Page 13 of 21
IM17.10-14 | Headache Emergency Care and Treatment — SDL Guide
Learning Objectives
- Enumerate the indications for emergency admission and describe immediate supportive care in patients with headache
- Describe the indications, pharmacology, dose, and adverse effects of abortive (acute) therapy in migraine including triptans, NSAIDs, and anti-emetics
- Describe the indications, pharmacology, dose, and adverse effects of prophylactic (preventive) therapy in migraine including propranolol, topiramate, and amitriptyline
- Describe the pharmacology, dose, adverse effects, and regimens for bacterial meningitis (ceftriaxone + dexamethasone), tuberculous meningitis (NTEP 2HRZE + 10HR), and viral/herpes encephalitis (IV acyclovir)
- Counsel patients with migraine and tension-type headache on lifestyle modification, correct use of acute medications, medication-overuse headache prevention, and red flags for emergency attendance
INSTRUCTIONS
This module covers the full treatment spectrum for headache: emergency management, acute migraine pharmacology, preventive migraine therapy, and infective meningitis regimens. The drug doses, indications, and contraindications in this module are high-yield examination content and must be memorised. Pay particular attention to triptan contraindications, the TBM NTEP regimen, and the dexamethasone timing rule for bacterial meningitis.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 17 — Headache and Ch. 140 — Meningitis (textbook)
- API Textbook of Medicine, 10th ed. — Migraine Treatment and CNS Infections (textbook)
- British Association for the Study of Headache (BASH) Guidelines, 4th edition — Acute and Preventive Migraine Therapy (guideline)
- NTEP (National TB Elimination Programme) Technical and Operational Guidelines for TB Control in India, 2019 (updated 2021) — CNS TB regimen (guideline)
- NICE Clinical Guideline CG102: Bacterial Meningitis and Meningococcal Septicaemia (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients arrive in your emergency department on the same afternoon. Deepa, a 32-year-old known migraineur, is brought in by her husband at 3 pm: her migraine attack began 4 hours ago, she has vomited three times, cannot keep any oral medication down, and rates her pain 9/10. She has taken sumatriptan twice in the last month but today cannot swallow anything. Ramesh, a 68-year-old with hypertension and a previous MI, presents with what he describes as a 'typical migraine' but his blood pressure is 170/110 mmHg and his ECG shows ST-T changes — his GP started sumatriptan last month. And in the resus bay, a 26-year-old student is obtunded with meningism, petechial rash, and a fever of 39.8°C — the casualty officer is holding a ceftriaxone vial, asking: 'What dose? IV or IM? Do we need dexamethasone? What about TB cover?' For the clinician who knows the pharmacology, the answers are immediate. For the one who does not, each of these patients pays the price of that ignorance.
WHY THIS MATTERS
Headache treatment spans the full spectrum from outpatient counselling to emergency resuscitation. The NMC competencies IM17.10–IM17.14 address: criteria for emergency admission (IM17.10), pharmacology and dose of abortive migraine therapy (IM17.11), pharmacology and dose of preventive migraine therapy (IM17.12), drug regimens for bacterial, tuberculous, and viral meningitis (IM17.13), and patient counselling for migraine and tension-type headache (IM17.14). These are KH and SH level competencies — you must not only know the drugs and doses but be able to prescribe them in a clinical scenario, justify the choice, and counsel a patient in plain language. In Indian practice, the added complexity of drug availability, cost, and the TB burden makes precise pharmacology knowledge especially important.
RECALL
Activate your relevant pharmacology. Recall that triptans are selective 5-HT₁B/₁D agonists — they cause vasoconstriction of intracranial vessels and inhibit trigeminal nociceptor activation and CGRP release. Recall from your headache foundations that propranolol is a non-selective beta-blocker and topiramate is a sodium/calcium channel blocker and GABA potentiator — both are first-line migraine preventives. From your antimicrobial pharmacology: ceftriaxone (third-generation cephalosporin) crosses the blood-brain barrier and is the backbone of bacterial meningitis treatment; rifampicin (R), isoniazid (H), pyrazinamide (Z), ethambutol (E) are the four drugs of the NTEP/WHO standard TB regimen. From your NTEP knowledge: drug-sensitive TB regimen is 2HRZE + 4HRE for pulmonary TB, extended to 2HRZE + 10–12HR for TBM. Recall that acyclovir (nucleoside analogue) inhibits herpes virus DNA polymerase — it is the drug of choice for herpes simplex encephalitis.
