Page 9 of 19
IM15.{9-10,16} | GI Bleeding Investigations — SDL Guide (Part 2)
Endoscopy: Indications, Technique Principles, and Risk Stratification
Endoscopy is the cornerstone of both the investigation and treatment of GI bleeding. It offers direct visualisation of the bleeding site, simultaneous tissue sampling (biopsy), and therapeutic capability in a single procedure. Understanding the indications, timing, and risk stratification frameworks for endoscopy — as required by NMC competency IM15.10 — is essential for the physician coordinating a GI bleed patient's care even if they are not the endoscopist.
Upper GI endoscopy (oesophago-gastro-duodenoscopy, OGD): OGD is indicated in all cases of acute UGIB once the patient is haemodynamically stable or has been optimised for the procedure. The BSG/ESGE guidelines recommend that OGD should be performed within 24 hours of presentation for most patients with UGIB; more urgent OGD (within 6–12 hours) is recommended for patients with haemodynamic instability despite initial resuscitation, fresh haematemesis in the clinical context suggesting active arterial bleeding, and high-risk stratification (Glasgow-Blatchford Score ≥6 or pre-endoscopic Rockall Score ≥3). Pre-endoscopy erythromycin (250 mg IV 30–90 minutes before OGD) is recommended to accelerate gastric emptying, improving mucosal visualisation and increasing the diagnostic yield — particularly important in patients with significant recent haemorrhage who may have a blood-filled stomach obscuring the view. In variceal haemorrhage, OGD is both diagnostic and therapeutic: band ligation is the gold-standard endoscopic treatment for oesophageal varices and significantly reduces immediate mortality when combined with vasoactive drugs.
At OGD, the Forrest classification of peptic ulcer stigmata of recent haemorrhage directly drives the decision for endoscopic therapy: Forrest Ia (actively spurting artery — endoscopic haemostasis mandatory: dual therapy with adrenaline injection + thermal coagulation or haemoclip application), Forrest Ib (active oozing — endoscopic therapy recommended), Forrest IIa (visible non-bleeding vessel — endoscopic therapy recommended: rebleed risk ~43% without treatment), Forrest IIb (adherent clot — debated; attempt clot removal and treat underlying vessel; rebleed risk ~22%), Forrest IIc (flat pigmented spot, rebleed risk ~10%) and III (clean base, rebleed risk <5%) — these latter two do not require endoscopic therapy and can be managed medically. Following endoscopic therapy for PUD, the patient should receive a high-dose IV PPI (e.g., pantoprazole or omeprazole 80 mg bolus then 8 mg/hour infusion for 72 hours) which reduces rebleeding and mortality by maintaining a gastric pH >6, in which environment haemostatic clot formation and platelet aggregation are most effective.
Indications for colonoscopy (lower GI bleeding): Colonoscopy is the first-line investigation for significant acute lower GI bleeding in haemodynamically stable patients, and the definitive investigation for chronic or occult lower GI bleeding and suspected colorectal carcinoma. Urgent colonoscopy (within 24 hours) is recommended in patients hospitalised with haematologically significant acute LGIB after adequate bowel preparation — it identifies the source in 48–90% of cases and allows simultaneous therapeutic intervention (haemoclip, diathermy, or adrenaline injection for diverticular bleeding; polypectomy for bleeding polyps; argon plasma coagulation for angiodysplasia). Bowel preparation is required before colonoscopy (unless the bleeding itself has provided a 'natural purge') and should be performed as oral polyethylene glycol solution over 2–4 hours. In patients with severe ongoing haematochezia making bowel preparation impractical, CT angiography or angiography is preferred over unprepared colonoscopy.
