Page 1 of 19
IM15.{1-3,6} | GI Bleeding Foundations and Stabilisation — SDL Guide
Learning Objectives
- Enumerate and classify the major causes of upper and lower GI bleeding
- Distinguish UGIB from LGIB on the basis of clinical features
- Describe the pathophysiological consequences of acute blood and volume loss
- Outline the immediate steps in stabilising a patient with acute GI haemorrhage including airway, IV access, fluid resuscitation, and transfusion triggers
INSTRUCTIONS
Gastrointestinal bleeding is one of the most common and potentially lethal medical emergencies encountered by any physician. This module builds your understanding of the causes and pathophysiology of GI haemorrhage and drills the first critical skill — systematic stabilisation of the bleeding patient before any definitive diagnostic workup begins.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 47 — Gastrointestinal Bleeding (textbook)
- API Textbook of Medicine, 10th ed. — Gastrointestinal Haemorrhage (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 21 — Alimentary Tract and Pancreatic Disease (textbook)
- British Society of Gastroenterology: UK guidelines on the management of upper gastrointestinal bleeding, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 3 AM in the emergency department. A 55-year-old man with a history of chronic alcohol use is brought in by ambulance after vomiting approximately 600 mL of fresh red blood at home. He is diaphoretic, his pulse is 118 beats per minute, blood pressure 88/60 mmHg, and he is breathing rapidly at 24 breaths per minute. His abdomen is mildly distended with shifting dullness. The house officer on duty freezes for a moment — the patient looks critically ill and is asking what to do first. Endoscopy? CT scan? A dose of omeprazole? None of those is the right first step. Every second of delay in establishing large-bore IV access, beginning fluid resuscitation, and calling for blood products moves this man closer to haemorrhagic shock and death. The ability to stabilise a bleeding patient before diagnostics is not a gastroenterology skill — it is a survival skill every physician must own.
WHY THIS MATTERS
Acute GI bleeding accounts for approximately 150 hospital admissions per 100,000 population per year in high-income settings, and the burden is substantially higher in India where peptic ulcer disease, variceal bleeding from chronic liver disease, and portal hypertension secondary to hepatitis B and C are extremely prevalent. In-hospital mortality for upper GI bleeding (UGIB) ranges from 5–14% overall and exceeds 30% for variceal bleeding in patients with decompensated cirrhosis. The physician who arrives at the bedside of a GI bleed patient must act as resuscitator and diagnostician simultaneously. NMC competencies IM15.1 through IM15.6 address this foundational triad: aetiology (what bleeds), pathophysiology (why it is dangerous), and stabilisation (what to do first). These are not academic exercises — they are the framework that separates a managed emergency from a preventable death.
RECALL
Before we proceed, recall the fundamentals that underpin GI haemorrhage physiology. The gastrointestinal tract is divided by the ligament of Treitz (the duodenojejunal flexure) into upper GI (oesophagus, stomach, duodenum) and lower GI (jejunum, ileum, colon, rectum, anus). Recall the Frank-Starling mechanism — cardiac output is preload-dependent, and any significant reduction in intravascular volume reduces ventricular filling and stroke volume, triggering a compensatory tachycardia and peripheral vasoconstriction mediated by the sympathoadrenal axis. Recall also that the body's compensatory mechanisms can maintain blood pressure until approximately 20–30% of circulating blood volume is lost — at which point the clinical picture deteriorates rapidly. Finally, recall the distinction between haematemesis (vomiting blood — origin almost always proximal to the ligament of Treitz), melaena (black tarry stool — digested blood from UGIB or proximal small bowel), and haematochezia (fresh red blood per rectum — usually LGIB, but can be massive UGIB).
Clinical Presentation and the UGIB–LGIB Distinction
Gastrointestinal bleeding (GI bleeding) is the passage of blood from anywhere along the gastrointestinal tract, from the mouth to the anus. The clinical presentation is shaped by the anatomical site, the rate of bleeding, and the patient's underlying physiology and comorbidities. Correctly localising the bleed to the upper or lower GI tract within the first few minutes of assessment is essential because the aetiologies, initial management priorities, and specialist inputs differ substantially between the two. The clinical features that permit this distinction are well-established and reliable in the majority of cases.