Emergency Headache: Indications for Admission and Immediate Supportive Care
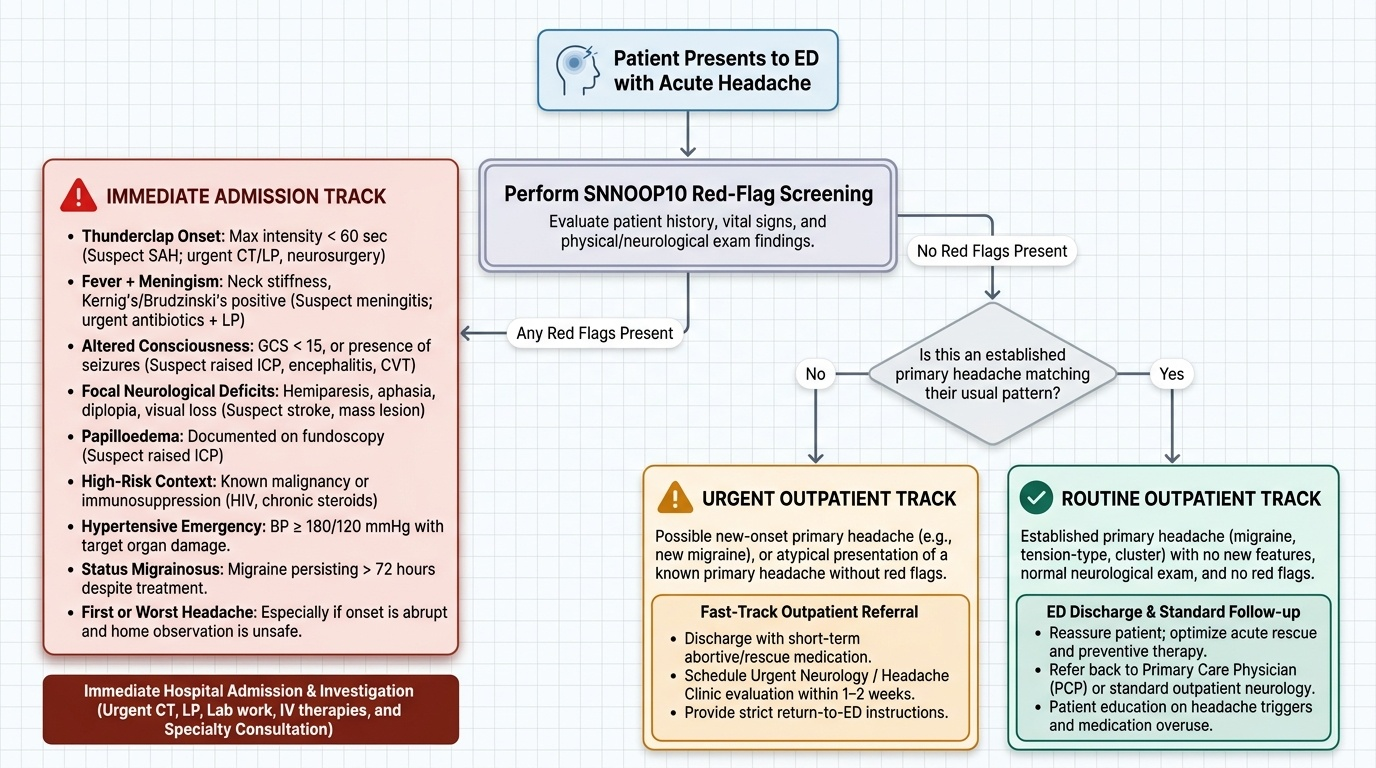
Not every severe headache requires hospital admission, but the clinical skill of identifying which patients require emergency care versus which can be safely managed in outpatient or urgent care settings is among the most consequential clinical decisions in the emergency department. The clinician who admits every severe headache 'to be safe' is not being cautious — they are consuming resources needed for genuinely urgent cases and exposing patients to the risks of hospitalisation without clinical benefit. Equally, the clinician who dismisses a secondary headache as a primary one courts catastrophic missed diagnoses. The ability to rapidly distinguish between these two populations depends on a systematic mental framework of red flags and clinical criteria, not on headache severity alone. The following criteria define the clinical indications for emergency admission and immediate supportive care in headache.
