Page 7 of 21
IM18.8-9 | Stroke Diagnostic Testing — SDL Guide
Learning Objectives
- Choose and interpret appropriate imaging tests (NCCT, CTA, CT perfusion, MRI DWI/FLAIR/GRE) to identify the anatomical site, type, and aetiology of stroke
- Explain the ASPECTS score and its clinical significance for thrombolysis and mechanical thrombectomy eligibility
- Describe the aetiological workup for ischaemic stroke including ECG, echocardiography, carotid duplex, and laboratory investigations
- Select and interpret diagnostic testing in young patients with CVA — covering dissection, PFO, thrombophilia, vasculitis, CVST, and haematological and genetic causes
- Describe the investigation of haemorrhagic stroke including the CTA spot sign, GRE microbleeds, CSF xanthochromia for SAH, and cerebral angiography for aneurysm
INSTRUCTIONS
This module focuses on investigative decision-making for stroke. The imaging sections are best studied alongside actual CT and MRI examples — Radiopaedia.org provides freely accessible annotated cases. The young stroke section is high-yield for examinations; learn the extended workup by understanding the aetiology behind each test, not rote memorisation.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 427–428 — Cerebrovascular Disease (textbook)
- AHA/ASA 2019 Acute Ischaemic Stroke Guidelines — Imaging and Diagnostic Workup (guideline)
- ESO Guidelines for the Management of Ischaemic Stroke, 2021 (guideline)
- API Textbook of Medicine, 10th ed. — Cerebrovascular Diseases (textbook)
- Indian Stroke Association Consensus Statement — Investigation of Young Stroke, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old man has just been wheeled into the CT scanner bay. He presented with sudden-onset right hemiplegia 90 minutes ago. His NCCT brain is about to be reported. The radiologist calls you: 'The scan is normal — I don't see any haemorrhage, and I don't see any early infarct changes.' You have the clinical diagnosis of ischaemic stroke. The patient is within the thrombolysis window. Now what? The CT is only the beginning of the imaging story. You still need to decide: is there a large vessel occlusion amenable to thrombectomy? What is the extent of salvageable penumbra versus dead core? What is the underlying aetiology — is this atherosclerosis, cardioembolism, vasculitis, or dissection? And because he is only 38, you need a completely different investigation strategy for young stroke. Every imaging and laboratory decision in the next hour will shape both the acute management and the long-term prevention plan. This module teaches you to navigate the diagnostic workup precisely — choosing and interpreting the right test for the right question.
WHY THIS MATTERS
Stroke diagnostic testing is the bridge between the clinical syndrome and the treatment decision. The NMC competencies IM18.8 and IM18.9 require you to choose and interpret appropriate imaging tests to identify the anatomical site, type, and aetiology of stroke, and specifically to choose and interpret appropriate diagnostic testing in young patients with CVA — a population with a distinct aetiological spectrum requiring a targeted, extended workup. For a final-year student, the ability to interpret a brain CT in the acute setting (is there haemorrhage? are there early ischaemic changes? is the ASPECTS score acceptable for thrombolysis?), select appropriate vascular imaging, and know what to order in a young stroke patient is directly tested in clinical examinations and is an operational skill needed from day one of internship. India's stroke registries consistently show high rates of young stroke, making IM18.9 particularly relevant to local clinical practice.
RECALL
Before proceeding, activate your prior knowledge. Recall that non-contrast CT (NCCT) brain is the first imaging in acute stroke, with the primary purpose of excluding haemorrhage — haemorrhage appears hyperdense (bright) on NCCT immediately. Recall that ischaemic stroke may not be visible on NCCT in the first 6 hours; MRI diffusion-weighted imaging (DWI) can detect acute ischaemia within minutes. Recall the TOAST classification of ischaemic stroke aetiology: large artery atherosclerosis, cardioembolism (AF, valvular disease, mural thrombus), small vessel (lacunar), other determined aetiology (thrombophilia, vasculitis, dissection), and cryptogenic. Recall that in young adults, the 'other determined' and 'cryptogenic' categories are proportionately much larger than in the elderly, and that causes like arterial dissection, thrombophilia, and paradoxical embolism through a patent foramen ovale become leading contenders. These categories are what drives the extended workup in young stroke.
