Page 1 of 14
IM19.1-2 | Movement Disorder Foundations — SDL Guide
Learning Objectives
- Describe the functional neuroanatomy of the basal ganglia and locomotor system relevant to movement disorders
- Explain the direct and indirect pathways through the basal ganglia and how their disruption produces hypokinetic versus hyperkinetic disorders
- Classify movement disorders based on phenomenology: distribution, rhythm, repetition, activation, and exacerbating/relieving factors
- Distinguish resting tremor, postural tremor, and intention tremor by activation condition and clinical significance
- Apply the classification framework to recognise hypokinetic disorders (parkinsonism) versus hyperkinetic disorders (chorea, dystonia, myoclonus, tics)
INSTRUCTIONS
Movement disorders represent a spectrum of neurological conditions in which voluntary motor control is disrupted — not by weakness, sensory loss, or cerebellar disease, but by dysfunction of the circuits that modulate, initiate, or suppress movement. The basal ganglia lie at the heart of this circuitry. A clear mental model of normal basal ganglia function makes every movement disorder logically predictable from the anatomy rather than a list to memorise. This module builds that model, then introduces the phenomenological classification that brings order to a clinically diverse group of conditions.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 431 — Movement Disorders (textbook)
- API Textbook of Medicine, 10th ed., Ch. — Extrapyramidal Disorders (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 28 — Neurological disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mr Rajan, a 62-year-old retired schoolteacher, is brought to the neurology outpatient department by his son. The son describes a three-year history of his father's hands shaking when he sits still — the tremor disappears completely when Rajan reaches for his cup of tea. He walks slowly, takes tiny steps, and has fallen twice in the past six months. His handwriting has become very small. On examination there is a coarse, regular pill-rolling tremor at rest in both hands, cogwheel rigidity at the wrists, and a slow, shuffling gait with reduced arm swing. The tremor stops the moment his hand is in motion. Now contrast this with Mrs Meena, a 28-year-old woman referred for involuntary dance-like flinging movements of her limbs that she cannot suppress. The movements are irregular, non-repetitive, unpredictable — jerking randomly from one muscle group to another. She was recently treated for a sore throat. These two patients share the label 'movement disorder', yet their phenomenology, anatomy, and underlying mechanisms are worlds apart. The key to telling them apart is understanding what the normal basal ganglia circuit does — and what happens when it breaks.
WHY THIS MATTERS
Movement disorders account for a significant proportion of neurology outpatient consultations in India. Parkinson's disease alone affects an estimated 5.8 million people in India (2016 Global Burden of Disease data), and its prevalence is rising with an ageing population. Beyond Parkinson's, the Indian clinician must be alert to conditions with very different prevalences and implications here: rheumatic chorea (Sydenham's chorea) remains a consequence of inadequately treated streptococcal pharyngitis and acute rheumatic fever; Wilson's disease is more common in South Asia due to founder-effect mutations; drug-induced movement disorders from long-term antipsychotic use (especially older first-generation agents) are an important iatrogenic category. The NMC IM19 competency group requires you to describe the neuroanatomy of the locomotor system and classify movement disorders by distribution, rhythm, repetition, and exacerbating/relieving factors — precisely the clinical skills needed to navigate this diverse group.
RECALL
Before proceeding, activate your prior knowledge of motor pathways. The upper motor neuron (UMN) originates in the primary motor cortex (precentral gyrus) and descends via the corticospinal (pyramidal) tract to synapse on lower motor neurons (LMN) in the anterior horn of the spinal cord. UMN lesions produce weakness, spasticity (velocity-dependent increased tone), hyperreflexia, and an extensor plantar response. LMN lesions produce flaccid weakness, wasting, fasciculations, and reduced reflexes. Movement disorders of the extrapyramidal system — the basal ganglia and their circuits — produce a distinct type of motor dysfunction: tone is altered (rigidity rather than spasticity), strength is relatively preserved, and the primary abnormality is in the quality, speed, or regulation of voluntary and involuntary movement. Cerebellar disorders produce yet another pattern: intention tremor, dysmetria, ataxic gait, and dysarthria. Keeping these three systems distinct (pyramidal, extrapyramidal, cerebellar) is the anatomical scaffold for this module.
Functional Neuroanatomy of the Locomotor System
The basal ganglia are a group of subcortical nuclei that form the core of the extrapyramidal motor system. They do not initiate movement directly but act as modulators of cortical motor output, controlling the selection, initiation, scaling, and suppression of movements. A working knowledge of their anatomy is essential, because every major movement disorder can be understood as the consequence of dysfunction at a specific node or pathway within this circuit.