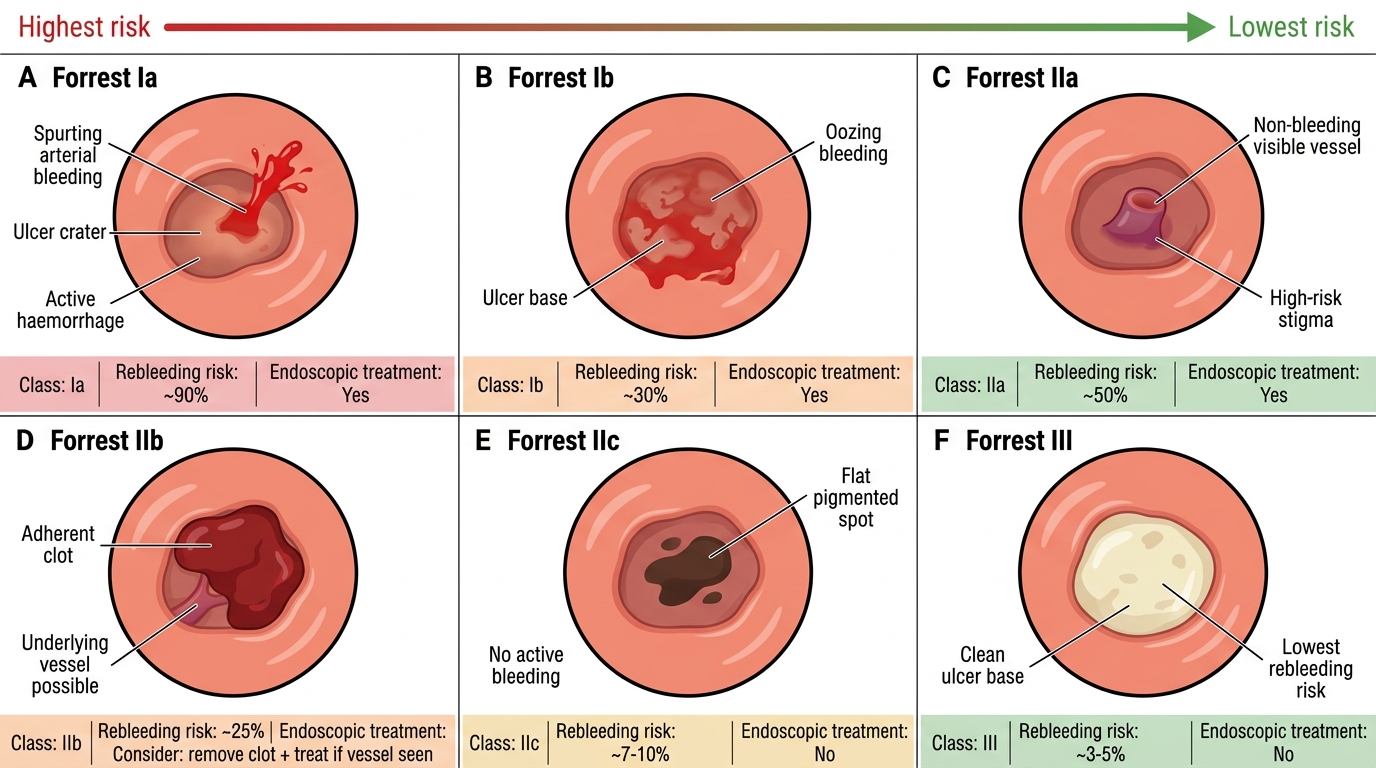
Forrest Classification of Bleeding Peptic Ulcers
Advanced Imaging and the Indications for Endoscopic or Surgical Intervention
When endoscopy fails to identify the bleeding source or bleeding is too rapid and ongoing for safe endoscopy, advanced imaging modalities and surgical intervention become relevant. Understanding their indications, capabilities, and limitations — required by NMC competency IM15.16 — is essential for the physician managing a patient with refractory GI haemorrhage.
CT angiography (CTA): CTA of the abdomen and pelvis (arterial phase, portal phase) is the most important advanced investigation in GI bleeding. It is non-invasive, widely available, and can detect active bleeding at rates as low as 0.3–0.5 mL/minute, with a sensitivity of approximately 85–90% for active haemorrhage. CTA is indicated when: (1) endoscopy has failed to identify the source (negative OGD with ongoing UGIB, colonoscopy unavailable or not feasible); (2) bleeding is from an unclassified small bowel source (between the duodenum and terminal ileum — a 'dark zone' inaccessible to standard endoscopy); (3) arterial haemorrhage is suspected (haemodynamically unstable, rapid haematochezia) and the pre-interventional anatomy needs mapping before angiographic embolisation. The CTA finding of active contrast extravasation ('blush') directly guides subsequent therapeutic angiography.