Neuroimaging in Acute Stroke — CT and MRI
Neuroimaging is the cornerstone of stroke diagnosis, driving every acute management decision and the long-term aetiological workup. The choice between CT and MRI — and the specific sequences or phases within each modality — depends on the clinical question being asked. In the acute setting, the sequence of imaging follows a logical progression from ruling out haemorrhage, to identifying large vessel occlusion, to quantifying the salvageable penumbra, and finally to characterising the aetiology. Understanding this sequence — and why each step comes in the order it does — prevents the common error of ordering the most sophisticated test first while missing the simple question that determines whether any treatment is safe.
Non-contrast CT (NCCT) brain — first imaging, always:
NCCT brain is the universal first-line investigation in suspected acute stroke. It is widely available, rapid (acquisition in under 5 minutes), and highly sensitive for haemorrhage — ICH appears as an area of hyperdensity (HU 60–80) immediately after onset. The critical question NCCT answers in the acute phase is NOT 'is there an infarct?' but rather: 'Is there haemorrhage?' If the answer is no, thrombolysis is not contraindicated on imaging grounds. Several key NCCT findings must be recognised:
- Hyperdense MCA sign: the thrombosed proximal MCA appears hyperdense compared to the contralateral MCA — a direct sign of intra-arterial thrombus. Sensitivity ~35–50%, specificity ~90%. Its presence confirms large vessel occlusion and should trigger CT angiography.
- Dense basilar artery sign: analogous sign in the posterior circulation — hyperdense basilar artery indicating thrombosis. A neurological emergency (basilar artery occlusion = locked-in syndrome or death without thrombectomy).
