Page 3 of 15
IM14.1-5 | Obesity Foundations — SDL Guide (Part 3)
Overview of the Management Approach: Principles and Rationale
The management of obesity follows a stepwise intervention ladder — lifestyle modification forms the foundation, pharmacotherapy is added when lifestyle measures fail to achieve clinically meaningful weight loss, and bariatric surgery is reserved for severe cases meeting specific criteria. Detailed management, including pharmacotherapy and bariatric indications, is covered in the 'Obesity Counselling and Treatment' module. The principles underpinning the ladder are reviewed here to complete the arc from pathophysiology and complications to intervention.
The overarching therapeutic goals in obesity management are: (1) achieve and sustain clinically meaningful weight loss — a minimum 5–10% reduction in total body weight has been consistently shown to reduce blood pressure, improve glycaemia and insulin sensitivity, lower triglycerides, reduce hepatic fat, and decrease OSA severity; (2) treat or prevent obesity-related comorbidities (diabetes, hypertension, dyslipidaemia, NAFLD, OSA); and (3) improve quality of life, functional capacity, and psychological wellbeing.
Lifestyle modification — encompassing dietary therapy (caloric restriction, diet quality, meal timing), structured physical activity, and behavioural interventions — is the first-line treatment for all patients and remains the cornerstone on which all other interventions are built. The importance of a caloric deficit of 500–750 kcal/day below energy expenditure is well established; this produces a weight loss of approximately 0.5–0.75 kg/week. Diet quality (not just calorie quantity) matters — reducing ultra-processed foods, sugar-sweetened beverages, and refined carbohydrates while increasing fibre, vegetables, and protein is the evidence-based approach. Physical activity recommendations for weight management are ≥150–300 minutes/week of moderate-intensity aerobic exercise, with resistance training to preserve lean muscle mass.