Mesenteric angiography (catheter angiography): When active bleeding is confirmed on CTA (or when the patient is haemodynamically unstable and directly taken to the interventional suite), selective mesenteric angiography allows both diagnosis (localisation of the bleeding vessel) and treatment via transcatheter arterial embolisation (TAE). TAE is the preferred non-surgical haemostatic treatment for diverticular bleeding, angiodysplasia, Dieulafoy lesion, and recurrent peptic ulcer bleeding after endoscopic failure. It requires active bleeding at a rate of at least 0.5–1 mL/minute to be diagnostic. Complications include bowel ischaemia from distal embolisation (particularly in the colon, where collateral circulation is less robust).
Nuclear medicine scintigraphy (labelled red cell scan): Technetium-99m labelled red blood cell scintigraphy can detect bleeding at rates as low as 0.1–0.4 mL/minute — more sensitive than angiography — and can detect intermittent or slow bleeding over a 24-hour scanning window. However, it only localises bleeding to a general region (right colon, left colon, small bowel) rather than the specific vessel, and its spatial resolution is insufficient for therapeutic guidance. It is most useful as a first step to confirm active bleeding before committing to angiography when the clinical picture is ambiguous.
Capsule endoscopy and deep enteroscopy (push or balloon-assisted): For obscure GI bleeding — defined as bleeding of unknown origin after negative OGD and colonoscopy — capsule endoscopy (a swallowed capsule containing a miniature camera) is the investigation of choice and identifies the source in approximately 50–60% of cases. It is particularly effective for identifying small bowel angiodysplasia, Meckel's diverticulum (using a Meckel's diverticulum technetium scan in addition), Crohn's disease, small bowel tumours, and NSAID-induced enteropathy. Push enteroscopy or device-assisted enteroscopy (single-balloon or double-balloon enteroscopy) allows direct visualisation and therapy of lesions in the proximal and mid-small bowel identified by capsule endoscopy.
Indications for surgical intervention in GI bleeding: Surgery is now the last resort for GI bleeding given the efficacy of endoscopic and angiographic haemostasis. Surgery is indicated when: (1) haemorrhage is not controlled after two attempts at endoscopic haemostasis (endoscopic failure); (2) the haemorrhagic rate requires transfusion of >6 units packed red cells within 24 hours despite endoscopic or radiological haemostasis attempts; (3) a surgical emergency exists independently of haemostasis (perforated viscus, aortoenteric fistula — immediate surgery is the definitive treatment); (4) the source is not accessible to endoscopy or angiography (rare anatomical variants, inaccessible bleeding loop). For variceal bleeding refractory to medical and endoscopic treatment, transjugular intrahepatic portosystemic shunt (TIPS) is the salvage procedure — it reduces portal pressure by creating a shunt between the portal and hepatic veins within the liver and achieves haemostasis in 90–95% of cases, though it can precipitate hepatic encephalopathy.