- Early ischaemic changes (visible in 30–60% of strokes within 3–6 hours): subtle signs include loss of the insular ribbon (the grey-white interface at the insula becomes blurred), sulcal effacement (gyri appear swollen), and loss of grey-white differentiation in the basal ganglia. These signs indicate established infarction — their extent is quantified by the ASPECTS score.
The ASPECTS score (Alberta Stroke Programme Early CT Score) evaluates 10 defined regions of the MCA territory on axial NCCT. Each region with early ischaemic change loses 1 point from a starting score of 10. ASPECTS 10 = no ischaemic change; ASPECTS 0 = the entire MCA territory is infarcted. An ASPECTS score ≤6 indicates extensive established infarction — these patients have higher risk of haemorrhagic transformation with thrombolysis and lower expected functional benefit; current guidelines generally favour ASPECTS ≥6 for mechanical thrombectomy.
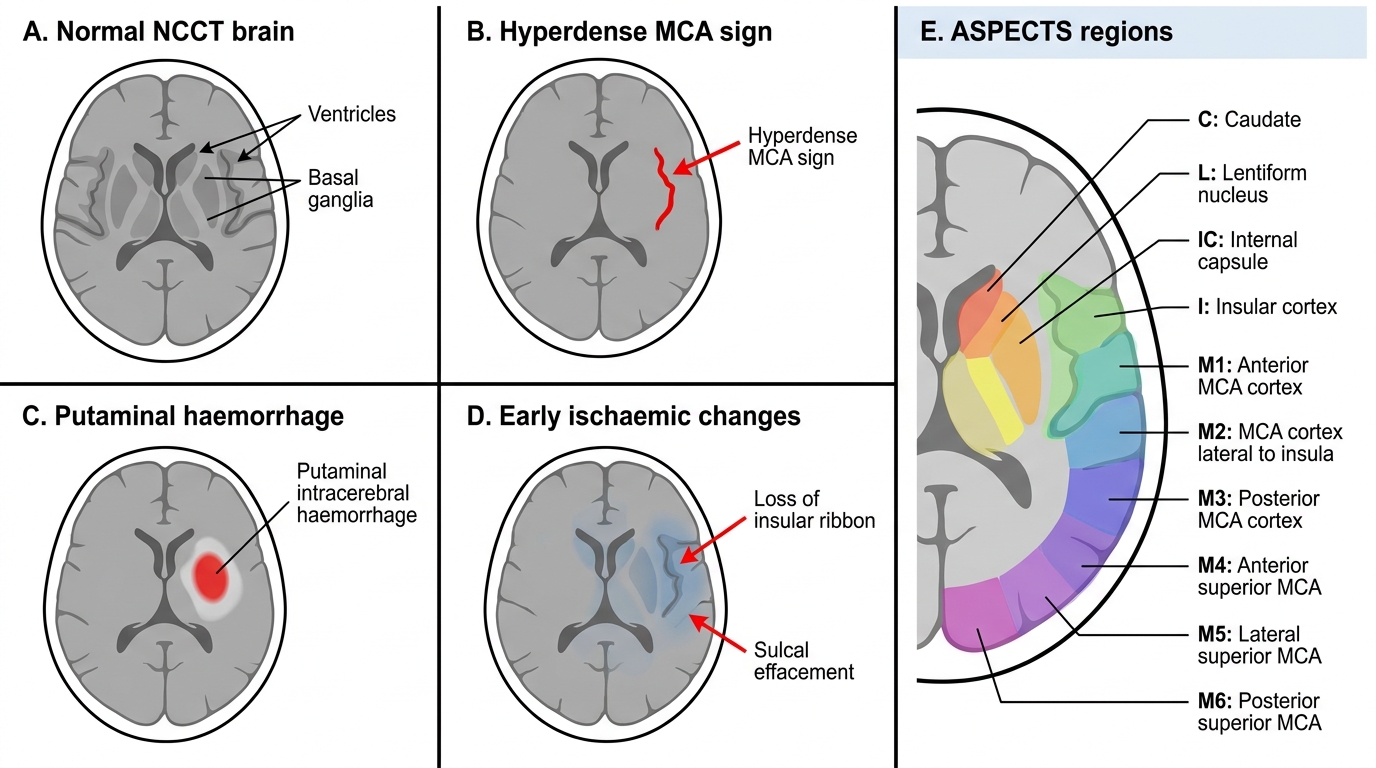
NCCT Brain Findings in Acute Stroke
CT angiography (CTA) — identifying the occlusion site:
CTA from the aortic arch to the vertex is the next step when large vessel occlusion is suspected (NIHSS ≥6, hyperdense MCA sign, or posterior circulation symptoms). It simultaneously images cervical carotid and vertebral arteries (for stenosis, dissection, or atherosclerotic plaque) and the intracranial vessels (for site and extent of occlusion). Key findings: site of occlusion for thrombectomy planning; carotid stenosis >70% = indication for endarterectomy/stenting; dissection (intimal flap, pseudoaneurysm, string sign); venous phase for CVST.
CT perfusion (CTP) — quantifying penumbra vs core:
CT perfusion maps cerebral blood flow (CBF), cerebral blood volume (CBV), mean transit time (MTT), and time-to-peak (TTP). The core-penumbra mismatch (penumbra:core ratio >1.8 with penumbra >15 mL) identifies patients who benefit from late-window thrombectomy (6–24 hours), as established in the DAWN and DEFUSE-3 trials.
