Page 12 of 24
IM2.{14-16,19-20,23} | ACS Acute Management — SDL Guide (Part 2)
Management: CCU Supportive Care, Analgesia, and Pharmacotherapy
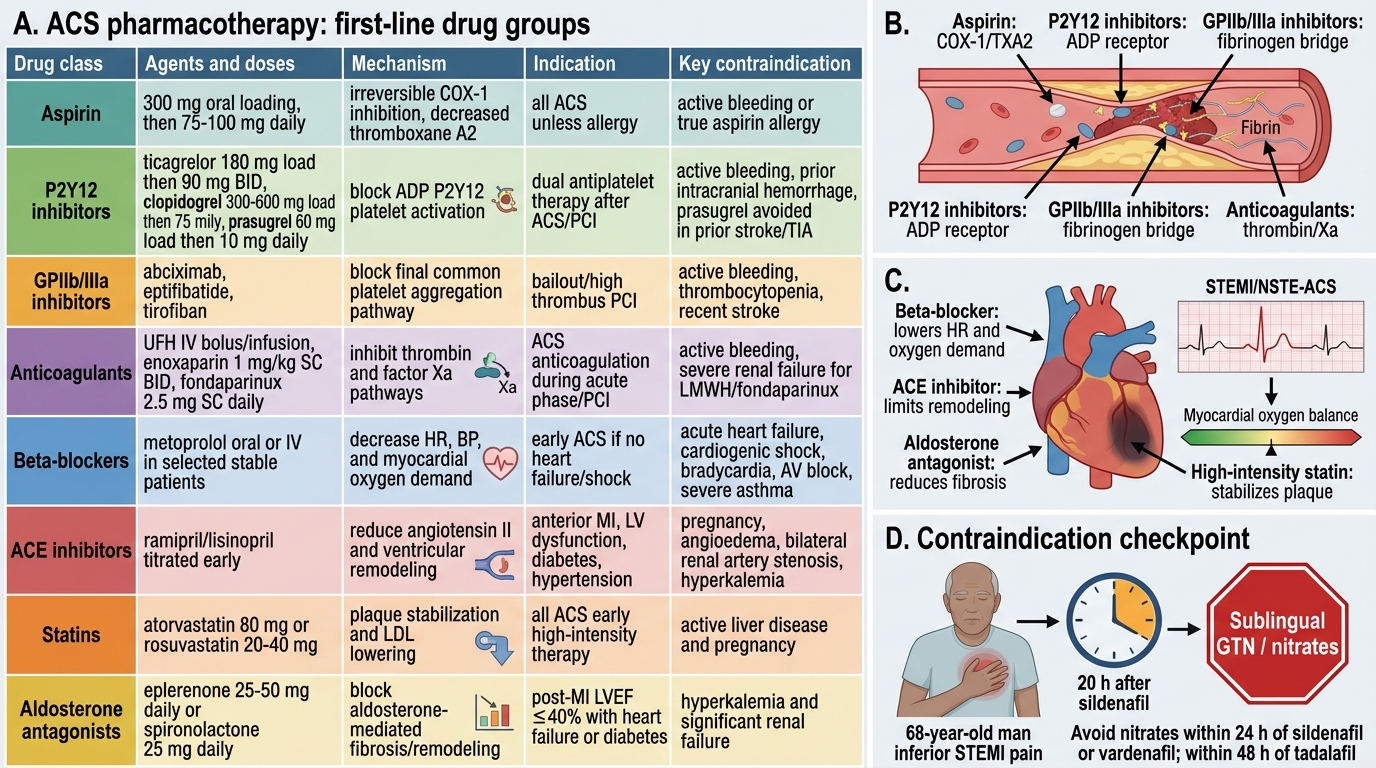
The pharmacological management of ACS is best understood through five therapeutic layers: (1) analgesia and haemodynamic support; (2) antiplatelet therapy; (3) anticoagulation; (4) pharmacological cardioprotection; and (5) reperfusion therapy. Each layer has a specific rationale, defined drug choices, and important contraindications. The 'MONA' mnemonic (Morphine, Oxygen, Nitrates, Aspirin) is a teaching aid but is outdated in its original form — current evidence has modified the role of oxygen and morphine. The accurate framework is presented here.
1. Analgesia and haemodynamic support:
Morphine (2–4 mg IV, titrated in 2 mg increments every 5 minutes): the gold standard for ischaemic chest pain relief. Mechanism: μ-opioid receptor agonist → analgesia + venodilation (reduces LV preload) + reduction of sympathetic activation (reduces HR and myocardial oxygen demand). Important caveat from CRUSADE and EARLY-ACS registry data: morphine in NSTEMI is associated with delayed P2Y12 inhibitor absorption (opioid effect on gastric motility) and potentially worse outcomes in some analyses. Current ESC 2023 guidance: morphine remains appropriate for severe pain (ischaemic chest pain NRS ≥7) but use the lowest effective dose and consider the P2Y12 oral absorption interaction. Nausea management: IV metoclopramide or ondansetron alongside morphine. Avoid NSAIDS in the acute MI phase — they increase platelet aggregability and impair myocardial healing.