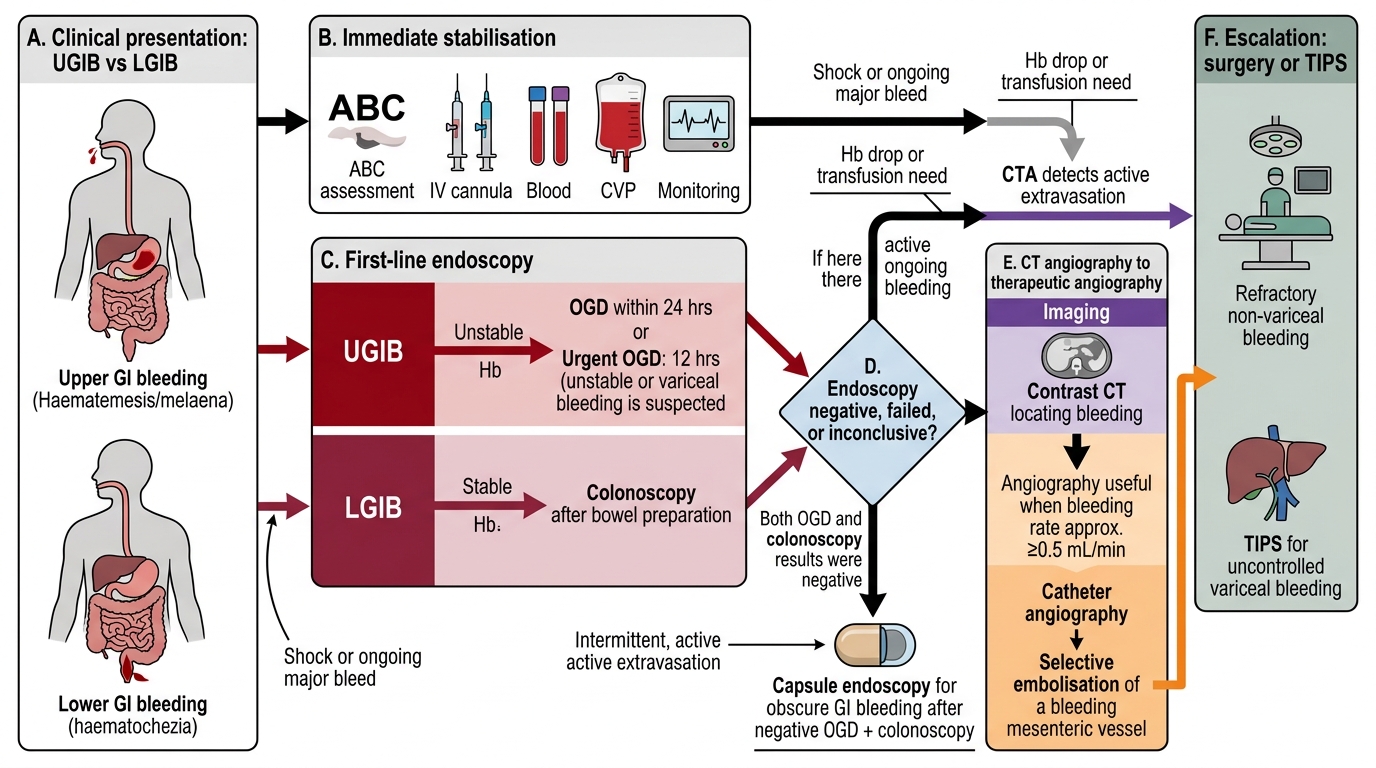
Decision Algorithm for GI Bleeding Investigation and Intervention
SELF-CHECK
A 65-year-old man with haematochezia has undergone upper GI endoscopy (negative for upper source) and colonoscopy (negative for colonic source) over 48 hours. He continues to have intermittent small-volume rectal bleeding over the next week, with haemoglobin dropping from 10.2 to 8.6 g/dL. What is the most appropriate next investigation?
A. Repeat colonoscopy with better bowel preparation
B. Mesenteric angiography — the bleeding is almost certainly arterial and needs embolisation
C. Capsule endoscopy to investigate the small bowel as the probable source
D. Surgical laparotomy to directly inspect the bowel
Reveal Answer
Answer: C. Capsule endoscopy to investigate the small bowel as the probable source
Negative OGD and colonoscopy in a patient with ongoing GI bleeding defines 'obscure GI bleeding.' The small bowel (between the duodenum and terminal ileum) is inaccessible to standard endoscopy. Capsule endoscopy is the recommended first-line investigation for obscure GI bleeding, identifying the source in approximately 50–60% of cases — commonly small bowel angiodysplasia, Crohn's disease, or NSAID enteropathy. Angiography requires active bleeding at ≥0.5–1 mL/min and would not localise intermittent slow bleeding. Laparotomy is reserved for failed endoscopic/angiographic haemostasis or surgical emergencies.
SELF-CHECK
At upper GI endoscopy for UGIB, a gastric ulcer is found with a visible non-bleeding vessel (Forrest class IIa). Which management approach is correct?
A. No endoscopic treatment needed; start oral PPI and discharge
B. Endoscopic haemostasis is recommended (e.g. dual therapy: adrenaline injection + haemoclip or thermal coagulation) followed by high-dose IV PPI infusion
C. Immediate surgical resection — Forrest IIa carries the highest rebleeding risk
D. Observe in hospital for 24 hours without endoscopic treatment; re-endoscope only if rebleeding occurs
Reveal Answer
Answer: B. Endoscopic haemostasis is recommended (e.g. dual therapy: adrenaline injection + haemoclip or thermal coagulation) followed by high-dose IV PPI infusion
Forrest IIa (visible non-bleeding vessel) carries a rebleeding risk of approximately 43% without endoscopic treatment. Endoscopic haemostasis is clearly recommended — dual therapy (adrenaline injection combined with a second modality: haemoclip, thermal coagulation, or fibrin glue) is superior to adrenaline alone. Following successful endoscopic therapy, high-dose IV PPI (80 mg bolus then 8 mg/hour infusion for 72 hours) maintains gastric pH >6, optimising haemostatic conditions and reducing rebleeding risk. Forrest Ia (actively spurting artery) carries the highest rebleeding risk (~55%), not IIa. Surgery is not indicated at this stage.