Provided image
Indications for emergency admission (IM17.10) — any of the following mandates immediate hospital admission for investigation and/or treatment:
1. Thunderclap headache (maximum intensity within 60 seconds) — suspected SAH until proven otherwise; requires CT then LP, neurosurgical assessment.
2. Headache with fever and meningism (neck stiffness, Kernig's, Brudzinski's positive) — suspected bacterial or TB meningitis; immediate antibiotics + LP.
3. Headache with altered consciousness (GCS <15) or seizures — raised ICP, encephalitis, venous sinus thrombosis.
4. Headache with focal neurological deficits (hemiparesis, aphasia, visual loss, diplopia) — stroke, space-occupying lesion, or complicated migraine.
5. Headache with papilloedema on fundoscopy — raised ICP requiring urgent imaging.
6. Headache in the context of known malignancy or immunosuppression (HIV, steroids) — metastatic disease, opportunistic CNS infection.
7. Hypertensive emergency with headache (blood pressure >180/120 mmHg with target organ damage — including headache) — controlled BP reduction required.
8. Status migrainosus: a migraine attack persisting beyond 72 hours despite adequate treatment — requires IV hydration, parenteral analgesia, and monitoring.
9. First or worst headache of life, particularly if onset is abrupt and the patient cannot be safely observed at home.
Immediate supportive care in the emergency setting covers the following principles regardless of the specific headache aetiology: (a) Airway, breathing, circulation — in obtunded patients (meningitis, SAH with decreased consciousness), secure the airway; supplementary oxygen; IV access and fluid resuscitation in septic shock from meningococcaemia. (b) Analgesia and anti-emetics: IV or IM analgesia (IV paracetamol, IV/IM ketorolac, IV metoclopramide, IV ondansetron) for pain and vomiting control, particularly when oral medication is not tolerated. (c) Seizure control: IV lorazepam or diazepam for active seizures; load with IV phenytoin or levetiracetam for status epilepticus. (d) Raised ICP emergency management: head elevation to 30°; IV mannitol 0.25–1 g/kg (osmotic diuresis reduces brain water and ICP); intubation and controlled hyperventilation (targets PaCO₂ 32–35 mmHg) as a temporising measure by reducing cerebral blood volume before definitive treatment; urgent neurosurgical referral.
