Page 13 of 19
IM15.{11-15,17-18} | GI Bleeding Treatment and Transfusion — SDL Guide (Part 3)
Specialist Consultation, Patient Counselling, and Treatment Plan Documentation
Effective management of GI bleeding extends beyond pharmacotherapy and blood products to encompass two equally important competencies: knowing when to involve specialist teams (IM15.17) and communicating clearly and compassionately with the patient and their family (IM15.18). Both are NMC SH/K-level requirements and both are demonstrably impactful on patient outcomes. The general medicine physician is the coordinator of the GI bleed patient's care — the person who recognises the need for specialist involvement, communicates clearly in the referral, and ensures that the family understand what is happening to their relative in real time. This coordination role is inseparable from the clinical management role; a technically correct resuscitation and pharmacotherapy plan that is not accompanied by appropriate specialist involvement and clear patient communication is incomplete care.
Specialist consultation triggers: The general medicine physician manages the initial resuscitation and risk stratification of GI bleeding and coordinates specialist involvement. The trigger for each consultation is based on the clinical and haemodynamic status:
- Gastroenterology: All patients with UGIB require gastroenterology input for endoscopic management. Urgent gastroenterology consultation (within 6–12 hours or immediately out-of-hours) is required when: Glasgow-Blatchford Score ≥6; haemodynamic instability despite initial resuscitation; suspected variceal bleeding; active haematemesis or melaena with haemodynamic compromise. Non-urgent consultation (within 24 hours) is appropriate for stable, low-risk UGIB (Blatchford 0–1 can be managed outpatient).
- Surgery: Surgical consultation is required when endoscopic haemostasis has failed twice, ongoing haemorrhage requires >6 units of blood in 24 hours despite attempted haemostasis, or a surgical emergency exists (perforation, aortoenteric fistula, visceral artery aneurysm rupture). Early surgical discussion — even before the second endoscopy — is good practice so that the surgical team is prepared.
- Interventional radiology: Consulted when active bleeding is confirmed on CT angiography and endoscopic haemostasis has failed or is not feasible. IR performs transcatheter arterial embolisation (TAE) as the preferred non-surgical haemostatic option.
- Hepatology and liver transplant teams: In patients with decompensated cirrhosis and variceal bleeding, early hepatology involvement is essential. TIPS (transjugular intrahepatic portosystemic shunt) is a salvage option when dual endoscopic and pharmacological therapy fails — TIPS reduces rebleeding rates but requires liver transplant team assessment. A Child-Pugh score and MELD score should be calculated and communicated in the referral.
- ICU team: ICU admission is indicated for patients with haemodynamic instability unresponsive to resuscitation (requiring vasopressors), respiratory failure (aspiration, ARDS), altered consciousness (hepatic encephalopathy, hypoxic confusion), massive transfusion requiring invasive monitoring, and high-risk endoscopic findings requiring close monitoring after haemostasis.
- Haematology: For patients with complex coagulopathy (DIC, factor deficiency, haemophilia presenting with GI bleeding), patients on novel anticoagulants (DOACs) requiring reversal agents (idarucizumab for dabigatran, andexanet alfa for factor Xa inhibitors), or massive transfusion requiring protocol-based blood product ordering.
Patient and family counselling (IM15.18): Counselling a patient and family in the setting of acute GI bleeding requires the physician to simultaneously convey urgency, maintain calm, and provide honest, empathetic communication about diagnosis and treatment. The key elements of counselling in this context are:
Explanation of the diagnosis: Use lay language — 'You have bleeding from inside the stomach/gut (or 'from blood vessels in the food pipe caused by liver disease'). We have started treatments to stop the bleeding and stabilise you.' Avoid jargon without explanation. For variceal bleeding in a cirrhotic patient, this is an opportunity to gently but honestly address the underlying liver disease and its implications.
Explanation of investigations and procedures: 'We are going to pass a thin flexible camera down your throat into your stomach — this is called an endoscopy — to find where the bleeding is coming from and to stop it during the same procedure.' Address the patient's anxiety about endoscopy (sedation will be given; the procedure takes approximately 15–20 minutes; there will be some discomfort but it should not be painful).
Explanation of blood transfusion: Many patients and families have concerns about blood transfusion — about religious objections (Jehovah's Witnesses), fear of infection (outdated concerns), or the need for consent. Address these directly and empathetically: 'The blood has been carefully tested and crossmatched specifically for you. Transfusion is needed to restore the oxygen-carrying capacity of your blood while we stop the bleeding. Without it, there is a significant risk of organ damage from anaemia.'
Prognosis and plan: Set realistic expectations about recovery. Acknowledge that further procedures may be needed. If the patient has decompensated liver disease, the conversation must honestly address the severity of the underlying condition and the need for long-term follow-up.