MRI in acute stroke:
MRI provides superior sensitivity for ischaemic infarction. Key sequences:
- DWI: detects restricted diffusion (bright on DWI, dark on ADC) within minutes — the most sensitive early test for ischaemia; detects posterior fossa infarcts missed by CT
- FLAIR: positive >4.5–6 hours after onset; DWI-FLAIR mismatch (DWI bright, FLAIR dark) = stroke <4.5 hours → wake-up stroke protocol
- GRE/SWI: haemorrhage as 'blooming' dark signal; microbleeds (CAA, hypertensive small vessel disease)
- MRA: non-contrast TOF intracranial vessel imaging; contrast-enhanced MRA of neck
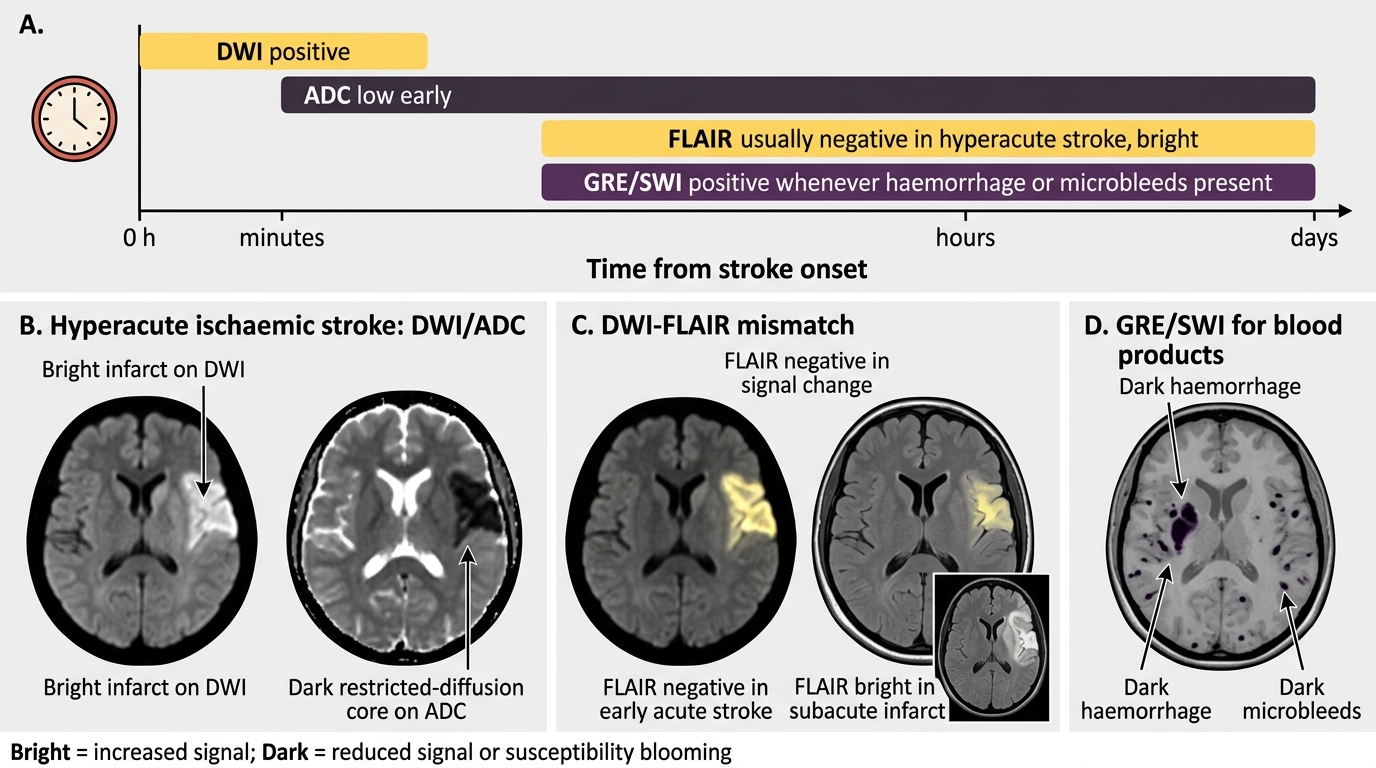
MRI Sequences in Acute Stroke
Cardiac and Vascular Investigations for Stroke Aetiology
Once the acute imaging phase has established stroke type and excluded haemorrhage, the aetiological workup begins in parallel with initial management. Identifying the aetiology is not academic — it directly determines secondary prevention (antiplatelet vs anticoagulant, statin intensity, blood pressure target, carotid surgery, cardiac ablation). The investigation sequence follows the TOAST classification: the clinical and imaging profile suggests the most likely mechanism, and targeted investigations confirm or refute it. A patient with ischaemic stroke for whom no aetiology is identified receives less effective secondary prevention — the investigation is therefore as important as the acute treatment.