Provided image
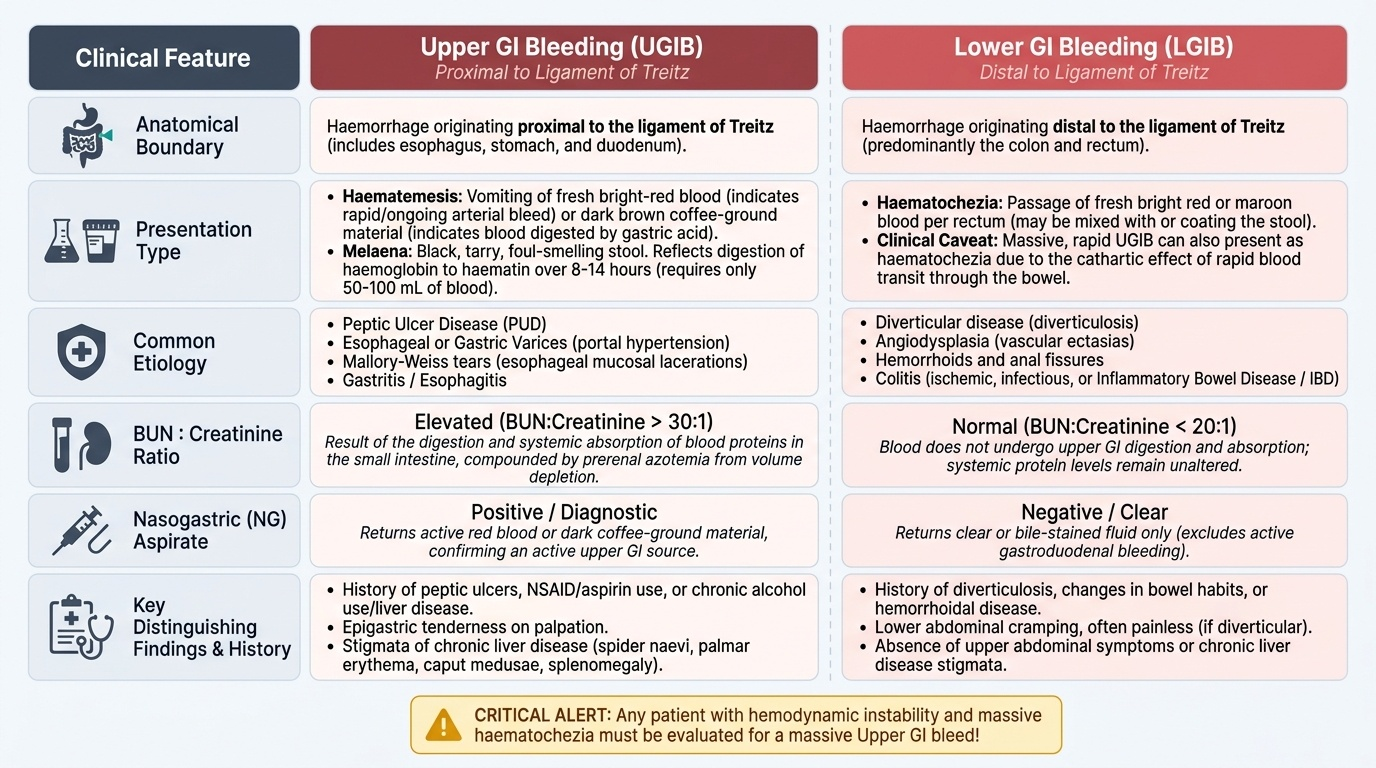
Upper GI bleeding (UGIB) refers to haemorrhage originating proximal to the ligament of Treitz, which marks the duodenojejunal junction. The cardinal symptom is haematemesis — vomiting of blood, which may appear as fresh bright-red blood (indicating rapid or ongoing arterial haemorrhage) or as dark brown 'coffee-ground' material (indicating slower bleeding that has been exposed to gastric acid and undergone partial digestion). Melaena — the passage of black, tarry, foul-smelling stool — is the most specific sign of UGIB, reflecting the digestion of haemoglobin to haematin by intestinal bacteria as blood transits the gut over 8–14 hours. Approximately 50–100 mL of blood in the GI tract is sufficient to produce melaena. Clinical context that strongly points to UGIB includes a history of peptic ulcer disease, NSAID or aspirin use, chronic alcohol use or known liver disease (variceal risk), anticoagulant or antiplatelet therapy, previous aortic graft surgery (aortoenteric fistula risk), and a prior history of UGIB. On examination, epigastric tenderness, stigmata of chronic liver disease (spider naevi, palmar erythema, caput medusae, splenomegaly), and an actively nasogastric aspirate returning blood all point to an upper source.