Abortive (Acute) Therapy for Migraine
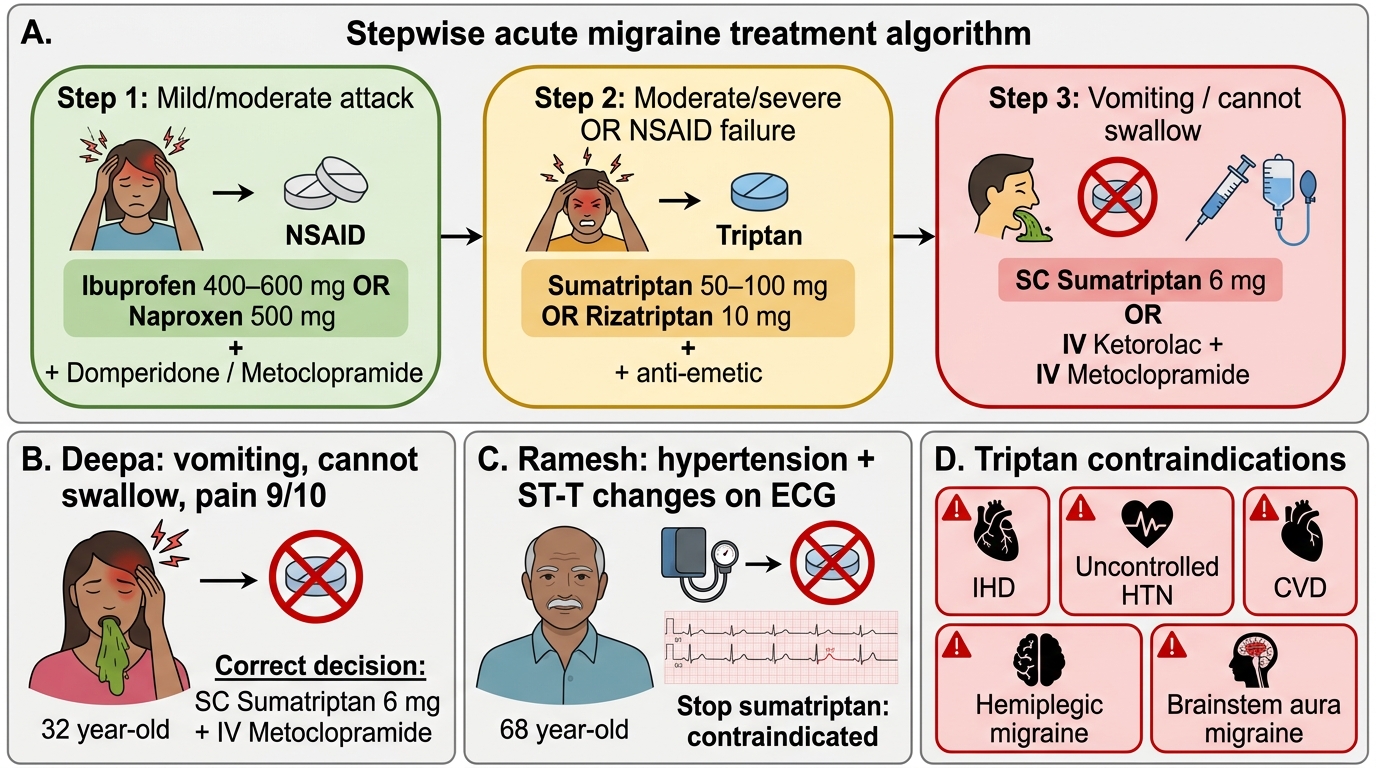
Abortive (acute) therapy for migraine aims to terminate an individual attack as rapidly and completely as possible, with the goal of restoring normal function within 2 hours and preventing headache recurrence within 24 hours. The pharmacological choices for acute migraine treatment are stratified by attack severity, patient comorbidities, tolerability, and cost — and the correct prescription requires knowledge of the mechanism, dose, contraindications, and key adverse effects of each agent.
Step 1 — Mild-to-moderate migraine or mild-to-moderate attacks in a patient who has not tried adequate acute therapy:
NSAIDs are the recommended first-line agents. Ibuprofen 400–600 mg (maximum 3 g/day) is effective, well-tolerated, and widely available in India. Naproxen sodium 500–550 mg at onset, may repeat 500 mg after 2 hours (maximum 1250 mg/day) — superior to ibuprofen for longer-lasting attacks. Aspirin 900–1000 mg ± metoclopramide is effective (aspirin is a valid alternative in resource-limited settings). Paracetamol (acetaminophen) 1000 mg is modestly effective for mild attacks. Critical caveat: use of NSAIDs or paracetamol on ≥15 days/month for >3 months constitutes medication-overuse headache (MOH) and paradoxically worsens migraine frequency — patients must be counselled to limit acute analgesic use to ≤10–14 days/month.