ECG and cardiac monitoring:
A 12-lead ECG is mandatory in all stroke patients and performed immediately — it may reveal AF (most common cardiac cause), recent MI, or LVH. A single ECG detects AF in only 5–10% of patients with paroxysmal AF. Prolonged cardiac monitoring substantially increases detection: 24-hour Holter captures an additional 5–10%; 7-day external loop recorder 15–20%; implantable cardiac monitor (ICM) over 3 years up to 30% of cryptogenic strokes. Guidelines recommend at least 24-hour monitoring in all acute stroke patients, with prolonged monitoring for cryptogenic stroke.
Echocardiography:
Transthoracic echocardiography (TTE) identifies LV thrombus (post-MI, cardiomyopathy), valvular disease (rheumatic mitral stenosis — important in India), aortic arch atheroma, and reduced LVEF. Transoesophageal echocardiography (TOE) has superior sensitivity for left atrial appendage (LAA) thrombus (the AF-related thrombus site — LAA not well seen on TTE), patent foramen ovale (PFO) with bubble contrast study (agitated saline + Valsalva — bubbles in LA within 3 heartbeats = positive right-to-left shunt), and aortic arch plaques. TOE is particularly indicated in young cryptogenic stroke.
Carotid duplex ultrasonography:
First-line test for carotid artery disease — images the CCA, bifurcation, and proximal ICA; measures intima-media thickness and characterises plaque. Clinical significance: symptomatic stenosis ≥50% ipsilateral = large artery atherosclerosis; ≥70% symptomatic stenosis = indication for carotid endarterectomy (CEA) within 2 weeks (NASCET/ECST trial evidence) or carotid artery stenting (CAS).
Routine laboratory tests in all stroke patients:
- FBC: polycythaemia, thrombocythaemia, thrombocytopenia
- Fasting glucose + HbA1c: diabetes status; hyperglycaemia worsens outcome
- Fasting lipid profile: LDL target for statin therapy
- Renal function: impacts anticoagulant and statin choice
- Coagulation screen (PT/INR, APTT): if anticoagulated or coagulopathy suspected
- ESR + CRP: elevated in vasculitis, endocarditis, inflammatory states
- Thyroid function: hyperthyroidism causes AF; hypothyroidism causes dyslipidaemia
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
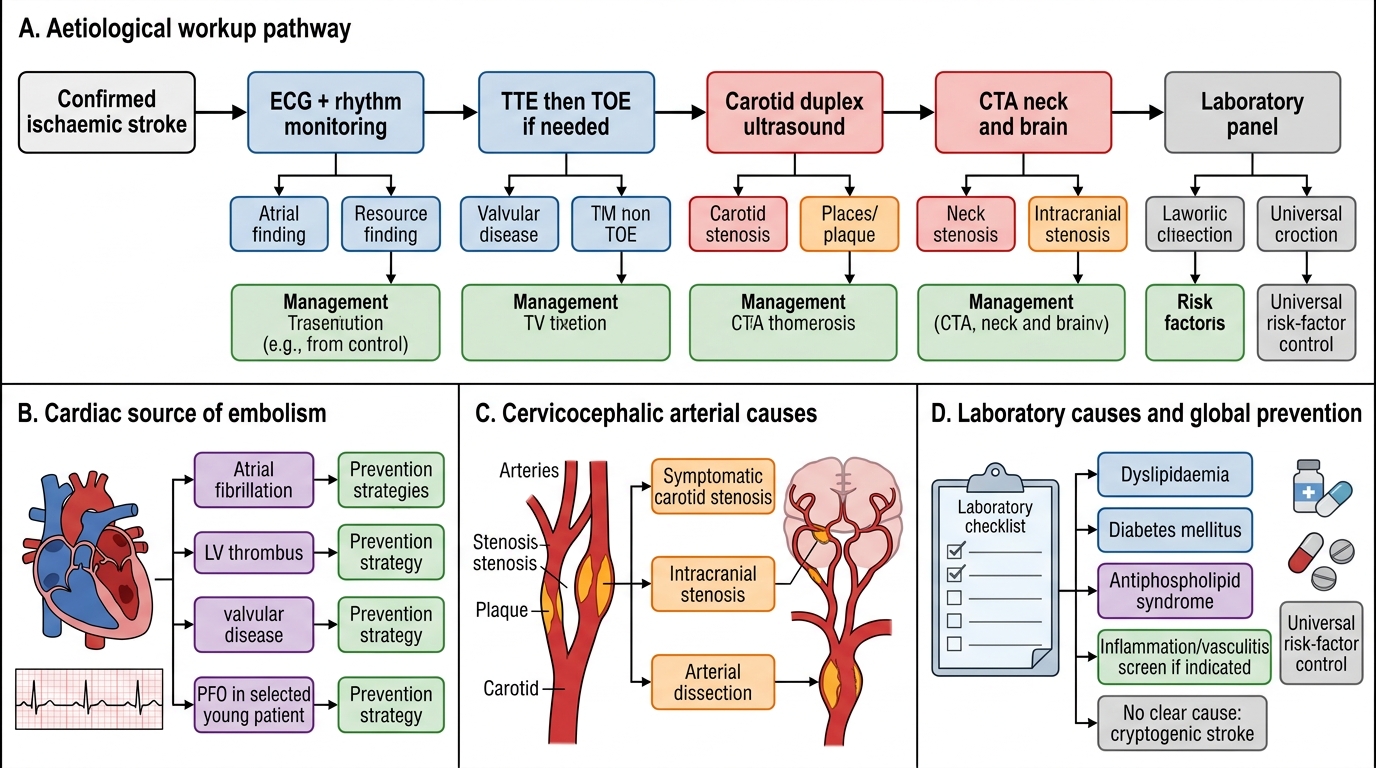
Aetiological Workup After Ischaemic Stroke
SELF-CHECK