Lower GI bleeding (LGIB) refers to haemorrhage from below the ligament of Treitz — predominantly from the colon. The characteristic presentation is haematochezia — the passage of fresh red or maroon blood per rectum, which may be mixed with stool, coating the stool, or appearing as pure blood. However, a critical caveat applies: massive, rapid UGIB (typically arterial) can present with haematochezia because blood acts as a cathartic and transits the bowel too quickly to be digested into melaena. Haematochezia from a suspected lower source in a haemodynamically unstable patient must always prompt exclusion of a massive upper source first. Symptom context favouring LGIB includes a history of diverticular disease, colonic polyps or colorectal carcinoma (altered bowel habits, weight loss, iron-deficiency anaemia), inflammatory bowel disease (IBD), or haemorrhoids and anal fissure (blood coating stool, associated with perianal pain and fresh blood on the toilet paper).
An important laboratory aid is the blood urea nitrogen (BUN) to creatinine ratio: digestion of blood protein in the small bowel raises BUN disproportionately compared to creatinine, so a BUN:creatinine ratio above 20:1 (or BUN/creatinine >30 in non-SI units) in the absence of pre-existing renal disease is a useful pointer toward an upper source. This simple calculation is often overlooked but adds real diagnostic value when the clinical picture is ambiguous.
Aetiology of Upper and Lower GI Bleeding
The causes of GI bleeding span a wide spectrum, from the common and easily managed to the rare and immediately life-threatening. A systematic aetiological approach mapped to the anatomical compartment ensures that no important diagnosis is overlooked and guides the prioritisation of both investigation and management. Understanding the mechanism behind each aetiology is not academic — it directly informs which treatments are appropriate and which interventions to avoid in specific patient groups.
Provided image
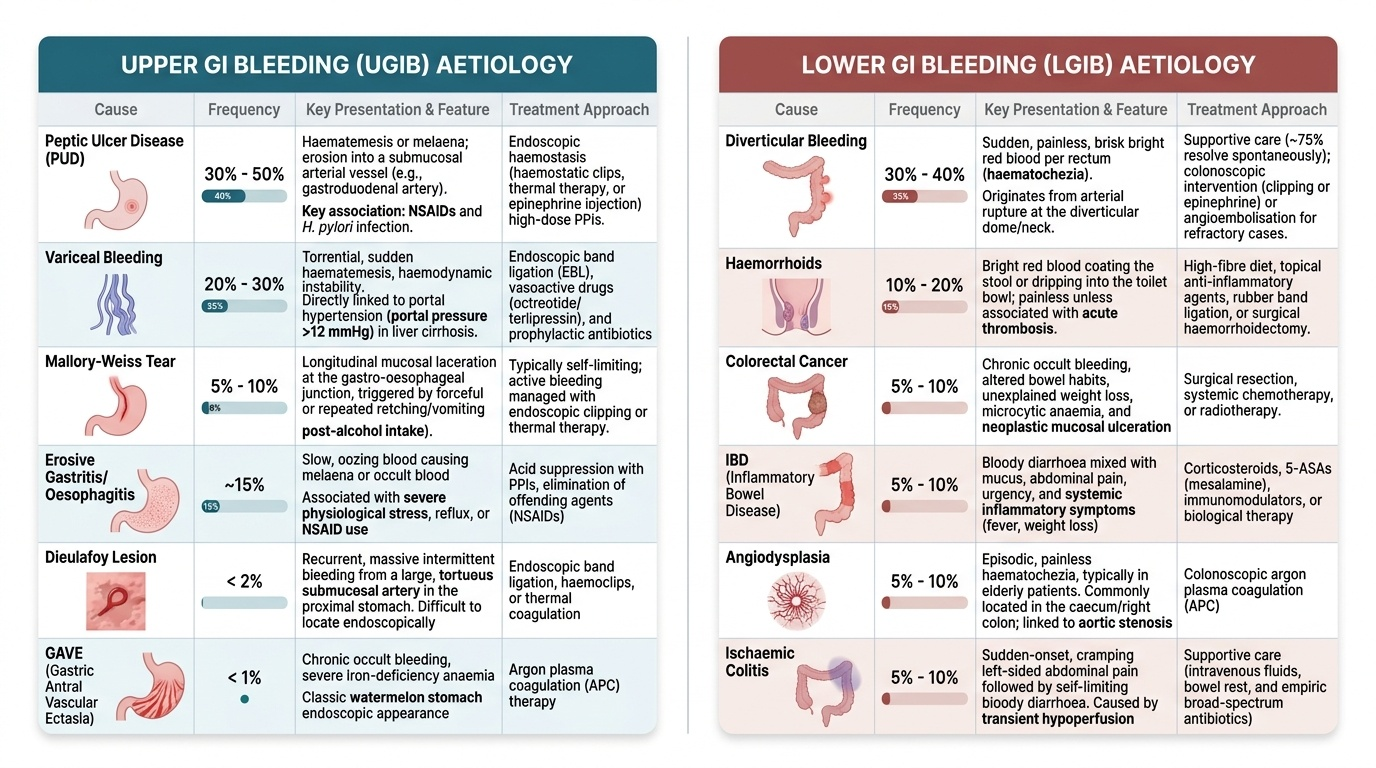
Upper GI bleeding aetiology: The commonest cause of UGIB worldwide is peptic ulcer disease (PUD), accounting for approximately 30–50% of cases. Gastric and duodenal ulcers bleed when they erode into a submucosal or submucosal arterial vessel; the most dangerous is the gastroduodenal artery underlying a posterior duodenal ulcer (Forrest class Ia — spurting arterial haemorrhage carries a rebleed risk of ~55% without intervention). NSAID use and Helicobacter pylori infection are the two principal causes of peptic ulceration in India. Variceal bleeding accounts for 20–30% of UGIB in India, given the high prevalence of hepatitis B-related and alcoholic cirrhosis; oesophageal varices form when portal pressure exceeds 12 mmHg and are a direct