Page 2 of 21
IM18.1-2 | Stroke Foundations — SDL Guide (Part 2)
The Ischaemic Penumbra and Therapeutic Window — Core Concepts
The concept of the ischaemic penumbra is arguably the most important pathophysiological concept in stroke medicine, because it provides the entire biological rationale for time-critical reperfusion therapies. Understanding the penumbra explains not only why treatment must be delivered urgently but also how to image the penumbra to identify patients who may still benefit from reperfusion even beyond the conventional time window. The penumbra concept is what transforms 'time is brain' from a slogan into a precisely quantifiable biological reality: every minute of major vessel occlusion, approximately 1.9 million neurons, 14 billion synapses, and 12 km of myelinated fibres are lost in the ischaemic territory. Restoring flow 30 minutes earlier translates into measurable survival of neuronal tissue and measurable improvement in clinical outcome — a relationship that motivates every element of the stroke pathway from pre-hospital triage to door-to-needle time targets.
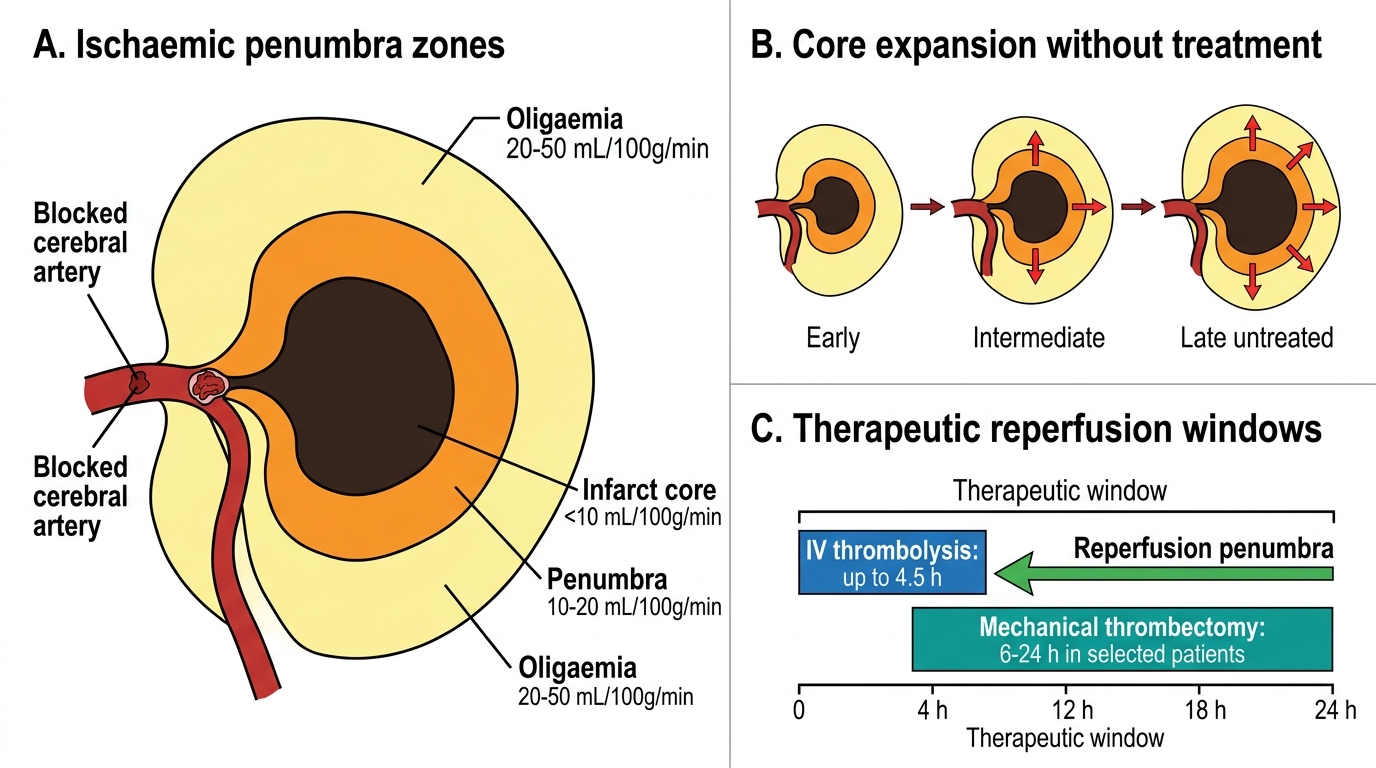
Following arterial occlusion, cerebral blood flow (CBF) falls below normal (50 mL/100 g/min) throughout the affected territory. The degree of CBF reduction determines the cellular fate:
- Core (CBF <10–15 mL/100 g/min): within minutes, ATP production ceases, membrane pumps fail, glutamate floods the extracellular space, and calcium influx triggers irreversible neuronal death via excitotoxicity, oxidative stress, and mitochondrial dysfunction. This tissue is already lost — reperfusion cannot rescue it, and may actually worsen outcome by converting ischaemic into haemorrhagic infarction.
