Page 2 of 19
IM16.{1-3,6,15} | Diarrheal Disorder Foundations — SDL Guide (Part 2)
Chronic Effects of Diarrhoea and Malabsorption
When diarrhoea persists for weeks to months, the systemic consequences extend far beyond acute dehydration and electrolyte imbalance to encompass progressive nutritional deficiency, wasting, and multi-system organ impairment. Understanding these chronic effects is essential for the final-year student because the patient with chronic diarrhoea presenting to the outpatient clinic may have spent months accumulating deficiencies that are not immediately visible and will not be reversed by treating diarrhoea alone — targeted nutritional rehabilitation is always required in parallel. The spectrum of chronic deficiency depends critically on which segment of the intestine is diseased: disease of the proximal small bowel primarily disrupts iron, folate, and fat-soluble vitamin absorption; disease of the terminal ileum specifically impairs vitamin B12 absorption; pancreatic exocrine insufficiency impairs fat digestion; and colonic disease produces predominantly inflammatory losses. This anatomical localisation principle allows the clinician to predict deficiency patterns before a full biochemical panel is available.
Macronutrient consequences:
In fat malabsorption (steatorrhoea), the patient loses not only fat calories but also the fat-soluble vitamins dissolved in the unabsorbed fat. The resulting fat-soluble vitamin deficiencies are clinically important:
- Vitamin A deficiency: night blindness → xerophthalmia → corneal ulceration/keratomalacia (a preventable cause of blindness in malnourished children with chronic diarrhoea in India)
- Vitamin D deficiency: osteomalacia (bone pain, proximal myopathy, looser zones on X-ray), rickets in children
- Vitamin K deficiency: coagulopathy (prolonged PT/INR); presents as easy bruising or bleeding gums
- Vitamin E deficiency: spinocerebellar ataxia, peripheral neuropathy (rare, seen in prolonged severe malabsorption)
Protein malabsorption leads to hypoalbuminaemia, which reduces the plasma oncotic pressure and causes oedema — particularly dependent oedema and, in severe cases, ascites. In children, this contributes to the spectrum of protein-energy malnutrition (PEM) — with kwashiorkor (oedematous malnutrition) having a recognisable connection to chronic gut disease in resource-poor settings.
Micronutrient consequences:
- Iron deficiency anaemia: chronic blood loss (inflammatory diarrhoea/IBD) + impaired absorption (duodenal and proximal jejunal mucosal damage in coeliac, tropical sprue)
- Vitamin B12 deficiency: ileal disease (Crohn's ileitis, tropical sprue, giardiasis interfering with absorption) → megaloblastic anaemia, subacute combined degeneration of the cord (posterior column + lateral corticospinal tract)
- Folate deficiency: jejunal malabsorption (coeliac, tropical sprue) → megaloblastic anaemia; also caused by methotrexate (used in IBD), sulfasalazine
- Zinc deficiency: impaired immunity, poor wound healing, acrodermatitis enteropathica (perioral/perianal rash), growth retardation in children
- Calcium and magnesium deficiency: neuromuscular excitability (cramps, Chvostek sign, Trousseau sign), osteoporosis (long-term)
Fluid and electrolyte consequences of chronic diarrhoea:
Chronic fluid loss leads to a state of persistent volume depletion with secondary hyperaldosteronism — the kidney retains sodium at the cost of wasting potassium, producing hypokalaemia even in the absence of acute losses. Chronic metabolic acidosis from persistent bicarbonate loss in stool can impair normal growth and bone mineralisation in children.
Malabsorption — the D4 triad: A classic teaching mnemonic for malabsorption covers the four hallmark presentations: Diarrhoea (steatorrhoea — fatty, floating, pale stools), Deficiency (multi-nutrient deficiencies as above), Distension (gaseous bloating from fermentation of unabsorbed carbohydrates), and Wasting/Dermatological signs (glossitis, angular stomatitis from B-vitamin deficiency; perianal rash from zinc; Casal's necklace in pellagra from niacin deficiency).