The five principal nuclei of the basal ganglia are the caudate nucleus, the putamen, the globus pallidus (divided into internal segment [GPi] and external segment [GPe]), the subthalamic nucleus (STN), and the substantia nigra (divided into pars compacta [SNc] and pars reticulata [SNr]). The striatum refers collectively to the caudate and putamen, and is the principal input nucleus of the basal ganglia — it receives excitatory glutamatergic projections from virtually the entire cortex as well as dopaminergic input from the substantia nigra pars compacta. The GPi and SNr together constitute the output nuclei of the basal ganglia; they project to the thalamus (ventral anterior and ventrolateral nuclei), which in turn projects back to the supplementary motor area and premotor cortex, completing the cortico-striato-thalamo-cortical loop.
The internal circuitry of the basal ganglia operates through two opposing pathways:
Direct pathway: Cortex → Striatum → GPi/SNr. The striatum sends GABAergic (inhibitory) projections directly to the GPi. Since the GPi tonically inhibits the thalamus (GABAergic output from GPi → thalamus), activation of the direct pathway disinhibits the thalamus — ultimately facilitating movement. Dopamine from the SNc acts on D1 receptors in the striatum to reinforce this pathway.
Indirect pathway: Cortex → Striatum → GPe → STN → GPi/SNr. The striatum inhibits GPe, which normally inhibits the STN. When the indirect pathway is activated, GPe inhibition is released from GPe, the STN is activated, and the STN sends excitatory projections to GPi — increasing GPi output and thus further inhibiting thalamic activity. This pathway suppresses movement. Dopamine acts on D2 receptors in the striatum to inhibit the indirect pathway.
The net effect of dopamine via both pathways is to facilitate movement — dopamine simultaneously facilitates the direct pathway (via D1) and suppresses the indirect pathway (via D2). This is why loss of dopaminergic neurons in the SNc — as in Parkinson's disease — simultaneously reduces direct pathway activation and disinhibits the indirect pathway, producing excessive GPi output and profound thalamic inhibition. The clinical result is hypokinesia — difficulty initiating and executing movement.
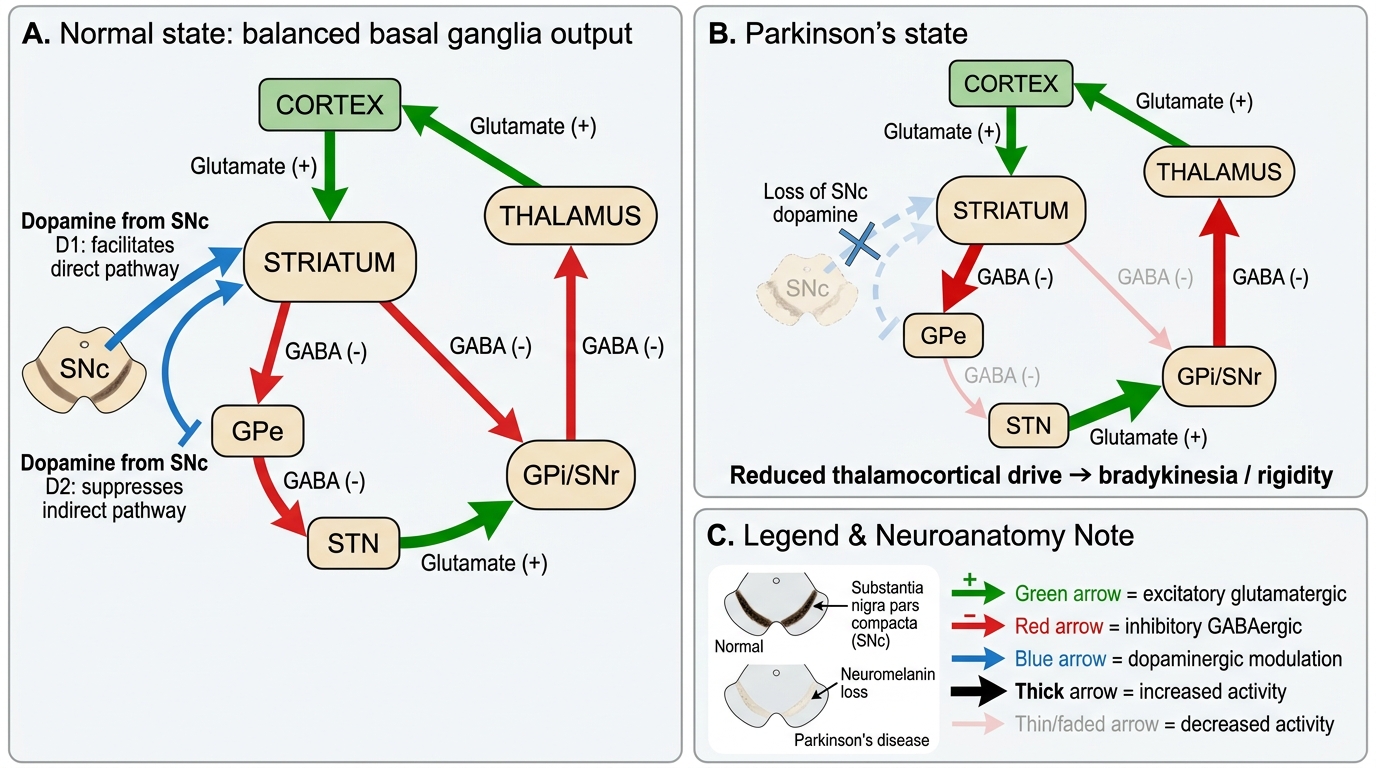
Basal Ganglia Direct and Indirect Pathways in Parkinson's Disease
Beyond the striatum, several other neuroanatomical structures are relevant to movement disorders. The substantia nigra is the pigmented midbrain structure that gives rise to the nigrostriatal dopaminergic pathway (the A9 dopamine system). Neuromelanin pigment in SNc neurons is visible macroscopically and is reduced in Parkinson's disease (loss of the normal black pigmentation of the substantia nigra). The locus coeruleus (noradrenergic) and