), hypertension, and OSA has completed a 6-month structured lifestyle programme with only 4% weight loss. He is referred for bariatric surgery assessment. Which procedure provides the greatest T2DM remission rate and through what mechanism?
A. Laparoscopic adjustable gastric banding — purely restrictive mechanism reducing caloric intake
B. Laparoscopic sleeve gastrectomy — reduces ghrelin and provides 50–60% T2DM remission
C. Roux-en-Y gastric bypass — combines restriction, malabsorption, and dramatic GLP-1 increase, with T2DM remission rates of 60–80%
D. Biliopancreatic diversion with duodenal switch — highest weight loss but not suitable for BMI 38
Reveal Answer
Answer: C. Roux-en-Y gastric bypass — combines restriction, malabsorption, and dramatic GLP-1 increase, with T2DM remission rates of 60–80%
Roux-en-Y gastric bypass (RYGB) provides the highest T2DM remission rate among standard procedures, approximately 60–80%, through a combination of mechanisms: restriction (small gastric pouch), caloric malabsorption (bypassed proximal bowel), and — most importantly — dramatic increase in post-prandial GLP-1 secretion when food is delivered directly to the distal ileum, producing potent incretin-mediated insulin secretion and T2DM remission independent of weight loss itself. Sleeve gastrectomy has T2DM remission rates of 50–60% (lower than RYGB). Adjustable gastric banding is the least effective for T2DM remission. BPD-DS has the highest remission rate (~90%) but is typically reserved for super-obesity (BMI ≥50) and carries the highest nutritional complication risk; BMI 38 kg/m² would generally be treated with RYGB or sleeve gastrectomy.
Prevention: Educating Patients, Health Workers, and the Public
Obesity prevention operates at three levels: primary prevention (preventing obesity from developing in those currently at healthy weight), secondary prevention (early identification and intervention in overweight individuals to prevent progression to obesity and its complications), and tertiary prevention (reducing the impact of established obesity through treatment of comorbidities and sustained weight management). As a clinician, you will contribute to prevention at all three levels — in clinical consultations, in community health education, and as an advocate for population-level policies.
Primary prevention — population and community level:
The most powerful drivers of the obesity epidemic are environmental (food environment, built environment, marketing of ultra-processed foods) and are therefore most amenable to policy rather than individual-level advice. As future clinicians, students should be aware of — and able to advocate for — the following evidence-based population interventions:
- Front-of-pack food labelling: mandatory nutritional traffic-light labelling on packaged food to enable informed consumer choice; reduces purchase of high-sugar, high-fat items.
- Sugar-sweetened beverage (SSB) tax: fiscal policy that increases the price of SSBs; the Indian government's GST on carbonated drinks (28% + 12% cess) is a step in this direction. Studies from Mexico, the UK, and Chile demonstrate SSB tax reduces consumption.
- Restrictions on marketing of junk food to children: banning advertising of high-calorie, low-nutrient foods during children's programming.
- Urban planning for active transport: building footpaths, cycling lanes, parks, and public recreational spaces — the built environment is a major determinant of physical activity.
- School-based interventions: promoting physical education, replacing SSBs and ultra-processed snacks in school canteens with healthier options, and nutrition literacy curricula.
- Workplace wellness programmes: activity breaks, healthy canteen options, standing desks, and health screening in large workplaces.
Key public health messages for individual and community education:
1. A 5–10% reduction in body weight (e.g., 5 kg in a 70 kg person) produces clinically meaningful reduction in blood pressure, blood glucose, and triglycerides — this achievable goal is motivating and actionable.
2. Replace one SSB per day with water or buttermilk — simple, culturally appropriate, high-impact.
3. 30 minutes of brisk walking daily is achievable and reduces cardiovascular risk; it does not require a gym or equipment.
4. Cook with measured oil — one to two teaspoons per person per meal, not free-pouring.
5. Eat traditional whole grains (millets, red rice, whole wheat) rather than refined grains — the nutrition transition away from these staples has driven India's obesity epidemic.
6. Childhood obesity is a family problem — obese children in obese families require family-based interventions, not child-only counselling.