Non-judgemental approach: NMC competency IM15.18 specifically requires communication 'in an empathetic non-judgemental manner.' This is especially important in patients whose GI bleeding is related to alcohol use disorder — the clinical setting is not the moment for lectures about alcohol cessation; instead, acknowledge the patient's distress, ensure they feel respected and supported, and plan alcohol cessation counselling and CAGE/AUDIT screening as a post-discharge intervention when the patient is stable and receptive.
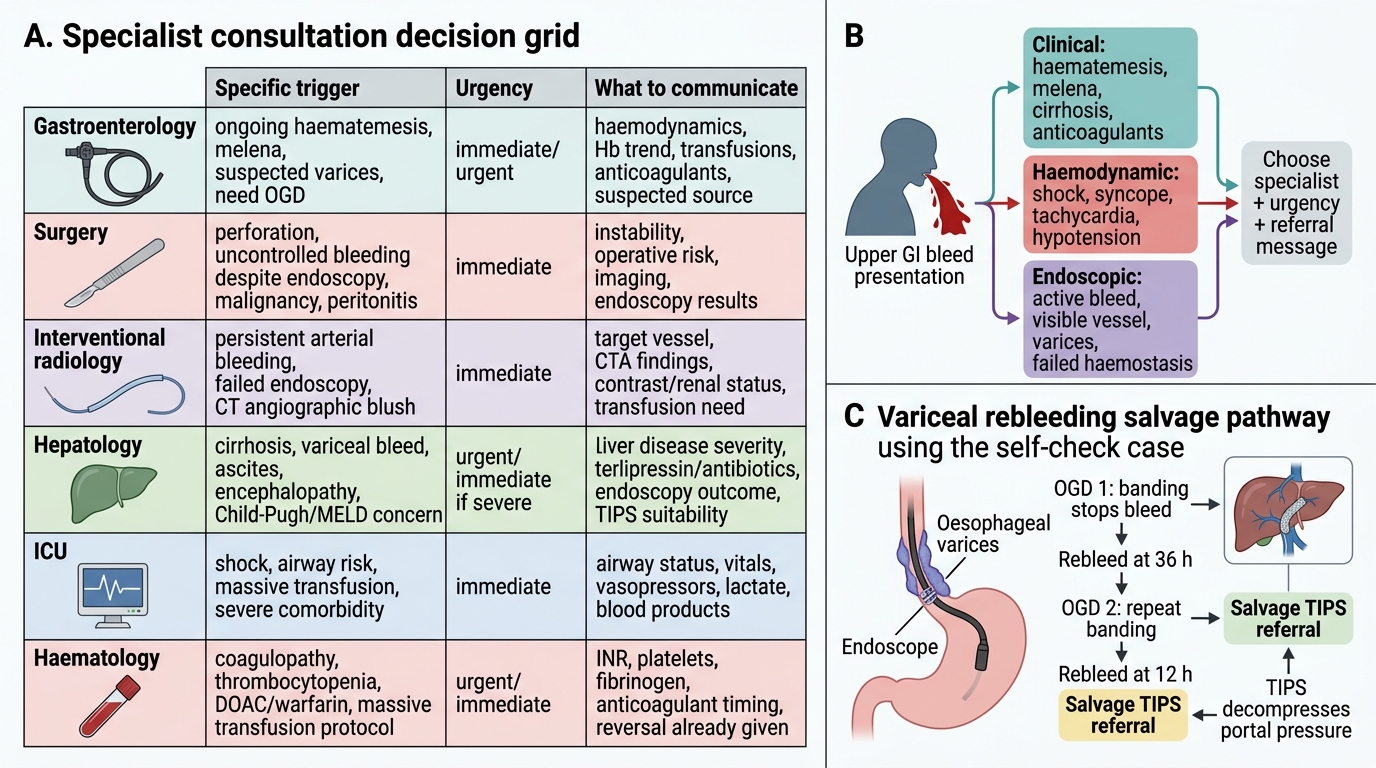
GI Bleeding Specialist Consultation Decision Grid
SELF-CHECK
A 48-year-old man with alcoholic cirrhosis presents with haematemesis. He is given terlipressin and IV ceftriaxone. OGD the next morning shows active oesophageal variceal bleeding; two bands are placed with cessation of bleeding. He rebleeds 36 hours later with a fresh episode of haematemesis. Repeat OGD is performed and further band ligation achieves haemostasis. He rebleeds again 12 hours later. What is the most appropriate next intervention?