consequence of portal hypertension. Variceal haemorrhage is distinctive: it is often torrential, carries a 6-week mortality of 20–30% in decompensated cirrhosis, and requires specific vasoactive therapy (octreotide or terlipressin) and antibiotic prophylaxis in addition to endoscopic band ligation. Mallory–Weiss tears — longitudinal mucosal lacerations at the gastrooesophageal junction from forceful or repeated retching — are common in alcoholic patients and typically self-limiting but occasionally require endoscopic haemostasis. Erosive gastritis and oesophagitis (stress ulceration, NSAID-related, or reflux-associated) account for approximately 15% of UGIB. Less common but important causes include Dieulafoy lesion (a tortuous submucosal artery that bleeds without overlying ulceration, typically in the proximal stomach — difficult to identify endoscopically), gastric antral vascular ectasia (GAVE), aortoenteric fistula (a surgical emergency in any patient with a prior aortic graft who presents with GI bleeding), and haemobilia (bleeding into the biliary tree, classically after hepatic trauma or percutaneous biliary procedure, presenting as the Quincke triad: right upper quadrant pain, jaundice, and haematemesis or melaena).
Lower GI bleeding aetiology: In India and globally, diverticular disease is the single most common cause of significant LGIB in adults over 50 — accounting for 30–50% of acute lower bleeds in the elderly. Diverticular bleeding arises when the neck of a diverticulum erodes an adjacent arteriole and is typically abrupt, painless, and large-volume, but ceases spontaneously in 75–80% of cases. Haemorrhoids are the most prevalent anorectal cause overall, though the bleeding is generally modest (bright red blood coating stool or dripping into the pan). Colorectal carcinoma and colonic polyps are important causes especially in adults over 40 and in those with family history or prior polyps — the blood loss is often occult or intermittent rather than dramatically acute. Inflammatory bowel disease (IBD) — both Crohn's disease and ulcerative colitis — produces bloody diarrhoea rather than isolated haemorrhage; the context of chronic symptoms, mucus, and systemic inflammation distinguishes it from diverticular bleeding. Angiodysplasia (arteriovenous malformations, AVMs) of the colon, typically in patients over 60 and associated with aortic stenosis and renal failure (Heyde's syndrome), produces recurrent modest bleeds. Ischaemic colitis, Meckel's diverticulum (the most common congenital small bowel anomaly — typically presents in children and young adults, painless massive haematochezia), mesenteric vascular disease, and infective colitis (Salmonella, Shigella, Campylobacter, Clostridioides difficile) complete the differential.