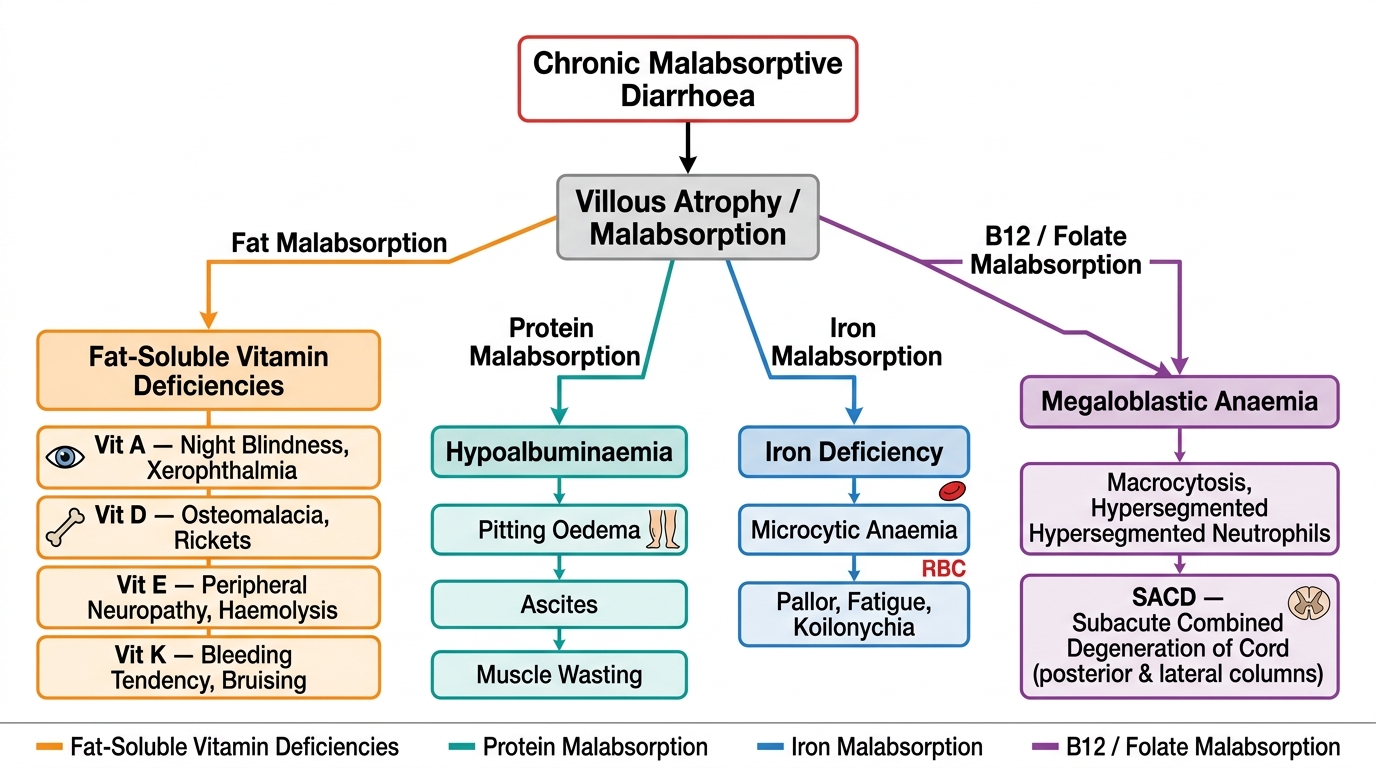
Consequences of Chronic Malabsorptive Diarrhoea: Deficiency Pathways and Clinical Signs
Diarrhoea vs Dysentery: Clinical Distinction and IBD Patterns
The distinction between diarrhoea and dysentery is not merely semantic — it carries immediate management implications. A student who fuses these two presentations and applies the same treatment algorithm risks providing antibiotics when none are indicated, withholding antibiotics when they are urgently needed, or administering contraindicated antimotility agents to a patient with invasive colitis. Understanding the Crohn's vs ulcerative colitis distinction (IM16.15) similarly has management weight, since the choice of medical therapy, the role of surgery, and the surveillance strategy differ substantially between the two. In the community and district hospital settings where final-year students train most extensively in India, the failure to make this distinction promptly is one of the commonest sources of avoidable therapeutic errors — both the inappropriate use of antibiotics for viral gastroenteritis and the dangerous use of antimotility agents for bloody dysentery. Making the distinction correctly from history and physical examination, before microbiological results are available, is therefore a core clinical skill at this level of training.