- Penumbra (CBF 15–25 mL/100 g/min): cells are electrically silent (the CBF threshold for function is higher than for survival), ATP is still being produced (reduced oxidative phosphorylation, sustained partly by glycolysis), and salvage is possible if perfusion is restored within the therapeutic window. Without reperfusion, these cells progressively die as the core expands. The speed of core expansion depends on collateral circulation — patients with good collaterals have a larger penumbra sustained for longer; patients with poor collaterals have rapid core expansion.
- Oligaemia/benign oligaemia (CBF 25–50 mL/100 g/min): reduced flow but above the electrical and metabolic threshold; may be mildly symptomatic or asymptomatic. This tissue does not die even without treatment.
The penumbra-core mismatch can be imaged using CT perfusion (CTP) or MRI perfusion-diffusion mismatch:
- DWI (diffusion-weighted imaging) MRI: shows the infarct core as restricted diffusion (bright on DWI, dark on ADC) within minutes of onset.
- PWI (perfusion-weighted imaging) or CT perfusion: shows the hypoperfused territory including both core and penumbra.
- A large mismatch (penumbra >> core) indicates a large amount of salvageable tissue — this patient is likely to benefit from reperfusion even if they present at 6–24 hours.
This penumbra imaging principle is the basis for the DAWN and DEFUSE-3 trials that extended the window for mechanical thrombectomy to 24 hours in selected patients with a large penumbra-core mismatch and a proximal large-vessel occlusion.
Ischaemic Penumbra and Therapeutic Window
SELF-CHECK
Which of the following correctly describes the difference between ischaemic stroke core and penumbra in terms of cerebral blood flow thresholds and salvageability?
A. Core: CBF <25 mL/100g/min, irreversible; Penumbra: CBF 25–50 mL/100g/min, reversible with reperfusion
B. Core: CBF <10–15 mL/100g/min, irreversibly necrotic; Penumbra: CBF 15–25 mL/100g/min, salvageable if reperfused within the therapeutic window
C. Core: CBF <30 mL/100g/min, reversible with thrombolysis; Penumbra: CBF 30–50 mL/100g/min, irreversible
D. Core and penumbra have the same CBF; the distinction is based on time elapsed since onset only
Reveal Answer
Answer: B. Core: CBF <10–15 mL/100g/min, irreversibly necrotic; Penumbra: CBF 15–25 mL/100g/min, salvageable if reperfused within the therapeutic window
The core is defined by very low CBF (<10–15 mL/100 g/min) where irreversible neuronal death has already occurred via excitotoxicity and energy failure — reperfusion cannot rescue this tissue. The penumbra has intermediate CBF (15–25 mL/100 g/min): cells are electrically silent and non-functional, but metabolically viable and potentially recoverable if blood flow is restored within the therapeutic window. This mismatch is the biological rationale for thrombolysis and thrombectomy. Option A gives incorrect thresholds. Option C incorrectly calls the core reversible. Option D is incorrect — CBF thresholds, not just time, define the zones, though time determines how much penumbra remains.
Stroke Diagnosis: Initial Approach and Differential
The initial approach to a patient presenting with acute focal neurological deficit requires rapid clinical recognition that this may be a stroke and immediate exclusion of conditions that mimic stroke. The diagnostic process begins in the first minutes of the patient encounter, running simultaneously with initial resuscitation and stabilisation.