Pharmacotherapy is added in patients with BMI ≥ 27.5 kg/m² (Asian-Indian threshold) with comorbidities, or BMI ≥ 32.5 kg/m², when adequate lifestyle modification over 3–6 months has not achieved the target weight loss. Approved agents in India include orlistat (pancreatic lipase inhibitor) and liraglutide/semaglutide (GLP-1 receptor agonists — also with cardiovascular and renal benefits). Pharmacotherapy must always be combined with lifestyle modification.
Bariatric surgery achieves greater and more sustained weight loss than any non-surgical intervention. Indications in India: BMI ≥ 37.5 kg/m² without comorbidities, or BMI ≥ 32.5 kg/m² with major obesity-related comorbidities (T2DM, hypertension, OSA, NAFLD). Procedures include sleeve gastrectomy and Roux-en-Y gastric bypass. Bariatric surgery can achieve remission of type 2 diabetes independent of weight loss, through incretin and gut-hormone-mediated mechanisms.
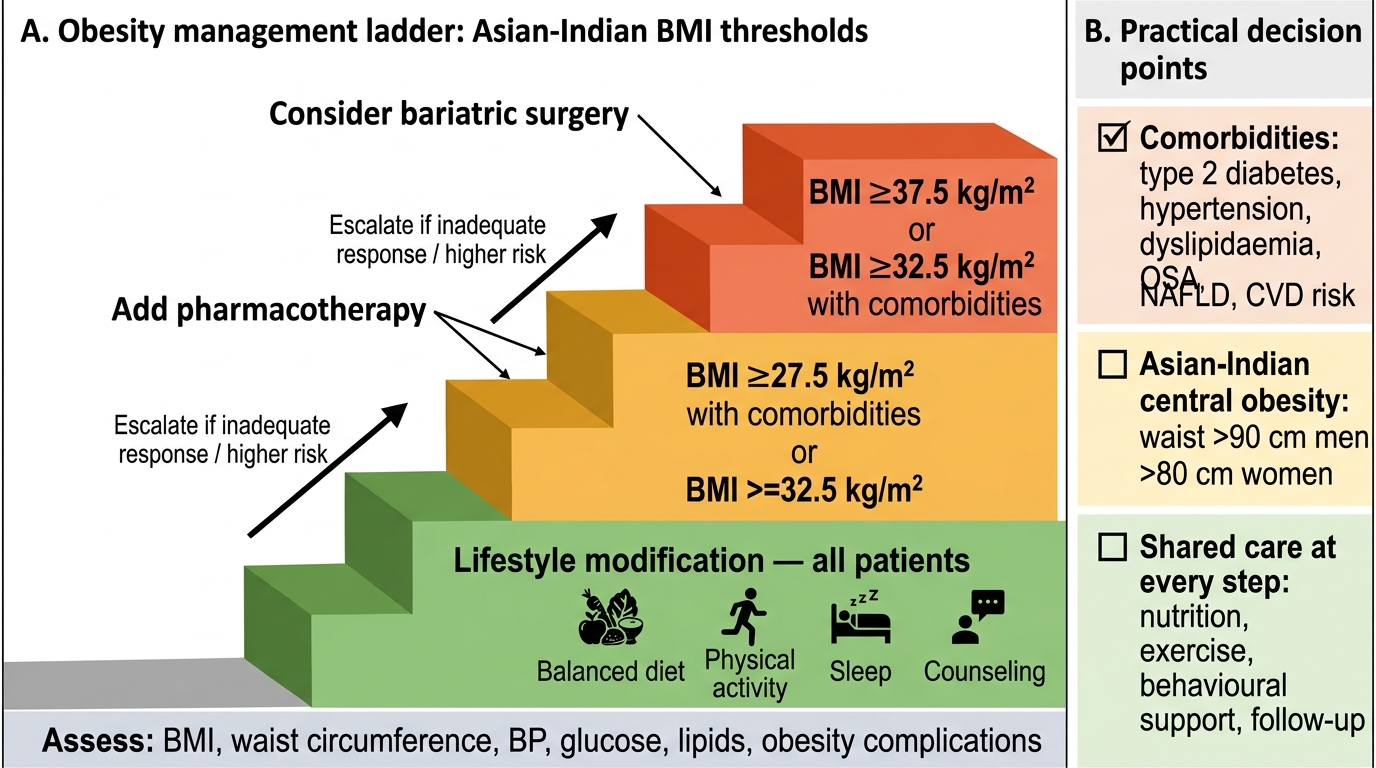
Obesity Management Ladder: Asian-Indian BMI Thresholds
Self-Assessment: Applying Obesity Foundations
You have now covered the key conceptual foundations of obesity for Indian practice: ethnicity-specific definitions and measurements, the full aetiological spectrum from modifiable risk factors to rare monogenic causes, the natural history from adipose tissue dysfunction to multi-organ complications, and the metabolic syndrome framework. The scenarios below test application of this knowledge.
Scenario A: Sunita is a 29-year-old woman who presents for a health check. Her BMI is 23.5 kg/m² and waist circumference is 84 cm. She is asymptomatic. Using Asian-Indian criteria, what is her BMI category and her abdominal obesity status, and what metabolic-syndrome components should you screen for?
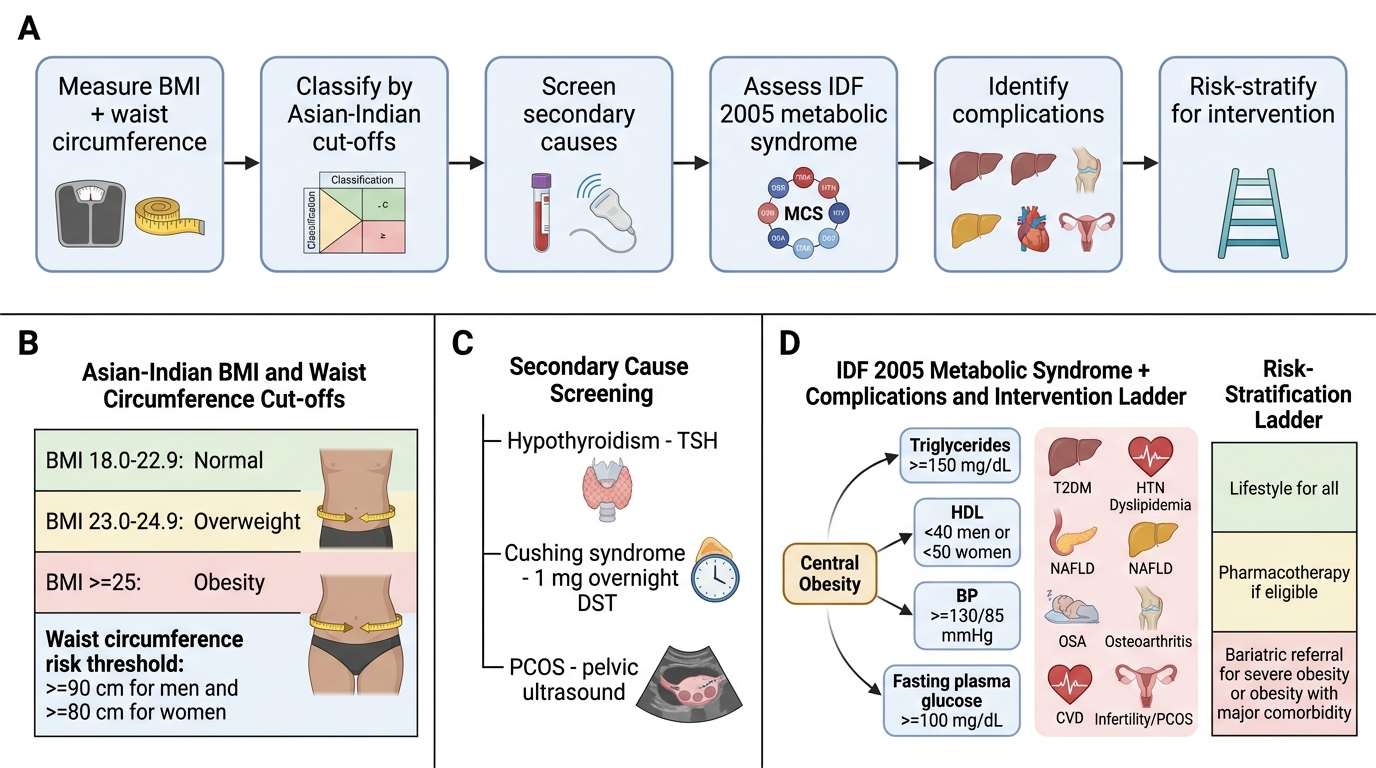