raphe nuclei (serotonergic) are also affected in Parkinson's disease, explaining non-motor symptoms. The cerebellum interacts with basal ganglia circuitry via cerebellar-thalamic-cortical loops; cerebellar output nuclei project to the ventrolateral thalamus. Disruption of these cerebellar connections produces a different movement disorder phenotype (intention tremor, ataxia) that is distinguishable from basal ganglia disease.
Pathophysiological Basis: How Circuit Disruption Produces Movement Disorder
Understanding the pathophysiology of movement disorders requires translating the circuit anatomy above into predictable clinical manifestations. The basal ganglia circuit model, originally proposed by DeLong in 1990 and subsequently refined, explains how the same circuit disrupted at different nodes produces clinically opposite syndromes — hypokinesia or hyperkinesia.
Hypokinetic disorders arise when the net output from the basal ganglia to the thalamus is excessive inhibition — suppressing the thalamo-cortical facilitation of movement. In the circuit, this means the GPi is overactive, sending excessive inhibitory GABA to the thalamus. The primary mechanism in Parkinson's disease is loss of SNc dopaminergic neurons, which leads to simultaneous underactivation of the direct pathway (which normally disinhibits thalamus) and overactivation of the indirect pathway (which additionally inhibits thalamus via STN excitation of GPi). The clinical result is the parkinsonian syndrome — characterised by the cardinal features abbreviated as TRAP: Tremor at rest (4–6 Hz, pill-rolling, asymmetric, suppressed by voluntary movement), Rigidity (lead-pipe or cogwheel, present throughout range of motion, velocity-independent — distinguishing it from UMN spasticity), Akinesia/bradykinesia (slowness and poverty of movement — impaired initiation, reduced amplitude, fatiguing), and Postural instability (loss of postural reflexes, leading to falls). Bradykinesia is the cardinal motor feature required for the diagnosis.
IMPORTANT DISTINCTION: Parkinson's disease (PD) is an idiopathic neurodegenerative condition (Lewy body pathology, alpha-synuclein aggregation). Parkinsonism is the clinical syndrome of TRAP features from any cause — and can arise from many aetiologies beyond PD. The term Parkinson-plus refers to neurodegenerative conditions that mimic PD but have additional features and do not respond to levodopa: progressive supranuclear palsy (PSP — falls, vertical gaze palsy, axial rigidity), multiple system atrophy (MSA — parkinsonism + autonomic failure + cerebellar), corticobasal syndrome (CBS — asymmetric limb rigidity, apraxia, alien limb), and dementia with Lewy bodies (DLB — parkinsonism + cognitive fluctuations + visual hallucinations + REM sleep behaviour disorder).