Diarrhoea vs Dysentery — distinguishing clinical features:
| Feature | Diarrhoea | Dysentery |
|---|---|---|
| Stool appearance | Watery, loose, unformed | Bloody, mucoid, purulent |
| Blood/pus | Absent | Present (defining feature) |
| Fever | Variable (absent in cholera) | Usually present |
| Abdominal pain | Often absent or mild | Prominent crampy pain |
| Tenesmus | Absent | Common |
| Stool volume | Often large | Small frequent stools (passage of mucus/blood) |
| Faecal leucocytes | Absent | Present (marker of mucosal invasion) |
| Mechanism | Secretory, osmotic, or toxin-mediated | Inflammatory/invasive |
| Causative pathogens (infective) | Cholera, ETEC, rotavirus, norovirus | Shigella, EIEC, Campylobacter, E. histolytica |
| Antimotility agents | Safe if no invasion | CONTRAINDICATED — may worsen invasive disease |
A critical safety point: loperamide and other antimotility agents are contraindicated in dysentery (bloody stools, fever, suspected invasive infection) because slowing intestinal transit prolongs mucosal contact with invasive organisms and toxins, increasing the risk of toxic megacolon and bacteraemia.
Inflammatory Bowel Disease: Crohn's Disease vs Ulcerative Colitis (IM16.15)
Both Crohn's disease (CD) and ulcerative colitis (UC) are chronic, relapsing-remitting inflammatory bowel diseases of uncertain aetiology (immune dysregulation against commensal gut bacteria in genetically susceptible individuals), but they are pathologically and clinically distinct entities:
Distribution and depth of inflammation:
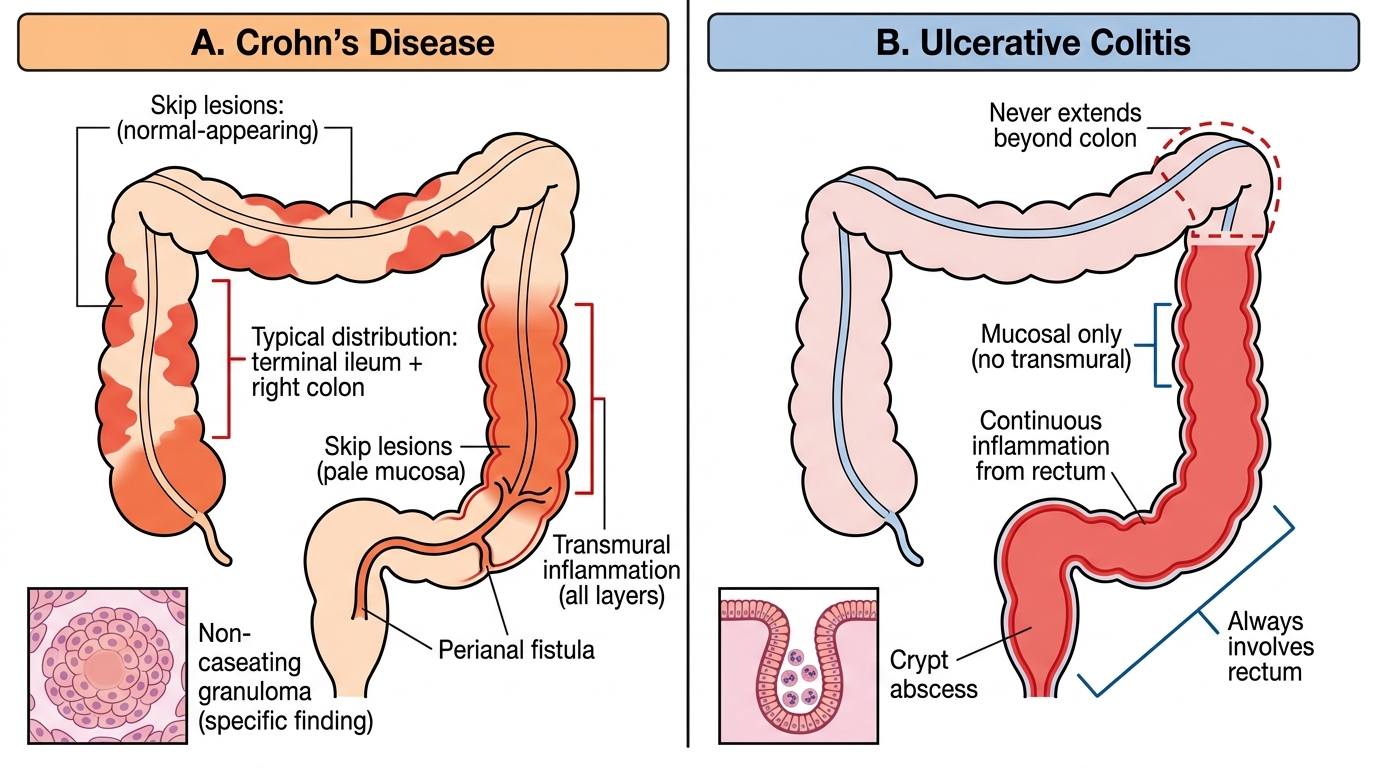
- CD: can involve any segment of the GI tract from mouth to anus; classically affects the terminal ileum and right colon; inflammation is transmural (full-thickness, all layers of the bowel wall); characteristically skip lesions (discontinuous involvement alternating with normal mucosa)