CLINICAL PEARL
The Rockall Score and the Glasgow-Blatchford Score are complementary, not interchangeable. The Glasgow-Blatchford Score is a pre-endoscopy score designed to identify which patients need intervention and should not be discharged — it relies entirely on clinical and basic laboratory data available at presentation. The Rockall Score requires endoscopy for its full calculation because it incorporates the endoscopic diagnosis and stigmata of recent haemorrhage — it is a post-endoscopy mortality and rebleeding predictor. A common student error is using the Rockall Score to decide whether to do endoscopy — that is precisely the job of the Glasgow-Blatchford Score. Use Blatchford first (should I admit and scope this patient?), then Rockall after endoscopy (what is this patient's ongoing risk?).
Applied Practice: Investigation Case Scenarios
The investigation decisions you make in GI bleeding must be both technically correct (choosing the right test) and sequentially rational (ordering tests in the right order for the right patient at the right time). The following scenarios consolidate your investigative reasoning by requiring you to identify the most appropriate next investigation at each clinical branch point — a skill directly tested in NMC IM15.9 and IM15.10 at the KH/SH level. Apply the five governing principles and the three-tier investigation ladder to each case before reading the analysis. For each case, explicitly identify which risk score applies, what tier of investigation is most appropriate at this clinical moment, and what false-negative trap (if any) needs to be anticipated in the investigation plan.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
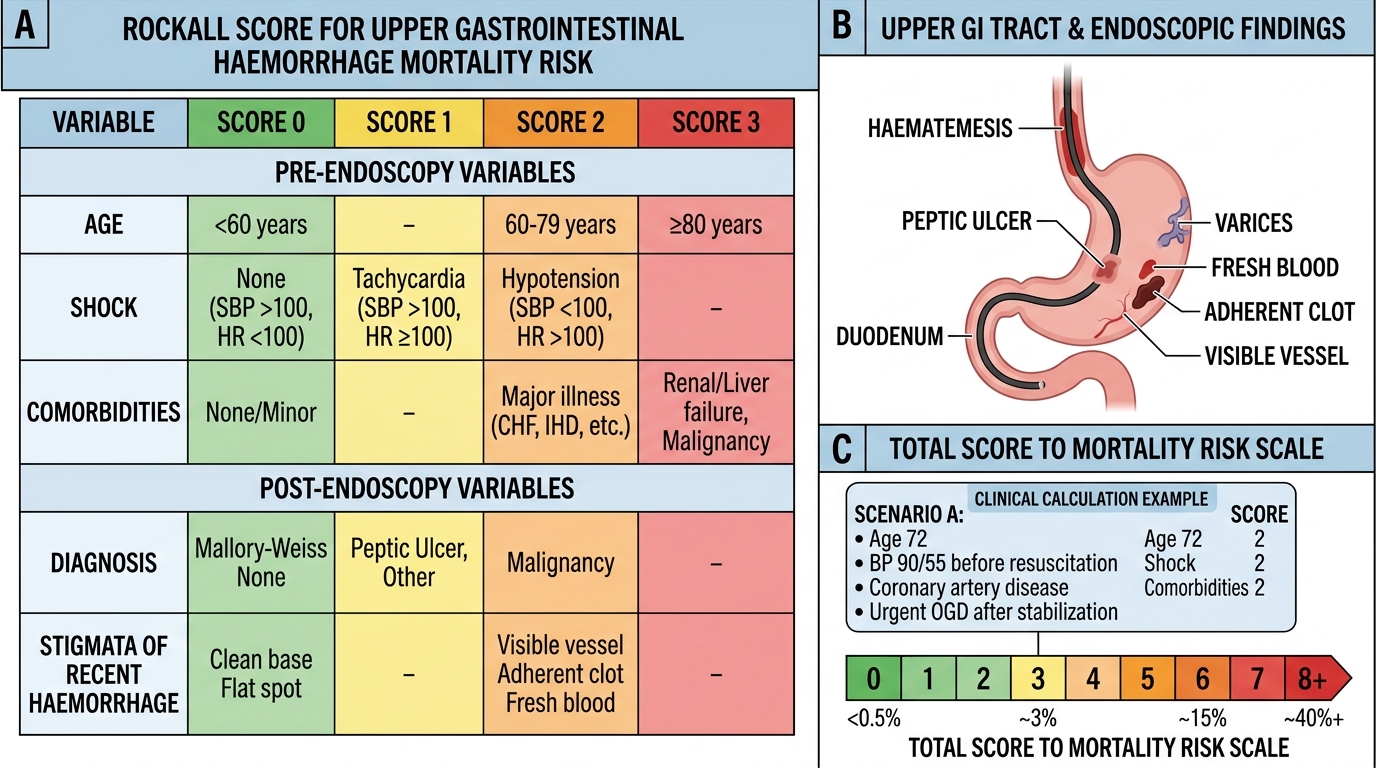
Rockall Score for Upper GI Bleeding
Scenario A: A 72-year-old man with hypertension and type 2 diabetes presents with sudden onset haematemesis (approximately 400 mL fresh blood). BP is 90/55 mmHg on arrival. He is resuscitated to BP 108/70 and pulse 96 within 30 minutes. He is on aspirin and clopidogrel for coronary artery disease. CBC returns: Hb 7.4 g/dL, platelets 142 × 10⁹/L; PT/INR 1.3. What investigations are indicated, and what is the next priority?