Hyperkinetic disorders arise when the net basal ganglia output is reduced inhibition of the thalamus — allowing excessive, unwanted thalamo-cortical excitation. In the circuit, GPi underactivity releases thalamic inhibition, producing abnormal, involuntary movements. Crucially, hyperkinetic disorders are not all the same — they differ in their involuntary movement phenomenology, and this phenomenology maps to distinct neuroanatomical substrates.
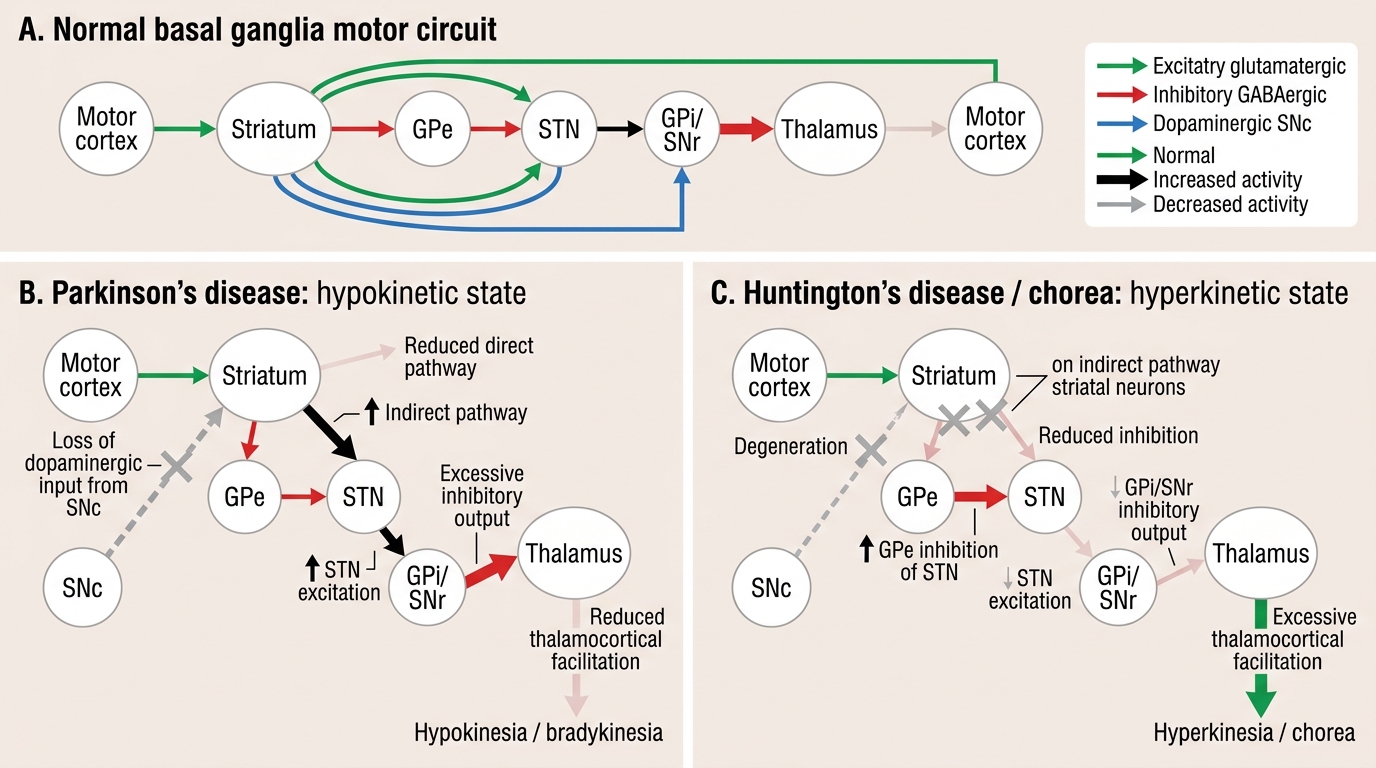
Hypokinetic vs Hyperkinetic Basal Ganglia Circuit States
Classification of Movement Disorders
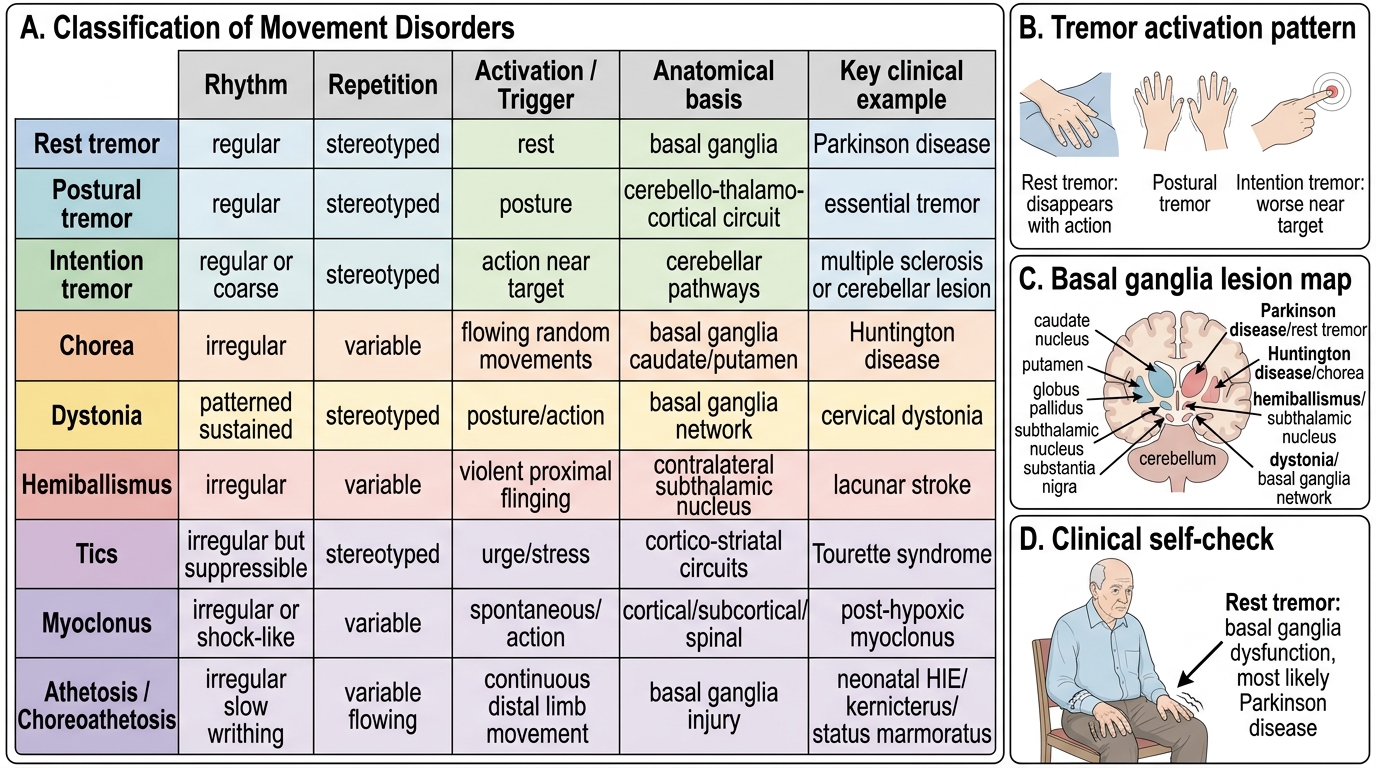
Movement disorders are classified by their phenomenology — what the movement looks like, when it occurs, and what modifies it. This classification is clinically powerful because the phenomenological features guide the anatomical localisation and differential diagnosis before any investigations are ordered. The classification framework uses five axes: distribution (focal, segmental, generalised, hemibody), rhythm (regular vs irregular), repetition (stereotyped and repetitive vs variable and non-repetitive), activation (at rest vs during posture vs during action), and exacerbating and relieving factors (stress, voluntary movement, sleep, distraction, sensory tricks).
The major phenomenological categories are as follows:
Tremor is a rhythmic, oscillatory, involuntary movement produced by alternating contractions of antagonist muscle groups. It is the commonest movement disorder. Tremor classification by activation condition is clinically crucial:
- Rest tremor: present when the affected limb is fully supported and not engaged in voluntary activity; disappears or diminishes with voluntary movement. The classic example is the pill-rolling tremor of Parkinson's disease — 4–6 Hz, coarse, asymmetric at onset. The disappearance with action distinguishes it from other tremors.
- Postural tremor: present when the limb is maintained against gravity (e.g., arms outstretched). The prototypic example is essential tremor — 6–12 Hz, symmetric, affects hands/arms bilaterally, often with family history, classically relieved by alcohol. Physiological tremor (fine, high frequency, seen in anxiety, hyperthyroidism, stimulants, beta-agonists) is also postural. Orthostatic tremor (high frequency leg tremor on standing) is a distinct variant.