7. Mental health support matters — depression and stress are underaddressed drivers of obesity; removing stigma from seeking mental health care reduces emotional eating.
Role of the clinician as educator:
In the NMC framework, IM14.14 explicitly requires you to educate patients, health workers, and the public. In practice, this means:
- Brief counselling at every clinical encounter for patients with BMI ≥23 kg/m² (Asian-Indian threshold)
- Leading or contributing to community health education sessions, school health talks, and workplace health camps
- Training nurses, paramedical staff, and community health workers to measure waist circumference correctly, screen for obesity using Asian-Indian cut-offs, and apply brief motivational counselling
- Advocating for evidence-based public health policies at institutional and national level
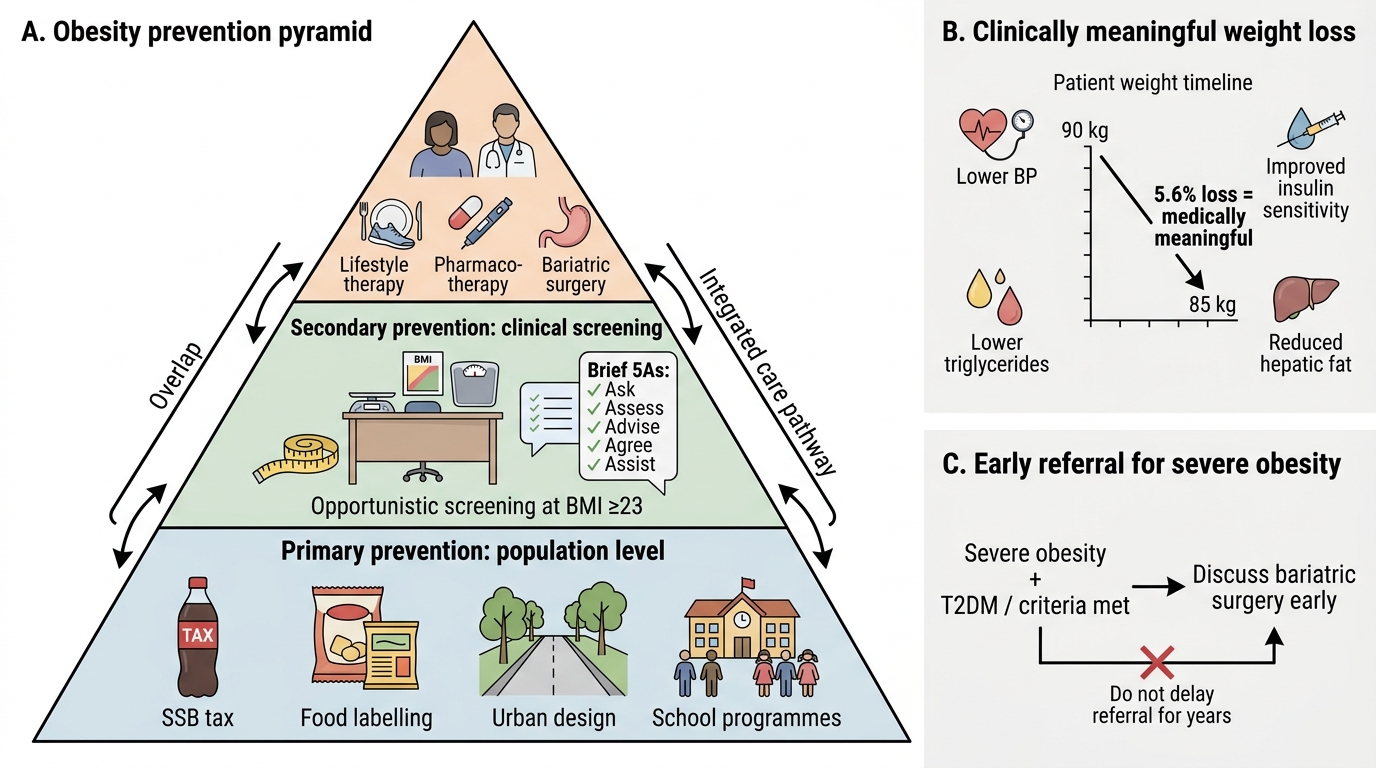
Three-Tier Obesity Prevention Pyramid
CLINICAL PEARL
The most evidence-based sentence in obesity pharmacotherapy is: 'Weight loss of 5% is the minimum clinically meaningful threshold.' A patient who started at 90 kg and is now 85 kg (5.6% loss) may feel disappointed — 'I've only lost 5 kg.' But they have measurably reduced their blood pressure, improved insulin sensitivity, lowered triglycerides, and reduced hepatic fat. Frame this early victory explicitly: 'You have achieved a medically meaningful weight loss — your body is already healthier. This is the foundation we build on.' This reframing reinforces self-efficacy and sustains motivation for the continued effort needed to reach larger targets.