A 70-year-old patient with acute left MCA territory stroke has NCCT showing early ischaemic changes in 4 of the 10 ASPECTS regions. What is the ASPECTS score and what does it indicate for mechanical thrombectomy?
A. ASPECTS 4 — severe infarction; NOT a candidate for mechanical thrombectomy
B. ASPECTS 6 — borderline; thrombectomy decision requires integration with clinical severity and perfusion imaging
C. ASPECTS 10 — normal; no contraindication to thrombectomy
D. ASPECTS 8 — mild infarction; thrombectomy strongly indicated
Reveal Answer
Answer: B. ASPECTS 6 — borderline; thrombectomy decision requires integration with clinical severity and perfusion imaging
ASPECTS = 10 minus the number of regions with early ischaemic changes. 4 regions involved → ASPECTS = 10 − 4 = 6. ASPECTS 6 is the commonly cited lower threshold for mechanical thrombectomy eligibility — current guidelines generally favour ASPECTS ≥6. An ASPECTS of exactly 6 is borderline: it does not automatically exclude thrombectomy, but the decision should be made by integrating clinical severity, time from onset, presence of large vessel occlusion, and CT perfusion mismatch. ASPECTS ≤5 (not 4) would indicate more extensive established infarction where the risk-benefit calculation shifts against thrombectomy. Options A and D misidentify the ASPECTS value. Option C confuses the score calculation.
Diagnostic Workup in Young Stroke (Age <45 Years)
Young stroke — conventionally defined as stroke in patients aged 18–45 years — requires a fundamentally different and extended aetiological investigation strategy compared to elderly stroke. The aetiological spectrum shifts dramatically: traditional cardiovascular risk factors (hypertension, atherosclerosis, AF) are less common, while rare but important causes — arterial dissection, thrombophilia, paradoxical embolism through PFO, vasculitis, haematological disorders, and genetic diseases — become the principal diagnostic targets. In India, young stroke is disproportionately common compared to Western countries, accounting for nearly 20–30% of all stroke admissions in some registries. Rheumatic heart disease remains a significant cardiac cause in this age group, and Takayasu arteritis is an important vasculitis to consider in young Indian women. Failing to investigate young stroke systematically leaves the patient without a diagnosis, without appropriate secondary prevention, and at high risk of recurrence from a treatable cause.