Provided image
The most widely used and validated bedside screening tool for stroke recognition is the FAST acronym: Face drooping (ask the patient to smile — is one side drooping?), Arm weakness (ask the patient to raise both arms — does one drift downward?), Speech difficulty (ask the patient to repeat a simple phrase — is speech slurred or garbled?), Time (time of symptom onset and time to call for help). The FAST test has a sensitivity of approximately 72% for ischaemic stroke but misses posterior circulation strokes (vertigo, ataxia, diplopia, dysarthria — without facial or arm involvement). The BEFAST variant adds Balance and Eyes to improve sensitivity for posterior circulation events.
The differential diagnosis of acute stroke includes conditions that mimic stroke — 'stroke mimics' — which account for 5–30% of suspected stroke presentations:
- Hypoglycaemia: the most important and immediately reversible stroke mimic; focal weakness and altered consciousness can be indistinguishable from stroke. Blood glucose must be checked immediately in every suspected stroke patient. A glucose <3.5 mmol/L (63 mg/dL) causing focal deficits is treated with IV dextrose; if deficits resolve, the diagnosis is hypoglycaemia, not stroke.
- Hypertensive encephalopathy and PRES (posterior reversible encephalopathy syndrome): headache, confusion, visual disturbance, and seizures in the context of severely elevated blood pressure; imaging shows reversible vasogenic oedema predominantly in the posterior white matter.
- Todd's paresis (postictal weakness): focal weakness following a generalised or focal seizure; typically resolves over minutes to hours; history of seizure is the key.
- Migraine with aura: focal neurological symptoms (visual aura, motor or sensory symptoms) followed by headache; usually positive past history; aura is typically slow-spreading (not sudden-onset).
- Functional (conversion) neurological symptom disorder: inconsistent neurological signs, positive Hoover sign, history of psychiatric illness.
- Intracranial mass lesion (tumour, abscess, subdural haematoma): can present acutely with focal deficits; CT will distinguish. A large subdural haematoma following trauma or in anticoagulated patients can present with sudden focal deficits.
- Metabolic encephalopathy (hyponatraemia, hepatic encephalopathy): diffuse rather than focal, but some focality can occur.
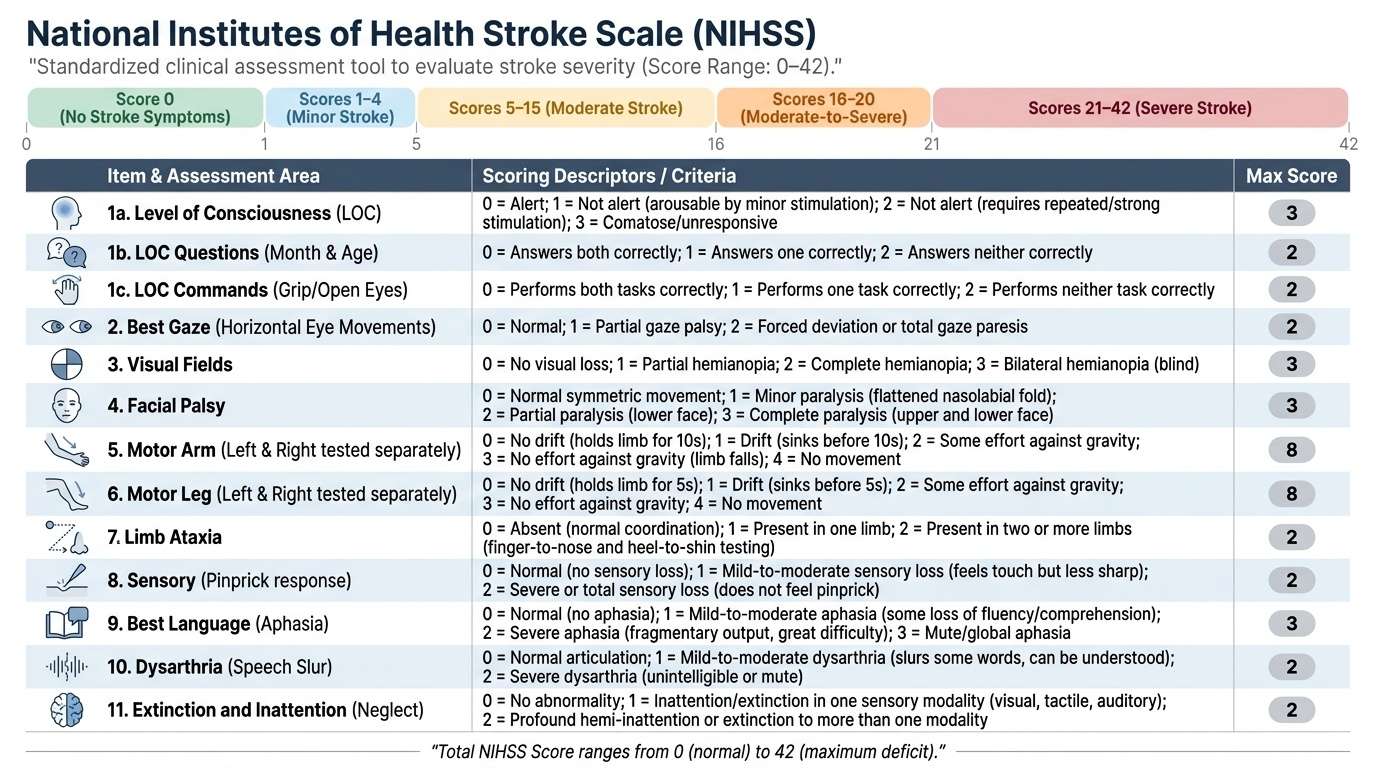
The NIHSS (National Institutes of Health Stroke Scale) is the standard validated tool for quantifying neurological deficit severity in acute stroke. It assesses 11 domains (level of consciousness, best gaze, visual fields, facial palsy, arm motor, leg motor, limb ataxia, sensory, best language, dysarthria, extinction/inattention) on a 0–4 or 0–2 scale, with a total range of 0–42. An NIHSS score of 0–4 = minor stroke; 5–15 = moderate; 16–20 = moderate-severe; ≥21 = severe. The NIHSS is important for determining eligibility for thrombolysis and mechanical thrombectomy, for monitoring response to treatment, and for prognostication. All final-year students must be familiar with the NIHSS components.