- Intention (kinetic) tremor: tremor that worsens as the limb approaches a target during voluntary movement (e.g., finger-nose test). This implicates cerebellar dysfunction or cerebellar connections — it is NOT a basal ganglia tremor. Associated with dysmetria and past-pointing.
- Task-specific tremor: only present during a specific task (e.g., writing tremor is a focal task-specific tremor).
Chorea is composed of random, irregular, non-repetitive, flowing, 'dance-like' movements that appear to move from one body part to another unpredictably, as if the patient is incorporating them into semi-purposeful movements (parakinesias). Chorea arises from reduced GPi output with thalamic disinhibition. Important causes include Huntington's disease (autosomal dominant CAG repeat expansion in HTT gene; progressive chorea + psychiatric + dementia), Sydenham's chorea (rheumatic; post-streptococcal, reversible, often in children; associated with acute rheumatic fever), drug-induced chorea (dopaminergic drugs, oral contraceptive pill, phenytoin), and metabolic chorea (thyrotoxicosis, pregnancy — chorea gravidarum, SLE — anti-phospholipid antibody, polycythaemia vera).
Dystonia is sustained or intermittent muscle contractions producing abnormal, repetitive twisting movements or abnormal postures. It is often worse with voluntary movement (action dystonia) and can be relieved by sensory tricks (geste antagoniste, e.g., touching the chin relieves cervical dystonia). The distribution can be focal (e.g., blepharospasm — involuntary eye closure; writer's cramp — hand dystonia during writing; cervical dystonia/torticollis — head/neck twisting), segmental, or generalised. Important causes: genetic (DYT1 gene in primary generalised dystonia), secondary (Wilson's disease, cerebral palsy, basal ganglia lesions, tardive dystonia).
Hemiballismus is a violent, large-amplitude, unilateral flinging movement of the proximal limb, most commonly caused by a lesion (typically a vascular lacunar infarct) in the contralateral subthalamic nucleus (STN). Loss of STN excitation of GPi leads to GPi underactivity → disinhibition of thalamus → uninhibited cortical motor discharge. This is a direct anatomical-clinical correlation of the circuit model.
Tics are brief, stereotyped, repetitive movements (motor tics) or sounds (vocal tics) that the patient can temporarily suppress with effort (associated with premonitory urge). They wax and wane spontaneously. Tourette syndrome = multiple motor tics + at least one vocal tic for >1 year before age 18. Tics are NOT rhythmic (distinguishing from tremor) and NOT as random as chorea.
Myoclonus is sudden, brief, shock-like, involuntary muscle jerks arising from a sudden burst of muscle electrical activity. It may be cortical (e.g., cortical myoclonus in epilepsy), subcortical, spinal, or peripheral in origin. Causes include metabolic encephalopathy (uraemia, hepatic failure — asterixis is a form of negative myoclonus), post-anoxic injury (Lance-Adams syndrome), and familial progressive myoclonic epilepsies.
Classification of Movement Disorders
Athetosis refers to slow, writhing, continuous, flowing movements, often with alternating flexion/extension and pronation/supination — particularly affecting the distal limbs. It frequently co-occurs with chorea (choreoathetosis). The classical association is with basal ganglia damage in the neonatal period (e.g., hypoxic-ischaemic encephalopathy, kernicterus from bilirubin encephalopathy affecting the basal ganglia — termed status marmoratus).
SELF-CHECK
A 62-year-old man has a coarse tremor of his right hand that is most prominent when he sits quietly with his hand resting in his lap. When he reaches forward to pick up a glass, the tremor disappears completely. Which type of tremor is this and what does it implicate?
A. Intention tremor — cerebellar pathway dysfunction
B. Postural tremor — essential tremor or enhanced physiological tremor
C. Rest tremor — basal ganglia dysfunction, most likely Parkinson's disease
D. Task-specific tremor — focal occupational dystonia
Reveal Answer
Answer: C. Rest tremor — basal ganglia dysfunction, most likely Parkinson's disease
Rest tremor is present when the limb is fully relaxed and supported, and characteristically decreases or disappears with voluntary movement (re-emergence of tremor is possible with sustained posture in PD but the key feature is its suppression during the initial phase of voluntary action). This contrasts with intention tremor (worsens as the limb approaches a target — cerebellar) and postural tremor (persists with sustained posture, typical of essential tremor). Rest tremor implicates basal ganglia — specifically dopaminergic nigrostriatal pathway dysfunction — and is the classic tremor of Parkinson's disease.