Analysis: BMI 23.5 kg/m² = overweight by Asian-Indian cut-offs (normal upper limit is 22.9). Waist 84 cm in a woman exceeds the 80 cm threshold for Asian-Indian women — she has central obesity. She meets the IDF 2005 mandatory criterion for metabolic syndrome. She should be screened for fasting triglycerides, HDL, fasting glucose, and blood pressure to determine how many additional components she meets. Counselling on lifestyle modification should begin at this stage, before complications develop.
Scenario B: A 6-year-old boy presents with severe obesity since infancy, constant hyperphagia, and a history of neonatal hypotonia and poor feeding. He has mild intellectual disability and behavioural problems. He is currently obese and his family is distressed. What syndrome should you suspect and what is the genetic mechanism?
Analysis: This is the classic presentation of Prader-Willi syndrome — neonatal hypotonia and poor feeding followed by severe hyperphagia and rapid weight gain in early childhood, intellectual disability, and behavioural issues. The genetic mechanism is a deletion of the paternal chromosome 15q11-q13 region (or uniparental maternal disomy, or imprinting defect). This is syndromic, not monogenic; growth hormone therapy may be indicated. Genetic testing (methylation analysis) is confirmatory.
Scenario C: A 50-year-old woman with long-standing obesity has a BMI of 32 kg/m² and reports increasing fatigue, constipation, cold intolerance, and puffiness around her eyes over the past year. Her weight has increased 8 kg in 12 months despite no change in diet or activity. Which secondary cause must be excluded and with what test?
Analysis: The combination of obesity, fatigue, constipation, cold intolerance, and periorbital puffiness strongly suggests hypothyroidism. This is a classic secondary cause of obesity. The screening test is serum TSH — elevated TSH (primary hypothyroidism) confirms the diagnosis and necessitates levothyroxine replacement before attributing all weight gain to lifestyle factors.
Clinical Approach to Obesity