The first investigation in the emergency setting is non-contrast CT (NCCT) brain — the single most important initial imaging test. Its purpose in the acute phase is NOT primarily to diagnose ischaemic stroke but to exclude haemorrhage. ICH appears as a hyperdense (bright) lesion on NCCT immediately after onset. Ischaemic stroke is typically NOT visible on NCCT within the first 6 hours — the NCCT may be normal, or show only subtle early signs (hyperdense MCA sign — thrombosed artery appears bright; loss of the insular ribbon; sulcal effacement). If NCCT shows no haemorrhage, the patient can proceed to thrombolysis. The approach to full diagnostic workup (MRI, angiography, cardiac investigations) is covered in detail in the Stroke Diagnostic Testing SDL.
CLINICAL PEARL
The most dangerous error in acute stroke care is giving thrombolysis to a patient who actually has a haemorrhagic stroke — because it will convert a manageable haemorrhage into a fatal one. This is why non-contrast CT brain is mandatory before thrombolysis, even if every minute counts. The second-most-dangerous error is missing hypoglycaemia as the cause of a focal neurological deficit: always check a point-of-care blood glucose immediately in every suspected stroke — before ordering any imaging. Treating hypoglycaemia takes 30 seconds; a missed diagnosis costs the patient the entire reperfusion window.
A third pearl for this foundations module: the ABCD2 score after TIA is not just a risk stratification tool — it is an action trigger. Patients with an ABCD2 score ≥4 have a 10–15% risk of stroke within the next 2 days without treatment. Dual antiplatelet therapy (aspirin + clopidogrel) for 21 days, started immediately after TIA, reduces this early recurrence risk by approximately 75% in high-risk patients (POINT and CHANCE trials). Every TIA patient must be risk-stratified with ABCD2 within the first hour.
Principles of Acute Stroke Management — Overview
The management of stroke is governed by two overarching imperatives that flow directly from the pathophysiology covered in this module: first, restore perfusion as rapidly as possible to salvage the ischaemic penumbra in acute ischaemic stroke; second, prevent early recurrence and secondary brain injury regardless of stroke type. Although the detailed management of ischaemic and haemorrhagic stroke is covered in dedicated SDLs, the foundations module must establish the broad management framework so that the classification and pathophysiology knowledge is anchored to clinical action. Without this anchor, the TOAST subtypes remain abstract categories rather than treatment-driving diagnoses.