SELF-CHECK
A 62-year-old man presents with passage of black tarry stool and a blood urea nitrogen of 48 mg/dL with creatinine of 1.1 mg/dL (ratio ~44). He denies haematemesis. His nasogastric aspirate returns coffee-ground material. Which anatomical source of bleeding is most consistent with this picture?
A. Descending colon, consistent with diverticular bleeding
B. Rectosigmoid junction, consistent with colorectal carcinoma
C. Proximal to the ligament of Treitz, consistent with upper GI bleeding
D. Terminal ileum, consistent with Meckel's diverticulum
Reveal Answer
Answer: C. Proximal to the ligament of Treitz, consistent with upper GI bleeding
Melaena (black tarry stool) indicates digested blood — the transit time to produce melaena requires approximately 8 hours of intestinal transit. The elevated BUN:creatinine ratio (44:1 — far above the 20:1 upper GI threshold) reflects protein digestion of blood in the small bowel raising BUN disproportionately, consistent with an upper GI source. Coffee-ground nasogastric aspirate directly confirms upper GI origin. Diverticular and colorectal carcinoma bleeding typically presents as haematochezia (fresh blood per rectum) without coffee-ground aspirate. Meckel's bleeding also causes haematochezia and is most common in children.
Pathophysiology of Acute Blood and Volume Loss
To understand why a patient with GI haemorrhage deteriorates and how to respond effectively, the physician must have a precise mental model of the pathophysiological cascade that follows acute blood loss. Haemorrhagic shock is not simply 'low blood pressure from bleeding' — it is a multi-organ system failure process that, if not interrupted early, becomes self-perpetuating and ultimately irreversible. Understanding the physiology enables rational prioritisation: it explains why the sequence airway → breathing → circulation → IV access → fluid resuscitation is the correct order, and why waiting for investigation results before beginning resuscitation is dangerous.
Provided image
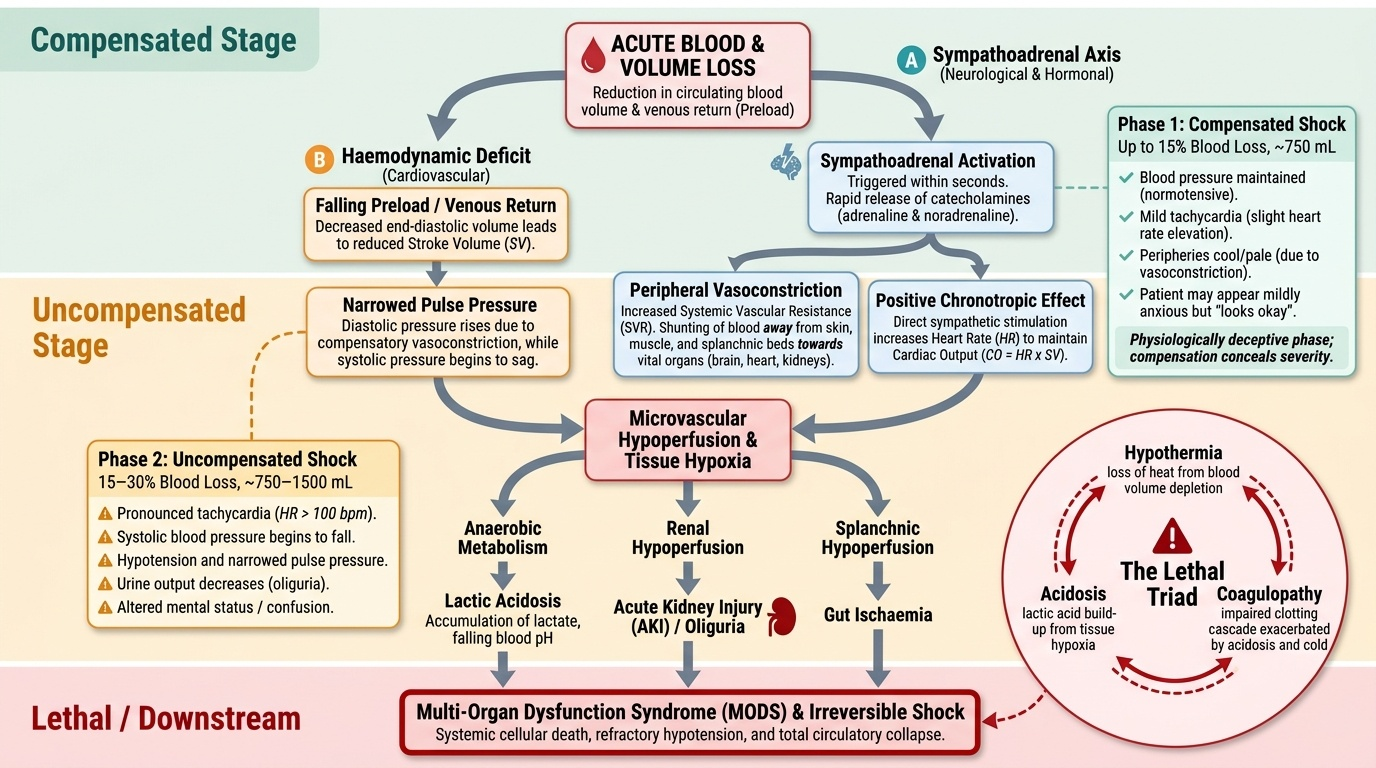
Phase 1 — Compensated haemorrhagic shock (loss of up to 15% circulating blood volume, ~750 mL in a 70 kg adult): The sympathoadrenal axis is activated within seconds of haemorrhage. Catecholamine release (adrenaline from the adrenal medulla, noradrenaline from sympathetic nerve terminals) causes peripheral vasoconstriction, increasing systemic vascular resistance and redistributing blood from skin, skeletal muscle, and splanchnic vessels toward the brain, heart, and kidneys. Heart rate increases through sympathetic chronotropic stimulation. Blood pressure is maintained. The patient may appear mildly anxious and peripherally cool but the vital signs are broadly normal or only mildly tachycardic. This phase is clinically deceptive — the patient 'looks okay' despite significant ongoing haemorrhage.