A. A third OGD with further band ligation
B. Transjugular intrahepatic portosystemic shunt (TIPS) referral as salvage therapy
C. Increase terlipressin dose to 4 mg every 4 hours
D. Oral propranolol to reduce portal pressure
Reveal Answer
Answer: B. Transjugular intrahepatic portosystemic shunt (TIPS) referral as salvage therapy
After two failed attempts at endoscopic haemostasis for variceal bleeding (two OGD procedures with band ligation, both complicated by rebleeding), the patient qualifies for TIPS as salvage therapy. TIPS creates an intrahepatic portosystemic shunt to decompress portal pressure, achieving haemostasis in approximately 90–95% of cases refractory to endoscopic treatment. A third OGD is not indicated after two failures — the guidelines define two endoscopic failures as the trigger for salvage. Increasing terlipressin dose does not have evidence for additional efficacy after endoscopic failure. Oral propranolol is a secondary prophylactic agent that takes days to weeks to achieve portal pressure reduction and is entirely inappropriate in an acute rebleeding situation.
CLINICAL PEARL
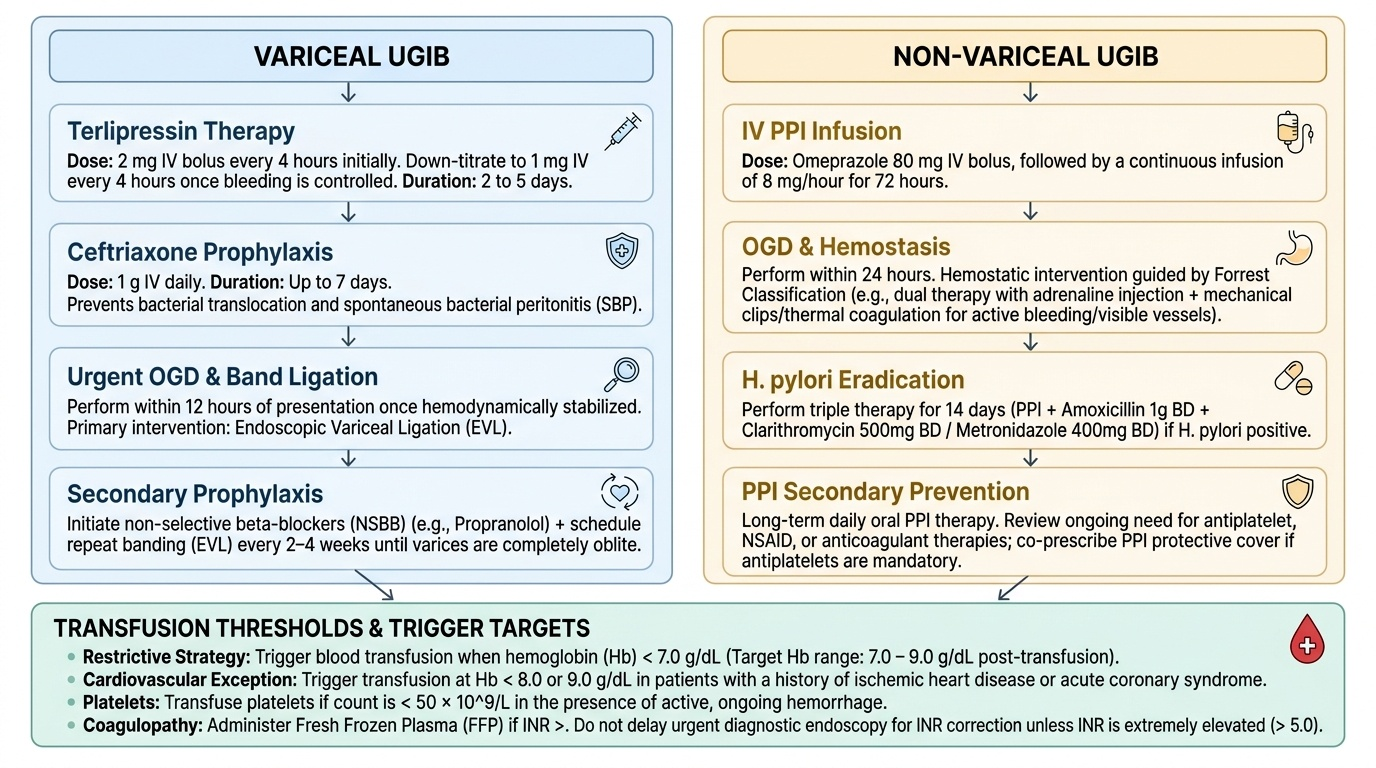
The pharmacological bundle for variceal bleeding has four components, all supported by Level 1A evidence and all contributing independently to mortality reduction: (1) vasoactive drug (terlipressin — start immediately on clinical suspicion, before endoscopy); (2) antibiotic prophylaxis (IV ceftriaxone 1 g/day for 7 days — reduces bacterial infection, rebleeding, and mortality); (3) endoscopic band ligation (performed at the first haemodynamically stable OGD within 12 hours); and (4) secondary prophylaxis post-discharge (non-selective beta-blocker — propranolol or carvedilol — to reduce portal pressure and prevent recurrence, combined with repeat banding at 2–4 weekly intervals until variceal eradication). Omitting any of these four elements increases mortality. The most commonly omitted is antibiotic prophylaxis — prescribe it reflexively in every cirrhotic patient presenting with GI bleeding.