Provided image
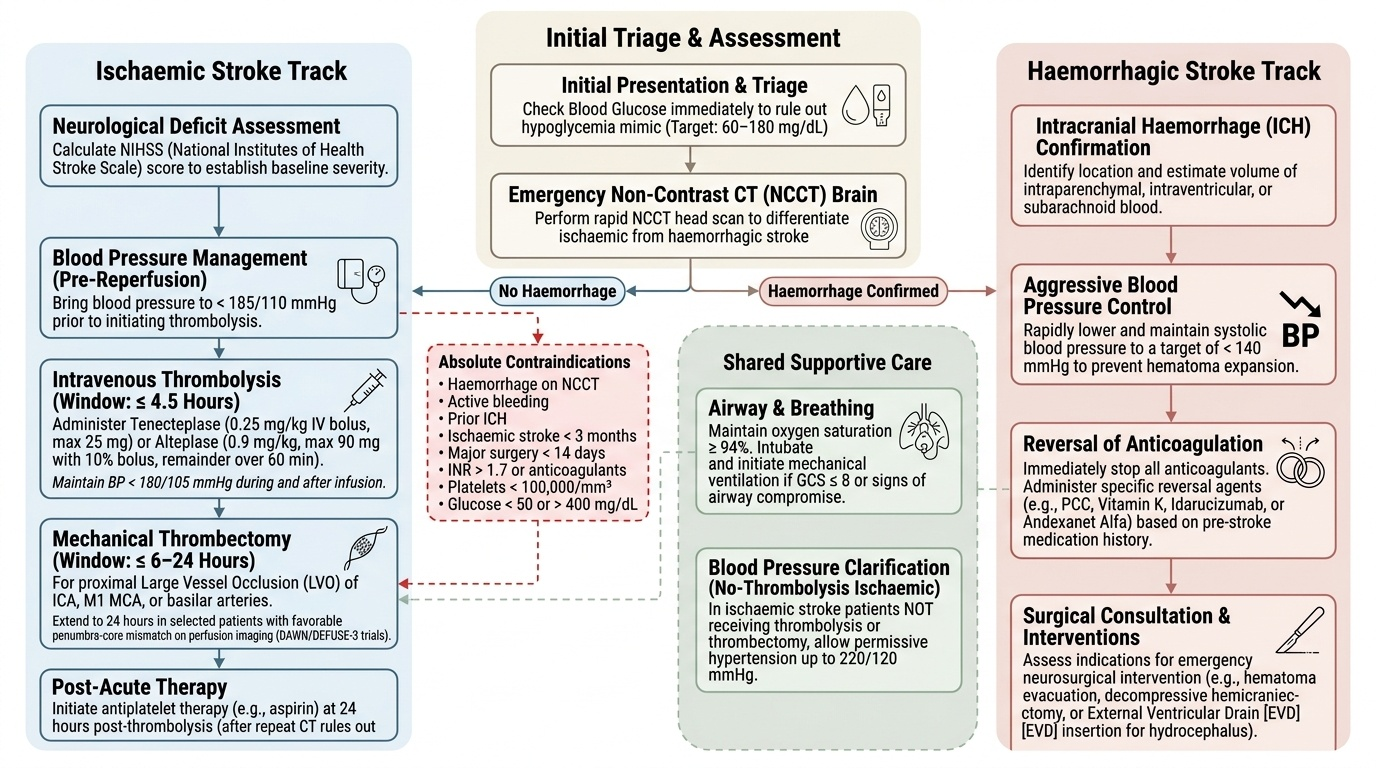
Acute ischaemic stroke — the reperfusion imperative:
The single most time-sensitive intervention is intravenous thrombolysis with alteplase (0.9 mg/kg, maximum 90 mg; 10% as bolus, remainder over 60 minutes) or tenecteplase (0.25 mg/kg IV bolus, maximum 25 mg — now preferred in many centres for ease of administration). The treatment window is ≤4.5 hours from symptom onset (the 4.5-hour boundary is for tenecteplase/alteplase in eligible patients without major contraindications). Before thrombolysis, blood pressure must be brought below 185/110 mmHg and maintained below 180/105 mmHg during and after the infusion — because uncontrolled hypertension increases the risk of haemorrhagic transformation. Absolute contraindications include: haemorrhage on NCCT, active bleeding, prior intracranial haemorrhage, ischaemic stroke within 3 months, major surgery within 14 days, INR >1.7 or use of anticoagulants, platelet count <100,000/mm³, blood glucose <50 or >400 mg/dL, and NIHSS >25 (relative). For eligible patients with proximal large-vessel occlusion (ICA, M1 MCA, basilar), mechanical thrombectomy (endovascular clot retrieval) is the preferred reperfusion strategy within 6 hours of onset (and up to 24 hours in selected patients with favourable penumbra-core mismatch on perfusion imaging, based on the DAWN and DEFUSE-3 trials).