- UC: restricted to the colon and rectum only; invariably starts in the rectum and extends proximally in a continuous, uninterrupted fashion (no skip lesions); inflammation is mucosal and submucosal only (superficial, not transmural)
Histopathology:
- CD: transmural inflammation; non-caseating granulomas (present in 60% — pathognomonic when found); fissuring ulcers; Cobblestone appearance endoscopically
- UC: mucosal ulceration; crypt abscesses (collections of neutrophils within crypts — hallmark); goblet cell depletion; pseudopolyps (islands of residual inflamed mucosa between ulcers)
Clinical features:
- CD: right lower quadrant pain (terminal ileitis mimicking appendicitis), malabsorption and weight loss (small bowel involvement), perianal disease (fistulae, tags, abscesses — up to 30%), fistulae (enteroenteric, enterovesical, enterocutaneous), anaemia of chronic disease + B12 deficiency (ileal disease)
- UC: rectal bleeding (hallmark), tenesmus, urgency, bloody diarrhoea; disease confined to colon; extra-intestinal manifestations include primary sclerosing cholangitis (more common in UC than CD), uveitis, pyoderma gangrenosum, erythema nodosum
Extra-intestinal manifestations (shared): arthritis (peripheral > axial), uveitis/episcleritis, skin lesions (erythema nodosum, pyoderma gangrenosum), hepatobiliary disease (PSC strongly associated with UC)
Crohn's Disease vs Ulcerative Colitis: Distinguishing Features
SELF-CHECK
A 32-year-old man has had intermittent right lower quadrant pain, non-bloody loose stools, and weight loss of 8 kg over 12 months. He has two anal fistulae. Colonoscopy shows deep ulcers and normal-appearing mucosa alternating in the terminal ileum and right colon. Biopsy shows transmural inflammation and non-caseating granulomas. Which diagnosis BEST fits this picture, and what is the ONE most specific histological finding?