Self-Assessment: Integrated Treatment Planning
The treatment of GI bleeding integrates resuscitation, blood product decisions, disease-specific pharmacotherapy, escalation judgements, and patient communication into a coherent clinical plan that must be constructed under time pressure. The following scenarios test your ability to generate this integrated plan, as required by NMC competency IM15.11 at the KH level — 'develop, document, and present a treatment plan.' For each scenario, work through the pathophysiological treatment rationale (why each drug or blood product), the specific dose and duration of each pharmacological intervention, and the specialist escalation trigger before reading the model answer. The scenarios are deliberately chosen to represent the two most common and most deadly presentations of acute UGIB — variceal haemorrhage in cirrhosis and peptic ulcer bleeding with antiplatelet use — because these two presentations account for the majority of preventable mortality in acute GI bleeding and represent the highest-yield examination and clinical scenarios for final-year MBBS.
Provided image
Scenario A: A 44-year-old man with hepatitis B cirrhosis (Child-Pugh B) presents with 500 mL haematemesis. BP 88/55 mmHg, pulse 120 bpm. Hb 7.2 g/dL, INR 1.9, platelets 52 × 10⁹/L. No prior variceal banding. Write a complete treatment plan documenting all immediate interventions in priority order.
Integrated treatment plan:
1. Airway: Assess — patient communicating but anxious; lateral positioning and oxygen 6 L/min via face mask.
2. Circulation: Two 14G IV cannulae. Blood draw: FBC, LFTs, coags, crossmatch 6 units. Start normal saline 500 mL IV stat.
3. Blood products: Hb 7.2 + haemodynamic instability → transfuse PRBCs (crossmatched; if uncrossmatched O-negative emergency). INR 1.9 and liver disease → FFP 4 units IV. Platelets 52 × 10⁹/L with active bleeding → 1 pool platelets IV.
4. Vasoactive therapy: IV terlipressin 2 mg every 4 hours (portal pressure reduction — start immediately).
5. Antibiotic prophylaxis: IV ceftriaxone 1 g stat and daily for 7 days.
6. Monitoring: Urinary catheter. Hourly urine output, vitals every 30 min. Target MAP ≥65 mmHg, UO ≥0.5 mL/kg/hour.
7. Endoscopy: Contact gastroenterology — urgent OGD as soon as haemodynamically stabilised (target within 12 hours).
8. Specialist consultation: Hepatology for Child-Pugh B assessment and TIPS contingency planning.
9. ICU review: Refer given active haemodynamic instability and high-risk variceal bleeding.
10. Documentation: Inform patient and family of diagnosis, planned endoscopy, need for transfusion; obtain verbal consent for OGD.
Scenario B: A 58-year-old man on NSAID therapy for osteoarthritis is diagnosed with a Forrest IIa posterior duodenal ulcer at OGD. Endoscopic haemostasis with adrenaline injection and haemoclip applied. H. pylori CLO test is indeterminate (patient was on rabeprazole for 3 weeks pre-admission). Design the post-endoscopy pharmacological plan and H. pylori management strategy.
Post-endoscopy plan: (1) IV pantoprazole 80 mg bolus then 8 mg/hour infusion for 72 hours post-endoscopy (maintains pH >6, reduces rebleed risk for Forrest IIa). (2) Stop NSAID (ibuprofen/naproxen) permanently — the ulcer aetiology is NSAID use; if analgesia is required, switch to paracetamol or, if anti-inflammatory is essential, use celecoxib (COX-2 selective) with a PPI gastroprotectant. (3) After 72-hour IV PPI, switch to oral rabeprazole 20 mg twice daily for 4–8 weeks (ulcer healing). (4) H. pylori management: CLO test indeterminate because of prior PPI — arrange urea breath test or stool antigen test at 4-week follow-up after 2-week PPI washout (if feasible) or at 4 weeks post-eradication to confirm. If positive: standard 14-day triple therapy (PPI twice daily + clarithromycin 500 mg BD + amoxicillin 1 g BD). (5) Confirm eradication 4 weeks after completing eradication therapy, 2 weeks off PPI, using UBT or stool antigen. (6) Long-term: if NSAID is truly necessary for musculoskeletal pain, use lowest effective dose of COX-2 inhibitor + PPI; H. pylori eradication alone reduces but does not eliminate NSAID ulcer recurrence risk.