Second pearl: bariatric surgery is not 'giving up on the patient.' It is the most effective long-term treatment for severe obesity and should be discussed proactively — not as a last resort after years of failed attempts — with any patient meeting the criteria. Delayed referral is a common clinical error; the patient with BMI 38 and T2DM will likely achieve better long-term outcomes with early surgery than with another decade of escalating pharmacotherapy.
Self-Assessment: Integrating Counselling and Treatment
The scenarios below require you to integrate all four components of this module: non-judgemental counselling technique, dietary/lifestyle modification prescription, pharmacotherapy selection, and prevention messaging. Each scenario is followed by an analysis.
Scenario A: Deepa is a 35-year-old woman, BMI 29 kg/m² (obese, Asian-Indian), with T2DM (HbA1c 8.2% on metformin) and hypertension (BP 144/90 on amlodipine). She has tried three different diets in the past two years, lost 3–4 kg each time, and regained the weight within 3 months. She is frustrated and says: 'Why even try if it always comes back?' What is your counselling approach and treatment plan?
Analysis: Validate her frustration first — 'Losing weight and regaining it is very common, and it is not a sign of failure. Your body has biological systems that resist weight loss, and each attempt builds knowledge and skills.' Explore barriers: what made her regain each time? Identify the most actionable change. She has T2DM + obesity with inadequate glycaemic control: she meets the pharmacotherapy criteria (BMI ≥27.5 with comorbidities). A GLP-1 receptor agonist (liraglutide or semaglutide) is the ideal choice — it addresses both obesity and glycaemic control and reduces cardiovascular risk. Discuss the biological basis for her previous 'failures' — this removes self-blame and motivates engagement with treatment. Set a 3-month target: ≥5% weight loss and HbA1c improvement.
Scenario B: A community health worker at a rural health camp measures a 42-year-old farmer, Sunil, at BMI 24 kg/m² (overweight, Asian-Indian) with waist circumference 96 cm and fasting glucose 118 mg/dL. He has no current symptoms. What prevention message is most appropriate?
Analysis: Sunil has central obesity (waist ≥90 cm, Asian-Indian men) + impaired fasting glucose (100–125 mg/dL = pre-diabetes). He has at least 2 of the 5 IDF metabolic syndrome components. Despite BMI 24 being 'normal' by Western standards, by Asian-Indian criteria he is overweight AND has central obesity and pre-diabetes. Prevention message: 'Your waist circumference and blood sugar are in the danger zone. But the good news is that at this stage, small changes work very well. Losing even 3–4 kg, replacing rice with millets, and walking 30 minutes daily can stop this from becoming diabetes.' Refer for structured lifestyle programme; recheck fasting glucose and waist circumference in 3 months.
Scenario C: Arvind, 44 years old, BMI 41 kg/m², T2DM (HbA1c 11.4% on insulin + metformin), hypertension, and severe OSA (AHI 42 on polysomnography) has been on a supervised lifestyle programme for 8 months. He has lost 4% of body weight. He is considering bariatric surgery. Does he meet the criteria? What procedure would you discuss first?