A. Ulcerative colitis; crypt abscesses
B. Ulcerative colitis; goblet cell depletion
C. Crohn's disease; non-caseating granulomas
D. Intestinal tuberculosis; caseating granulomas
Reveal Answer
Answer: C. Crohn's disease; non-caseating granulomas
The constellation of terminal ileitis, skip lesions (alternating ulcers and normal mucosa), transmural inflammation, perianal fistulae, and weight loss with right lower quadrant pain is classic Crohn's disease. Non-caseating granulomas are the most specific histological finding — present in about 60% of biopsies. Ulcerative colitis is restricted to the colon/rectum, produces continuous mucosal-only inflammation, and shows crypt abscesses (not granulomas). Intestinal TB is a critical Indian differential — TB granulomas are caseating (central caseous necrosis), unlike Crohn's which is non-caseating; TB also tends to affect the ileocaecal region, have submucosal fibrosis, and respond to anti-TB therapy.
Overview of Investigations and Management Principles
For this foundational SDL, a brief overview of the investigation and management framework orients the learner to the subsequent cluster SDLs (diarrhea-clinical-evaluation, diarrhea-diagnostics, diarrhea-treatment), which cover these areas in full procedural and pharmacological depth. An integrated mental model — knowing which investigation serves which mechanism and which treatment targets which pathogen — is the scaffold that makes the detailed SDLs clinically coherent rather than a series of isolated facts.
Investigations framework overview:
For acute diarrhoea, the first clinical question is severity of dehydration (WHO Plan A/B/C assessment — history and physical examination, not a laboratory test). Basic blood tests (serum electrolytes, blood urea, creatinine, bicarbonate) quantify the metabolic derangement. Stool examination — direct microscopy, wet preparation, and hanging-drop preparation — provides the most clinically directed first-line diagnostic in resource-limited settings: it can identify E. histolytica trophozoites/cysts, Giardia cysts, Cryptosporidium oocysts, and (critically for cholera control) V. cholerae in hanging-drop demonstrating characteristic darting motility. Stool culture is reserved for selected patients (see diarrhea-diagnostics SDL for indications). CBC showing leucocytosis suggests bacterial invasion; eosinophilia suggests parasitic infection.
For chronic diarrhoea, the investigation algorithm expands substantially: colonoscopy with biopsy (for IBD, microscopic colitis, coeliac diagnosis via duodenal biopsy at the time of upper GI endoscopy), serological tests (anti-tissue transglutaminase IgA and total IgA for coeliac disease), stool fat quantification (72-hour faecal fat collection), hydrogen breath tests (lactase deficiency, SIBO), and imaging (CT enterography for CD small bowel extent).