Arterial dissection — most common cause of young ischaemic stroke:
Spontaneous or traumatic dissection of the carotid or vertebral artery accounts for 10–25% of young stroke in many series. The mechanism is thromboembolism from the dissection site. Clinical clues: ipsilateral neck or head pain before the stroke; ipsilateral Horner syndrome (sympathetic fibres run along the ICA); posterior circulation stroke in a young person (vertebral artery dissection after sport or minor neck movement). Imaging: CTA or MRA of neck and intracranial vessels shows the narrow 'string sign', intimal flap, or pseudoaneurysm. T1 fat-saturation MRI of the neck is the gold standard — the intramural haematoma appears as a crescent of T1 hyperintensity within the vessel wall, displacing the flow void. A standard brain MRI does NOT adequately image the cervical vessels.
Patent foramen ovale (PFO) and paradoxical embolism:
PFO is present in ~25–30% of the general population but found in 40–50% of young cryptogenic stroke patients, implicating paradoxical embolism as the mechanism. Investigation: TOE with bubble contrast (agitated saline) during Valsalva — bubbles in the left atrium within 3 heartbeats = positive right-to-left shunt. PFO closure (transcatheter device) is recommended in selected cryptogenic stroke patients aged 18–60 with large PFO, no atrial fibrillation, and no other explanation (CLOSE, REDUCE, DEFENSE-PFO trial evidence).
Thrombophilia screen:
Protein C deficiency, protein S deficiency, antithrombin III deficiency, Factor V Leiden (activated protein C resistance), prothrombin gene mutation (G20210A), and antiphospholipid syndrome (APS) are the key inherited or acquired hypercoagulable states. APS criteria: clinical (arterial or venous thrombosis or obstetric morbidity) PLUS laboratory (lupus anticoagulant, anticardiolipin IgG/IgM, anti-β2GP1 antibodies) on two occasions ≥12 weeks apart. A single positive antiphospholipid test does NOT diagnose APS.
Vasculitis:
CNS vasculitis: headache, encephalopathy, focal deficits, CSF pleocytosis, multiple infarcts in different territories on MRI. Systemic vasculitis: Takayasu arteritis — granulomatous inflammation of the aorta and major branches including the carotid and vertebral origins, predominantly young Asian women; presents with limb claudication, bruits, absent pulses, or stroke; CTA/MRA shows wall thickening, stenosis, and aneurysm; ESR elevated. SLE-related stroke (vasculitis, Libman-Sacks endocarditis, APS). Workup: ESR, CRP, ANA, ANCA, complement, anti-dsDNA.
Haematological and genetic causes:
Sickle cell disease (HbSS): stroke in 11% of patients by age 20; annual transcranial Doppler screening in paediatric HbSS. Polycythaemia vera, essential thrombocythaemia. Genetic: CADASIL (NOTCH3 mutation — recurrent lacunar strokes, anterior temporal white matter changes on MRI, family history of early stroke); MELAS (mitochondrial — elevated serum lactate, stroke-like episodes not in vascular territories, maternal inheritance); Fabry disease (GLA mutation, X-linked — neuropathic pain, angiokeratomas, renal failure, stroke in young males).