General supportive care applies to all stroke types and runs in parallel with specific reperfusion therapy:
- Airway, breathing, circulation: maintain oxygen saturation ≥94%; intubation if GCS ≤8 or airway compromise
- Blood pressure: in ischaemic stroke without thrombolysis, permissive hypertension (allow up to 220/120 mmHg) for the first 24–48 hours preserves penumbral perfusion; do NOT lower aggressively. In ICH, the target is systolic <140 mmHg (based on INTERACT-2 and ATACH-2 trials)
- Blood glucose: maintain 140–180 mg/dL; both hyperglycaemia (expands infarct) and hypoglycaemia (mimics and worsens stroke) must be actively managed
- Temperature: treat fever (>37.5°C) with paracetamol; fever worsens outcome in stroke
- Antiplatelet therapy: aspirin 300 mg loading dose (if thrombolysis not given, and after 24-hour NCCT to exclude haemorrhagic transformation) is the standard antiplatelet initiation; dual antiplatelet (aspirin + clopidogrel) for 21 days is preferred in minor ischaemic stroke and high-risk TIA
- Anticoagulation: NOT given acutely in most ischaemic stroke (risk of haemorrhagic transformation); indicated in AF-related stroke after a delay based on infarct size (typically 2–14 days)
Haemorrhagic stroke — halt expansion, manage pressure:
For intracerebral haemorrhage, there is no equivalent of thrombolysis — the goal is to stop haematoma expansion and control intracranial pressure. Immediate reversal of anticoagulation is mandatory (vitamin K + prothrombin complex concentrate for warfarin; reversal agents for DOACs where available). Surgical evacuation is considered for specific indications (discussed in the Stroke Acute Management SDL): cerebellar ICH >3 cm with neurological deterioration, obstructive hydrocephalus, and selected lobar ICH in younger patients. Decompressive craniectomy for malignant MCA infarction (large MCA territory infarct with cerebral oedema causing herniation, typically in patients <60 years) is life-saving in selected cases.
Self-Assessment: Stroke Foundations
You have now covered the vascular anatomy of the brain and its clinical implications for stroke localisation, the pathological and aetiological classification of stroke (TOAST subtypes for ischaemic stroke, ICH subtypes, and SAH), the key risk factors and their pathogenic mechanisms, the ischaemic penumbra concept and its therapeutic implications, and the initial clinical approach including the NIHSS and the role of non-contrast CT. The following scenarios test your integration of these foundations.
Provided image
Scenario A: A 70-year-old man presents with sudden onset of right arm and leg weakness, right facial droop, and inability to speak — he opens his mouth but produces no intelligible words, although he seems to understand simple commands. His BP is 196/108 mmHg. NCCT brain shows a hyperdense right MCA sign. What is the most likely stroke type, the likely TOAST subtype, and the immediate management priority?