Step 2 — Moderate-to-severe migraine or failure of simple analgesics:
Triptans are the most effective acute agents and the treatment of choice for moderate-to-severe migraine. All triptans are selective 5-HT₁B/₁D agonists — they constrict dilated intracranial vessels (via 5-HT₁B) and inhibit trigeminal nociceptor CGRP release and signal transmission (via 5-HT₁D). Key triptans available in India:
- Sumatriptan (first-in-class, most studied): 50–100 mg oral at headache onset; can repeat dose after 2 hours if initial response is partial but headache recurs; maximum 200 mg/24 hours. Subcutaneous (SC) formulation 6 mg: fastest onset (10–20 min), most effective route — used when oral intake is impossible due to vomiting (as in Deepa's case). Nasal spray 10–20 mg: intermediate onset, useful when oral is problematic.
- Rizatriptan: 10 mg oral (5 mg with propranolol, as propranolol inhibits rizatriptan metabolism via MAO-A); oral disintegrating tablet (wafer) available — dissolves on tongue without water, useful in nausea.
- Zolmitriptan: 2.5–5 mg oral; nasal spray 5 mg.
- Naratriptan: 2.5 mg; slower onset, longer duration, lower recurrence rate — may be preferred for prolonged attacks.
Triptan pharmacology and key adverse effects: CNS: dizziness, somnolence, paraesthesiae ('triptan sensations' — tingling, heaviness of limbs or chest, not cardiac in origin in most cases). Cardiovascular: mild transient vasoconstriction; 'chest tightness' is common (non-cardiac in most; monitor in high-risk patients). Triptan-associated chest pain is usually musculoskeletal or oesophageal, not ischaemic — but triptans must not be used without careful risk assessment in patients with established CAD.
Triptan contraindications (critical — must be known for prescribing):
- Ischaemic heart disease (angina, MI history, ECG with ischaemic changes like Ramesh) — ABSOLUTE contraindication due to coronary vasoconstriction risk
- Uncontrolled hypertension (BP >180/110 mmHg) — relative to absolute contraindication
- Cerebrovascular disease (prior TIA, stroke)
- Hemiplegic migraine (theoretical vasoconstriction risk)
- Migraine with brainstem aura
- Concurrent use of MAO-A inhibitors (risk of serotonin syndrome)
- Pregnancy (relative — limited safety data; sumatriptan has the most data)
Step 3 — Anti-emetics as adjuncts: Nausea and vomiting impair oral drug absorption by causing gastric stasis. Anti-emetics improve both nausea symptoms and drug absorption:
- Metoclopramide 10 mg oral or IV/IM: pro-kinetic (promotes gastric emptying) + anti-emetic; given 10–20 minutes before the analgesic to improve absorption. Extrapyramidal side effects (acute dystonia) with repeated use — more common in young women.
- Domperidone 10–20 mg: dopamine D2 antagonist; peripheral pro-kinetic without CNS effects (does not cross BBB); safer for repeated use than metoclopramide. Avoid high doses due to QTc prolongation risk.
- Ondansetron 4–8 mg: 5-HT₃ antagonist; primarily anti-emetic without pro-kinetic effect; useful when vomiting is severe; IV formulation for emergency use.
Ergotamine and dihydroergotamine (DHE): Non-selective 5-HT agonists and vasoconstrictor agents. DHE 1 mg IM or IV is effective for acute migraine in the emergency department; ergotamine tartrate 1–2 mg oral is an older agent. Contraindicated in cardiovascular disease, cerebrovascular disease, peripheral vascular disease, and with triptans (risk of combined vasoconstriction). Ergotamine overuse (>2 days/week) causes ergotamine-dependent MOH.
Acute Migraine Treatment Algorithm
SELF-CHECK
Deepa (32-year-old migraineur, 4-hour attack, vomiting, cannot swallow, pain 9/10) and Ramesh (68-year-old with hypertension, ECG showing ST-T changes, told he has migraine, started on sumatriptan last month). Which management decision is correct for each patient?