Management framework overview:
All diarrhoeal disease management begins with rehydration: oral (WHO ORS for Plans A and B) or intravenous (Ringer's Lactate for Plan C). This applies regardless of aetiology. Then aetiology-specific treatment is layered:
- Viral gastroenteritis: supportive only — ORS, continued feeding, no antibiotics
- Cholera: ORS/IV rehydration (primary, life-saving) + single-dose doxycycline 300 mg (or azithromycin in children) to shorten illness and reduce transmission; NOT primary treatment in the sense that rehydration takes absolute precedence
- Shigella/invasive bacterial: ciprofloxacin or azithromycin (resistance patterns guide local choice)
- Amoebiasis: metronidazole 400–800 mg TDS × 5–10 days (tissue amoebiasis) + diloxanide furoate 500 mg TDS × 10 days (luminal agent to eliminate cysts and prevent recurrence/transmission)
- Giardiasis: metronidazole 400 mg TDS × 5–7 days or tinidazole single dose
- IBD: mesalamine (aminosalicylates — UC first-line), corticosteroids (active flare), immunomodulators (azathioprine, 6-mercaptopurine), biologics (anti-TNF: infliximab, adalimumab — moderate-severe disease), and surgery when indicated (colectomy curative in UC; complications-only in CD)
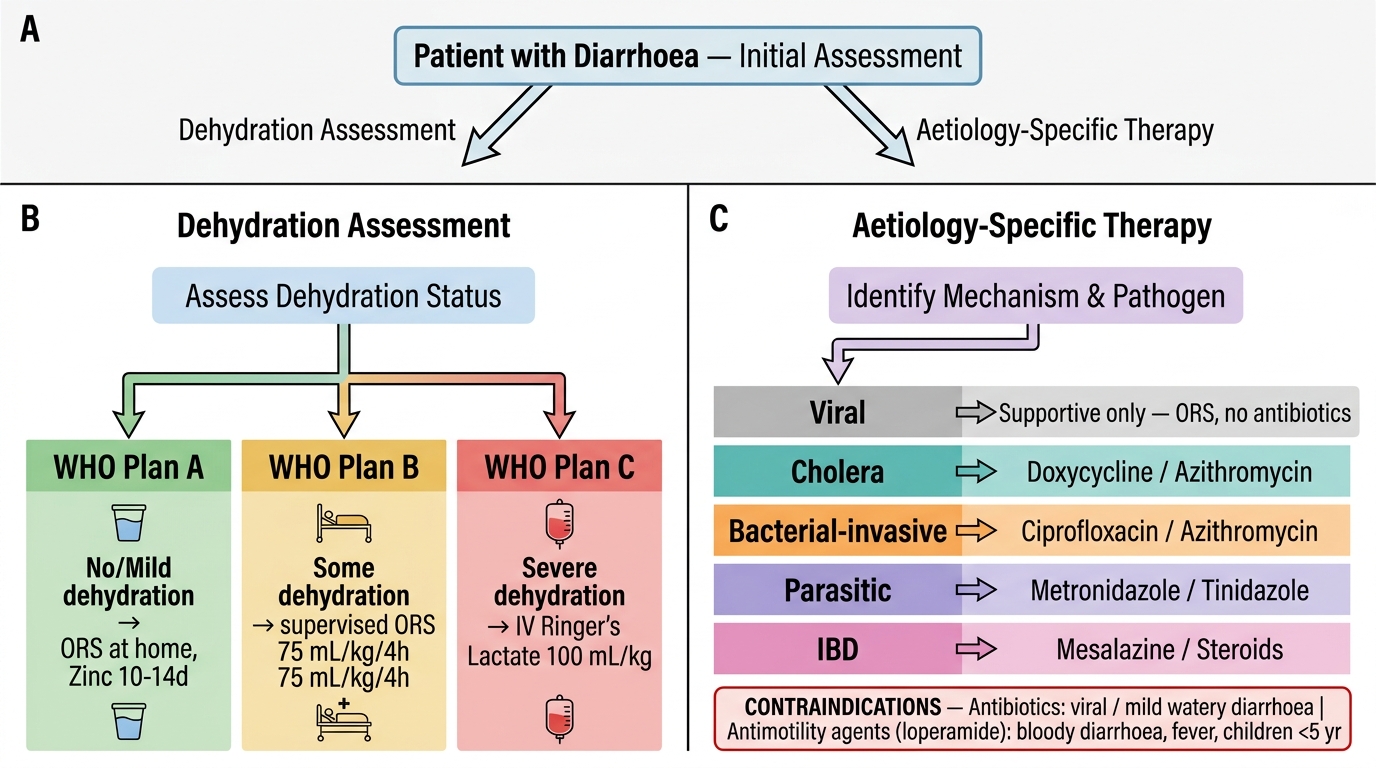
Diarrhoea Management Algorithm: Rehydration & Aetiology-Specific Therapy