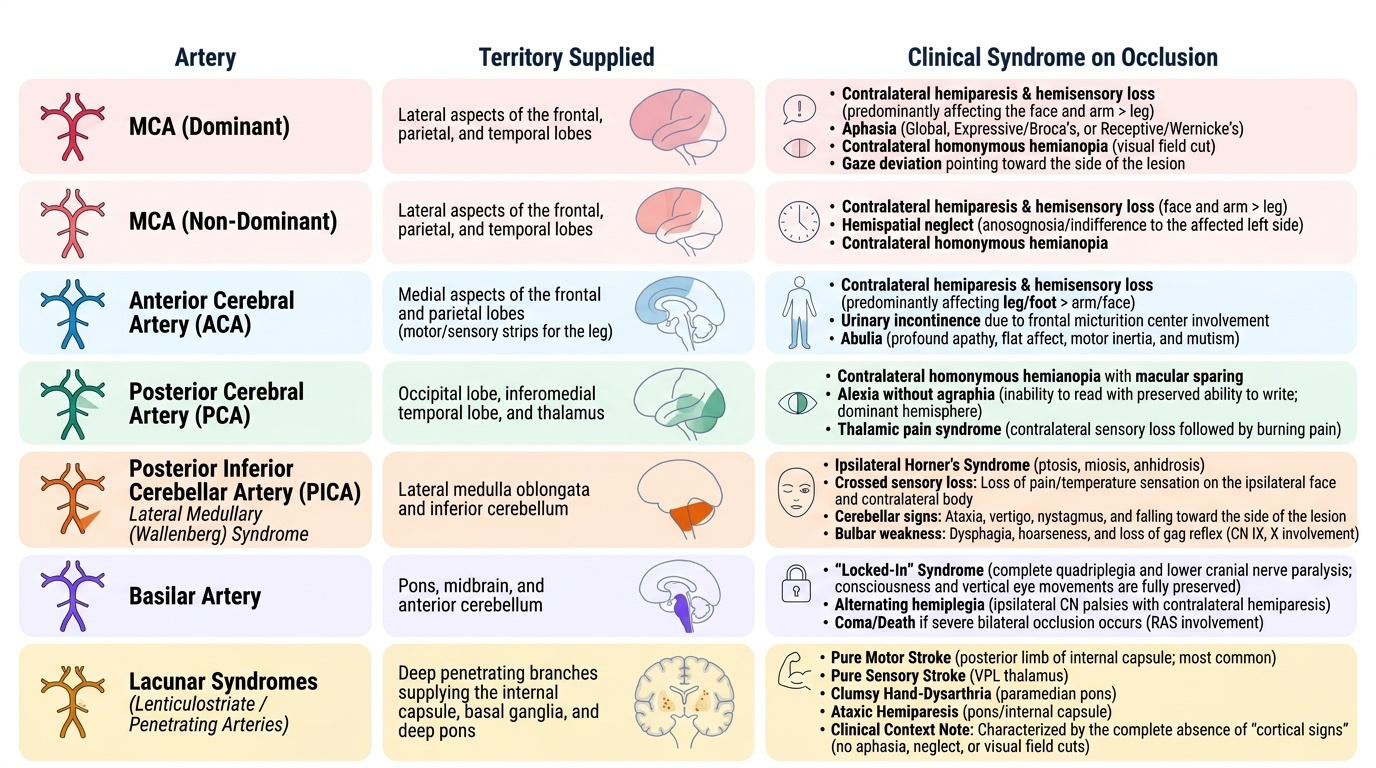
Analysis: Right hemisphere MCA territory stroke — but wait: if the MCA sign is on the RIGHT side, the infarct will cause LEFT-sided weakness; the patient has RIGHT-sided weakness. Therefore, the infarct must be in the LEFT MCA territory. Left MCA stroke explains right hemiplegia AND Broca's aphasia (posterior inferior frontal gyrus = Broca's area, left hemisphere). The hyperdense MCA sign confirms thrombus in the proximal left MCA. TOAST subtype: given age and hypertension with a large artery sign, either large artery atherosclerosis or cardioembolism is most likely — cardiac workup (ECG, echocardiogram) is mandatory to distinguish. Immediate priority: confirm BP <185/110 mmHg, exclude haemorrhage on NCCT (already done — no haemorrhage), check blood glucose, activate stroke team for thrombolysis assessment.
Scenario B: A 45-year-old woman with no known cardiovascular risk factors develops acute onset of severe vertigo, inability to walk (falls to the right), right facial numbness, and hoarseness. Her BP is 140/88 mmHg. NCCT brain is normal. What vascular territory is affected, and what syndrome does she have?
Analysis: The combination of ipsilateral facial numbness + contralateral body numbness (spinothalamic decussation level) + ipsilateral limb ataxia + dysarthria + hoarseness (IX/X involvement) + Horner syndrome (if present) = Wallenberg syndrome (lateral medullary syndrome) from PICA occlusion. The normal NCCT is expected — posterior fossa infarcts are often not visible on CT (bone artefact). MRI DWI would show the lateral medullary infarct. TOAST subtype in a 45-year-old with normal NCCT: consider vertebral artery dissection (spontaneous or post-trauma) as a priority — 'other determined aetiology'.