Analysis: Yes, he meets the criteria. Criteria: BMI ≥32.5 with major comorbidities (T2DM, hypertension, severe OSA) — he has all three, and his BMI of 41 kg/m² also exceeds the BMI ≥37.5 standalone threshold. Documented failure of structured lifestyle programme (8 months, <5% loss). Discuss RYGB as the preferred procedure given the combination of BMI 41 and severe T2DM requiring insulin — RYGB provides the highest T2DM remission rate (60–80%), addresses OSA severity through weight loss, and has the strongest long-term outcome data. Pre-operative workup: psychological evaluation, nutritional assessment, cardiac clearance, endoscopy, and optimisation of glycaemic control pre-operatively (target HbA1c <10% before surgery).
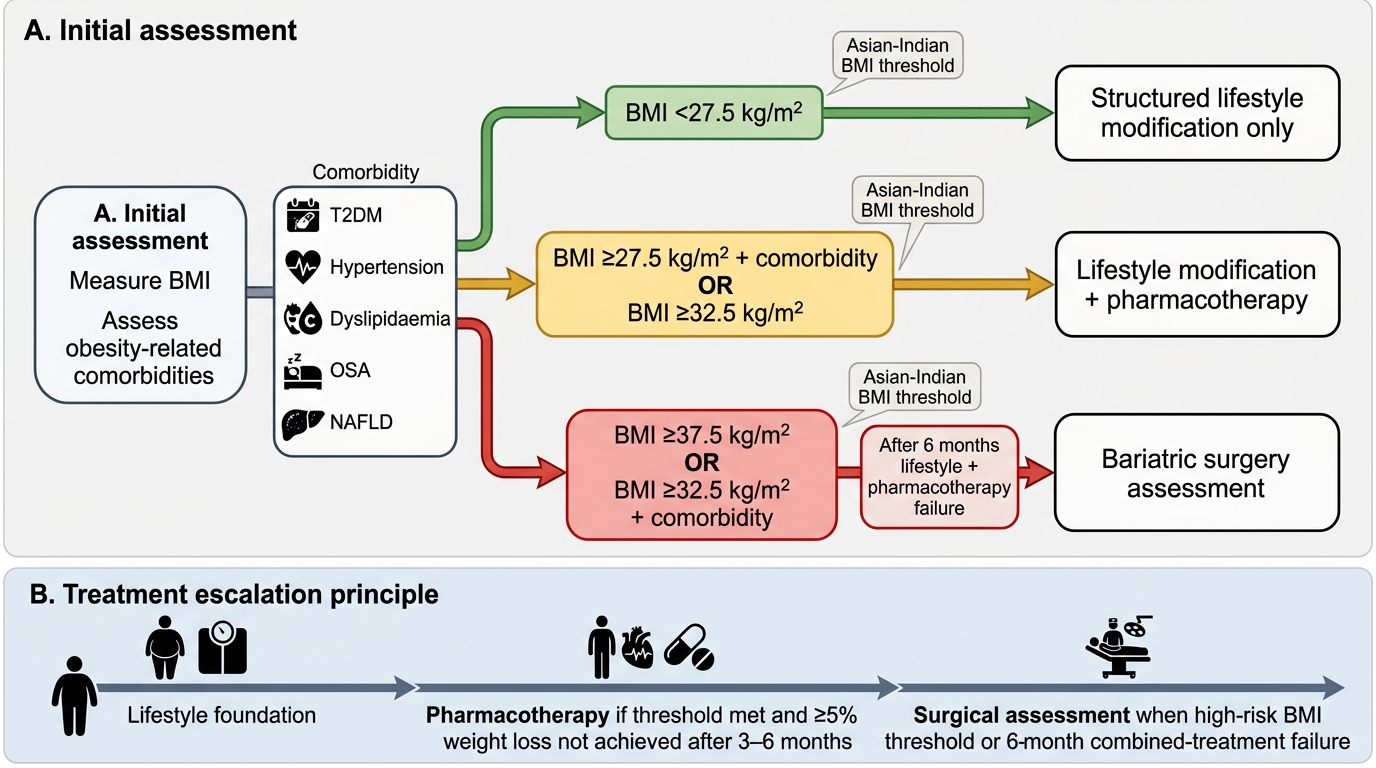
Obesity Treatment Decision Framework