A. Deepa: oral sumatriptan 100 mg; Ramesh: increase sumatriptan dose to 100 mg
B. Deepa: SC sumatriptan 6 mg + IV metoclopramide; Ramesh: stop sumatriptan — it is contraindicated; manage BP and consider IV ketorolac + anti-emetic
C. Deepa: IV morphine for severe pain; Ramesh: oral naproxen sodium 500 mg is safe with his cardiac history
D. Deepa: wait 2 more hours before treating; Ramesh: continue sumatriptan as the ECG changes are likely anxiety-related
Reveal Answer
Answer: B. Deepa: SC sumatriptan 6 mg + IV metoclopramide; Ramesh: stop sumatriptan — it is contraindicated; manage BP and consider IV ketorolac + anti-emetic
Deepa cannot swallow due to vomiting — oral medication is not absorbed in the presence of migraine-related gastric stasis. SC sumatriptan 6 mg is the appropriate route: fastest onset (10–20 min), highest bioavailability, unaffected by vomiting. IV metoclopramide treats both nausea and promotes gastric emptying. Ramesh has ischaemic heart disease (ECG with ST-T changes) — this is an absolute contraindication to all triptans and ergotamine due to coronary vasoconstriction risk. His sumatriptan must be stopped immediately. IV ketorolac (NSAID) + IV anti-emetic is appropriate acute management. IV morphine is not first-line for migraine. Naproxen sodium does NOT affect his cardiac contraindication to triptans.
Preventive (Prophylactic) Therapy for Migraine
Preventive (prophylactic) therapy for migraine aims to reduce the frequency, severity, and duration of attacks — and thereby improve quality of life and reduce the cumulative burden of acute medication use. It is a fundamentally different therapeutic goal from abortive therapy: where abortive drugs terminate an attack already in progress, preventive drugs alter the neurobiological milieu of the migraine brain to reduce the susceptibility to attacks in the first place. This distinction has practical clinical consequences — a patient may need both types of treatment simultaneously, and the failure of one category does not predict the failure of the other. The decision to initiate preventive therapy and the choice of agent requires systematic clinical assessment: how frequent are the attacks, how disabling, and which comorbidities could allow a single drug to serve dual purposes? These questions define the indications and agent selection criteria that constitute the IM17.12 competency.
Indications for preventive migraine therapy — at least one of the following should be present:
- Migraine attacks occurring on ≥4 days per month with significant impairment (even if individually brief)
- Severe or prolonged attacks (>48 hours) that significantly disrupt daily functioning even if infrequent