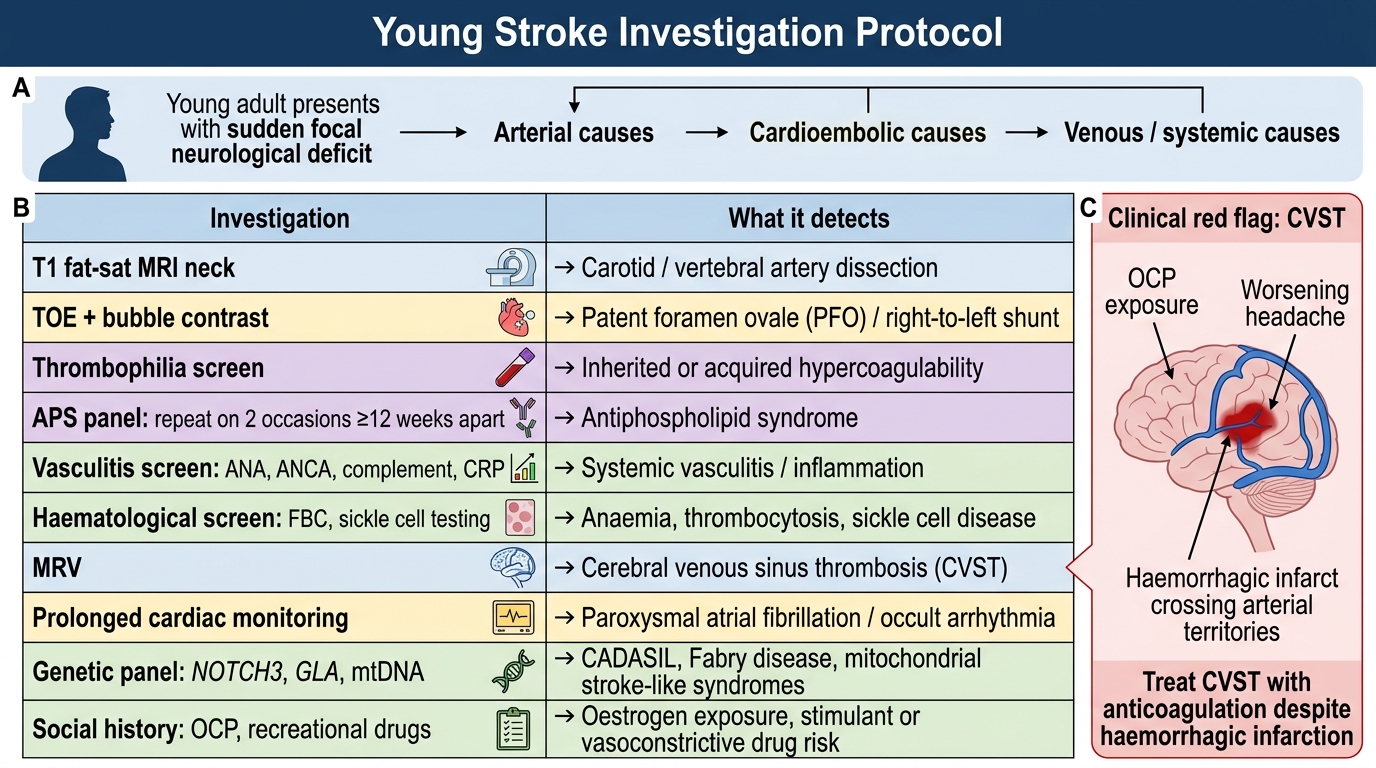
Young Stroke Investigation Protocol
SELF-CHECK
A 32-year-old woman presents with sudden right hemiplegia 2 days after starting combined oral contraceptive pills. She had a 5-day history of worsening headache. CT brain shows a haemorrhagic infarction in the right hemisphere that does not conform to any standard arterial territory. What is the diagnosis and the correct treatment?
A. Cardioembolic stroke from OCP-induced AF — withhold anticoagulation because of haemorrhage
B. Cerebral venous sinus thrombosis (CVST) — treat with anticoagulation (LMWH then warfarin or DOAC) despite the haemorrhage on CT
C. Ischaemic stroke from antiphospholipid syndrome — give aspirin only
D. Hypertensive ICH from OCP-related hypertension — treat conservatively without anticoagulation
Reveal Answer
Answer: B. Cerebral venous sinus thrombosis (CVST) — treat with anticoagulation (LMWH then warfarin or DOAC) despite the haemorrhage on CT
This is CVST: young woman on OCP (oestrogen drives a hypercoagulable state and predisposes to CVST), preceding headache (raised ICP from impaired venous drainage), haemorrhagic infarction not conforming to an arterial territory (venous infarcts cross arterial boundaries). CVST is treated with anticoagulation — LMWH initially, then warfarin or DOAC — EVEN when there is haemorrhagic infarction. This is the critical exception: the haemorrhage in CVST is caused by venous hypertension (not arterial rupture), and anticoagulation stops thrombosis propagation and reduces venous pressure, actually reducing bleeding risk. Withholding anticoagulation in CVST because of CT haemorrhage is a potentially fatal error. OCP should be stopped immediately. Diagnosis is confirmed by MRI + MRV showing absent flow signal in the sinus.