Analysis: He is now haemodynamically stabilised. First-line bloods drawn: FBC, coagulation, U&E (note BUN:creatinine ratio to confirm upper source), LFTs, blood group and crossmatch, H. pylori stool antigen test for later. With Hb 7.4 and cardiovascular disease (coronary artery disease), transfusion threshold is Hb <8 g/dL — so packed red cells should be ordered. INR 1.3 does not require FFP. Next priority: urgent OGD within 24 hours (Glasgow-Blatchford score likely ≥6 given haematemesis, hypotension on arrival, Hb 7.4, aspirin-clopidogrel use). Pre-OGD erythromycin 250 mg IV 30 min before to clear stomach. Given dual antiplatelet use, aspirin and clopidogrel should be held during acute management, restarted after haemostasis discussion with cardiology.
Scenario B: A 55-year-old woman with Child-Pugh B cirrhosis from hepatitis C presents with haematemesis. After initial resuscitation, OGD reveals grade 3 oesophageal varices with active oozing. Band ligation is performed on 4 varices with cessation of bleeding. Post-endoscopy, she remains stable. What further investigations are required, and what are the indications for re-intervention?
Analysis: Post-procedure: IV ceftriaxone 1 g/day for 7 days (prophylactic antibiotics reduce variceal rebleeding and infections — a key evidence-based intervention in cirrhotic variceal bleeding); continue terlipressin or octreotide for 3–5 days; calculate full Rockall Score (now includes endoscopic diagnosis: variceal bleed — higher score). Labs: LFTs + albumin + bilirubin + INR daily (Child-Pugh and MELD monitoring). Platelet count — target >50 × 10⁹/L during acute phase. Indications for re-intervention: rebleeding (fresh haematemesis or haemodynamic deterioration suggesting rebleed), defined as transfusion requirement >2 units after initial haemostasis — this triggers repeat OGD (second endoscopic attempt); failure of second endoscopy = TIPS referral (salvage therapy).
Self-Assessment: Consolidating Investigation Competencies
Having worked through the governing principles of investigation, the first-line laboratory panel with its correct interpretation and limitations, endoscopy indications and risk stratification with Glasgow-Blatchford and Rockall scores, and advanced imaging with its decision thresholds, you are now positioned to self-assess your mastery of the NMC IM15.9, IM15.10, and IM15.16 competencies. The self-assessment below covers the four key knowledge domains that will be tested in examinations and clinical practice. Before reviewing each domain, answer the question mentally and check your reasoning against the evidence base you have studied in this module.