- Failure or contraindication of acute therapy (triptans contraindicated; NSAIDs causing MOH)
- Medication-overuse headache (MOH) — preventive therapy is initiated after or alongside detoxification
- Specific migraine subtypes: hemiplegic migraine, migraine with brainstem aura, or very frequent aura episodes
- Patient preference — after appropriate shared decision-making
A preventive treatment trial should be continued for at least 3 months at an adequate dose before assessing efficacy. A minimum 50% reduction in attack frequency is the standard efficacy criterion. If effective, continue for 6–12 months, then consider gradual withdrawal.
First-line preventive agents (must know mechanism, dose, contraindications, key adverse effects):
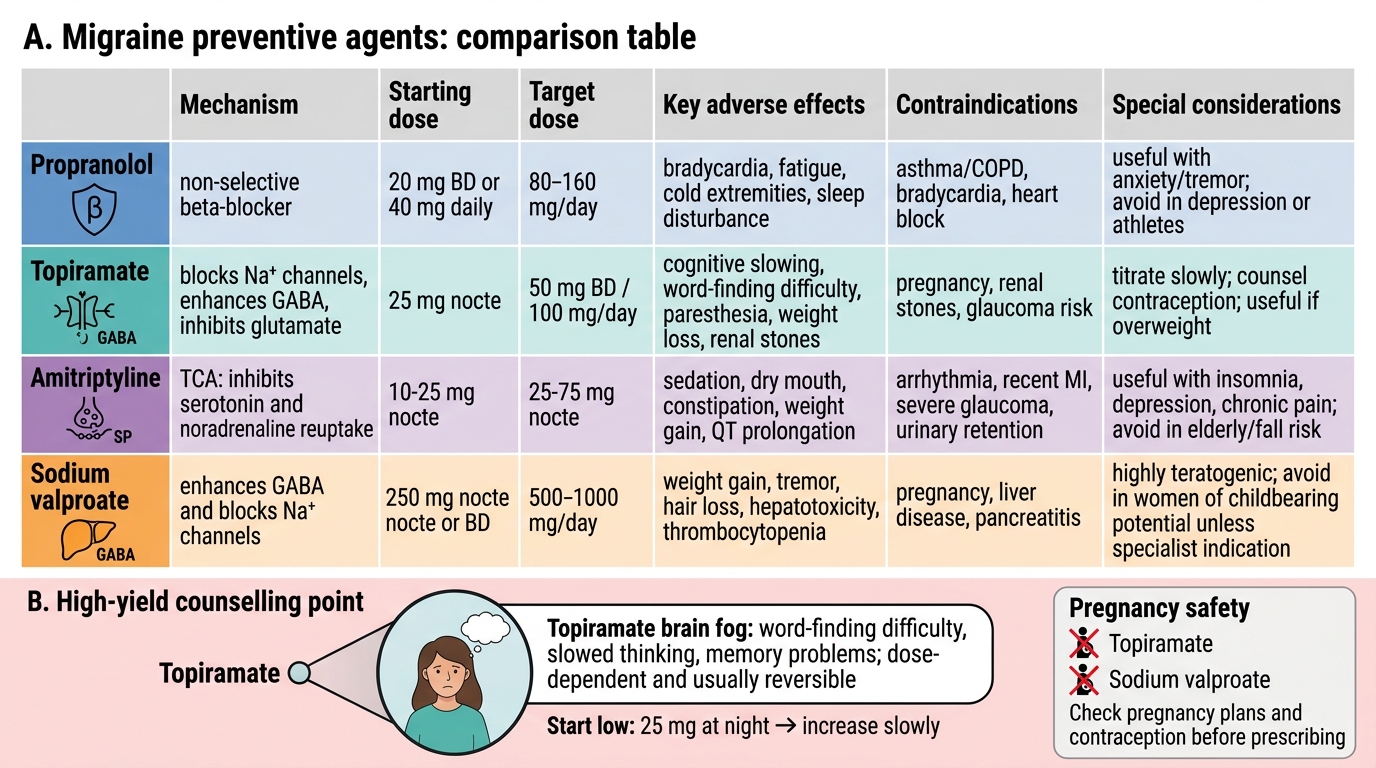
Propranolol (first-line, most evidence): Mechanism: non-selective beta-adrenoceptor blockade. Probable anti-migraine mechanism: blockade of central beta-adrenoceptors reduces noradrenergic hyperactivity in migraine generators; inhibition of platelet aggregation; stabilisation of vascular tone. Dose: start 20–40 mg twice daily; titrate to 40–120 mg twice daily (target dose 80–240 mg/day). Adverse effects: bradycardia, hypotension, fatigue, cold extremities, sleep disturbances, exacerbation of bronchospasm. Contraindications: asthma/COPD, heart block (>1st degree), decompensated heart failure, Raynaud's phenomenon, insulin-dependent diabetes (masks hypoglycaemia warning signs). Note: propranolol inhibits rizatriptan metabolism — use rizatriptan 5 mg (not 10 mg) if combined. Particularly useful in patients with hypertension or anxiety (dual benefit).
Topiramate (first-line, strong evidence): Mechanism: sodium channel blocker, calcium channel blockade (L-type), GABA potentiation, glutamate (AMPA/kainate receptor) inhibition, carbonic anhydrase inhibition. This broad mechanism profile reduces neuronal excitability and suppresses CSD propagation. Dose: start 25 mg at night; increase by 25 mg every 1–2 weeks; target 50–100 mg/day (given in two divided doses). Adverse effects: cognitive impairment ('topirmate' — difficulty with word-finding, memory, concentration — the most clinically significant side effect, dose-dependent and reversible with dose reduction), paraesthesiae (from carbonic anhydrase inhibition — usually benign), weight loss (may be desirable or undesirable), kidney stones (encourage hydration), acute angle-closure glaucoma (rare but serious — stop if eye pain/visual change), teratogenic (neural tube defects) — not safe in pregnancy; requires reliable contraception in women of reproductive age. Monitoring: renal function (carbonic anhydrase inhibition), eye examination if visual symptoms.