Phase 2 — Uncompensated shock (15–30% blood volume loss, ~750–1500 mL): Compensatory mechanisms begin to fail. Tachycardia becomes more pronounced (typically >100 bpm). Pulse pressure narrows as diastolic pressure rises from vasoconstriction and systolic pressure begins to fall. Urine output decreases as renal perfusion drops. Confusion or altered consciousness may begin due to cerebral hypoperfusion. The patient is pallid, diaphoretic, and visibly distressed. This is the window in which aggressive fluid resuscitation can restore organ perfusion — the compensatory vasoconstriction is still holding the system together, but decompensation is imminent.
Phase 3 — Decompensated / severe haemorrhagic shock (30–40% blood volume loss, ~1500–2000 mL): Blood pressure falls markedly. The compensatory mechanisms are overwhelmed. Metabolic acidosis develops because inadequate oxygen delivery to tissues forces anaerobic glycolysis, generating lactic acid — lactate >4 mmol/L indicates severe shock and is an independent predictor of mortality. Coagulopathy develops through dilution of clotting factors, hypothermia, and acidosis — the lethal triad (hypothermia, acidosis, coagulopathy) is self-amplifying: acidosis impairs clotting enzymes, coagulopathy worsens haemorrhage, haemorrhage worsens acidosis. Acute kidney injury develops as prolonged renal hypoperfusion causes tubular necrosis. The gut mucosa, already ischaemic from splanchnic vasoconstriction, may lose its barrier function, allowing bacterial translocation.
Phase 4 — Irreversible shock (>40% blood volume loss): Even with resuscitation, organ damage has progressed to the point where recovery is impossible. Multi-organ failure ensues. This stage is largely preventable with rapid, aggressive phase 2–3 intervention.
Two additional pathophysiological points warrant attention in GI bleeding specifically. First, volume loss in GI bleeding is invariably underestimated at the bedside — patients often report having 'passed some blood' when the actual loss is severalfold greater (blood mixed with stool, swallowed blood from nasopharyngeal drip). Serial haematocrit measurements are also misleading acutely because haemoconcentration from compensatory vasoconstriction can maintain haematocrit in the normal range for several hours despite major haemorrhage. Second, compensatory responses are blunted in the elderly, patients on beta-blockers (which block the tachycardic response), and patients with chronically elevated portal pressure (who have an expanded but poorly distributed circulating volume).