Domain 1 — Laboratory test interpretation: Can you state the specific clinical action triggered by each of the following results in a GI bleed patient: Hb 6.8 g/dL (no CVD); INR 1.9; BUN:creatinine ratio 35:1; MCV 72 fL with positive faecal immunochemical test; CLO test negative in a patient on pantoprazole? For each result, identify the clinical action and any required follow-up test. Domain 2 — Endoscopy indications: What is the correct timing of OGD for a Glasgow-Blatchford Score of 8 in a haemodynamically stable patient? What is the indication for pre-OGD erythromycin? What Forrest class mandates endoscopic haemostasis with dual therapy? Domain 3 — Advanced imaging: When is CT angiography indicated over colonoscopy in lower GI bleeding? What is the minimum bleeding rate detectable by CT angiography versus nuclear medicine scintigraphy? Domain 4 — Escalation decisions: After two failed attempts at endoscopic haemostasis for oesophageal varices, what is the next intervention? What transfusion volume threshold triggers surgical consultation? Reviewing your answers against the framework in this module will reveal any specific knowledge gaps to address before clinical assessment.
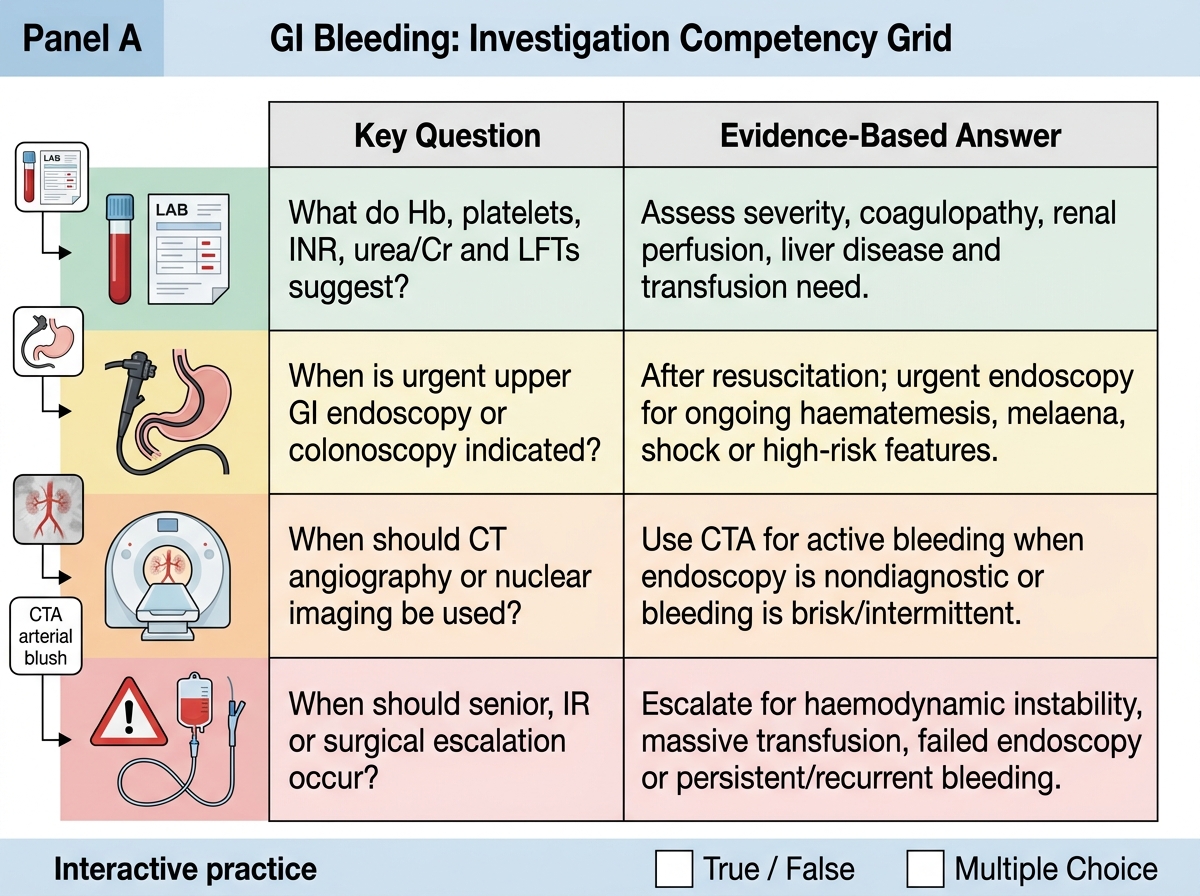
GI Bleeding Investigation Competency Grid