Amitriptyline (first-line, particularly for comorbid depression or insomnia): Mechanism: tricyclic antidepressant; blocks reuptake of serotonin and noradrenaline; sodium channel blockade; antihistamine. Anti-migraine mechanism is independent of antidepressant effect (occurs at lower doses). Dose: start 10 mg at night; titrate to 25–75 mg at night (anti-migraine doses are lower than antidepressant doses). Adverse effects: sedation, dry mouth, constipation, urinary retention, weight gain, prolonged QTc, postural hypotension. Contraindications: recent MI, cardiac arrhythmias, acute glaucoma, urinary retention, concurrent MAO inhibitor use. Preferred when migraine is comorbid with tension-type headache, insomnia, or depression.
Sodium valproate/valproic acid (first-line in non-pregnant adults): Mechanism: GABA-transaminase inhibition (raises brain GABA levels), sodium channel blockade, suppression of CSD. Dose: 500–1500 mg/day in divided doses. Adverse effects: weight gain, tremor, alopecia (reversible), teratogenic (highly teratogenic — neural tube defects, cognitive impairment in exposed offspring) — absolutely contraindicated in pregnancy and in women of childbearing potential without reliable contraception under the MHRA Pregnancy Prevention Programme. Hepatotoxicity and pancreatitis (rare but serious). Monitoring: liver function tests, full blood count (thrombocytopaenia), serum valproate levels if compliance concerns.
Second-line agents: Candesartan (angiotensin receptor blocker) 8–16 mg/day; lisinopril (ACE inhibitor) 10–20 mg/day; flunarizine (calcium channel blocker, not available in all markets); venlafaxine (SNRI) — useful with comorbid anxiety or depression. CGRP pathway monoclonal antibodies (erenumab, fremanezumab, galcanezumab): highly effective injectable preventives with excellent tolerability; not yet widely available or affordable in public healthcare settings in India but increasingly used in private practice.
Medication-overuse headache (MOH) management: Preventive therapy is ineffective if MOH is present. Primary treatment is analgesic detoxification — abrupt withdrawal of the overused drug (preferred for triptans and simple analgesics) or gradual tapering (preferred for opioids and butalbital-containing compounds to avoid withdrawal seizures). Detoxification causes a transient worsening of headache (withdrawal headache) for 1–2 weeks; warn the patient. Bridge therapy with a short course of oral prednisolone (60 mg/day tapering over 10 days) or IV dihydroergotamine can reduce withdrawal severity. Preventive therapy (topiramate, amitriptyline) initiated alongside or after detoxification.
Migraine Preventive Agents: Comparison Table
SELF-CHECK
A 27-year-old woman with migraine (6 attacks/month, each lasting 12–18 hours, significantly affecting her work) is started on topiramate for prevention. She should be counselled about which of the following adverse effects as the most clinically significant?
A. Bradycardia and cold extremities — common with topiramate due to beta-blockade
B. Cognitive impairment (word-finding difficulty, memory problems) — dose-dependent and reversible
C. Hepatotoxicity and thrombocytopaenia — require monthly LFT and CBC monitoring
D. Serotonin syndrome if combined with any analgesic for breakthrough attacks
Reveal Answer
Answer: B. Cognitive impairment (word-finding difficulty, memory problems) — dose-dependent and reversible
The most clinically significant adverse effect of topiramate that affects patient adherence is cognitive impairment — word-finding difficulty, slowed thinking, and memory problems ('topiramate brain fog'), which is dose-dependent and largely reversible with dose reduction or discontinuation. This is why topiramate is started at 25 mg at night and titrated slowly. Bradycardia and cold extremities are propranolol side effects, not topiramate. Hepatotoxicity and thrombocytopaenia are valproate side effects. Serotonin syndrome risk is primarily with triptans combined with serotonergic drugs, not topiramate. Additionally, because topiramate is teratogenic, this woman requires counselling about reliable contraception.