Oxygen: routine high-flow oxygen is NOT indicated in normoxic ACS patients (AVOID-STEMI, DETO2X-AMI trials showed no benefit and possible harm from oxygen in patients with SpO2 ≥94%). Oxygen should be administered only when SpO2 <94% (target 94–98%), in patients with breathlessness, or in cardiogenic shock. Hyperoxia causes coronary vasoconstriction and increases infarct size — this is the opposite of the intuitive expectation.
Nitrates (glyceryl trinitrate/nitroglycerine): venodilation (preload reduction) and coronary vasodilation. Sublingual GTN 0.4 mg (or isosorbide dinitrate 5 mg sublingual) provides rapid relief within 2–3 minutes. IV GTN infusion (5–200 mcg/min, titrated) is used for persistent pain, acute LV failure, and hypertensive ACS. Critical contraindications to nitrate: (a) SBP <90 mmHg (causes catastrophic hypotension — already vasodilated); (b) inferior STEMI with suspected RV infarction (nitrate causes hypotension by reducing RV preload — give IV fluids first); (c) recent PDE5 inhibitor use (sildenafil, tadalafil, vardenafil) — within 24 hours for sildenafil/vardenafil, 48 hours for tadalafil — produces life-threatening hypotension by synergistic cGMP accumulation.
2. Antiplatelet therapy (dual antiplatelet therapy — DAPT):
Aspirin (acetylsalicylic acid): the anchor antiplatelet in all ACS. Mechanism: irreversible COX-1 inhibition → block thromboxane A2 synthesis → reduced platelet aggregation. Loading dose: 300 mg non-enteric-coated (chewed or crushed for rapid absorption) at presentation. Maintenance: 75–100 mg daily indefinitely. Contraindicated in active bleeding or documented severe aspirin allergy (rare — true allergy requires desensitisation or clopidogrel monotherapy).
P2Y12 receptor inhibitors — given in addition to aspirin (DAPT) in all ACS patients without contraindication:
- Ticagrelor (180 mg loading, then 90 mg BD): preferred P2Y12 inhibitor in ACS (PLATO trial — superior to clopidogrel in reducing cardiovascular death + MI + stroke). Reversible ADP receptor antagonist; rapid onset (30 min). Contraindications: prior intracranial haemorrhage, active significant bleeding, concomitant strong CYP3A4 inhibitors (clarithromycin, ketoconazole). Adverse effect: dyspnoea (in ~15% — transient, mechanism unclear; does not indicate bronchospasm; rarely requires discontinuation).
- Clopidogrel (300 mg loading in NSTE-ACS; 600 mg loading for PCI; 75 mg daily maintenance): pro-drug requiring hepatic conversion to active metabolite (CYP2C19). Slower onset than ticagrelor. Acceptable alternative when ticagrelor is contraindicated or unavailable. CYP2C19 poor metabolisers (common in South and East Asian populations — ~30%) have reduced antiplatelet effect with clopidogrel — genetic testing is recommended before clopidogrel use in PCI if ticagrelor is an option.
- Prasugrel (60 mg loading, 10 mg daily maintenance): faster and more potent than clopidogrel; approved for STEMI patients undergoing primary PCI (TRITON-TIMI 38); contraindicated in prior stroke/TIA, age >75, or weight <60 kg (bleeding risk).
DAPT duration: minimum 12 months after ACS with stenting; duration may be extended to 24–36 months if ischaemic risk high and bleeding risk low (DAPT trial); may be shortened to 3–6 months if bleeding risk is elevated (based on PRECISE-DAPT score).
GPIIb/IIIa inhibitors (abciximab, eptifibatide, tirofiban): block the final common pathway of platelet aggregation — fibrinogen binding to GPIIb/IIIa receptor. Most potent antiplatelet agents available. Current role: limited by era of modern potent oral P2Y12 inhibitors; used mainly as bailout in high-thrombus-burden STEMI undergoing PCI, or in high-risk NSTE-ACS undergoing PCI who did not receive adequate oral P2Y12 preloading. Not indicated for routine pre-PCI treatment (EARLY-ACS, ACUITY trials).
3. Anticoagulation:
Unfractionated heparin (UFH): IV bolus 60 units/kg (max 4000 units) followed by infusion 12 units/kg/h (max 1000 units/h), titrated to APTT 50–75 seconds (1.5–2× control). Standard anticoagulant for STEMI patients undergoing primary PCI. Monitor APTT 6-hourly. Advantage: reversible with protamine sulphate.
Low-molecular-weight heparin (LMWH) — enoxaparin: 1 mg/kg SC every 12 hours. More predictable pharmacokinetics than UFH (no need for APTT monitoring in most patients); at least equivalent to UFH in NSTE-ACS (ExTRACT-TIMI 25 trial for STEMI). Renally cleared — dose-reduce in CKD (eGFR 15–30 mL/min: 1 mg/kg once daily; avoid in eGFR <15). Partially reversible with protamine (60–70% anti-Xa activity neutralised).
Fondaparinux (selective factor Xa inhibitor, 2.5 mg SC once daily): recommended as first-choice anticoagulant in NSTE-ACS by ESC 2023 guidelines (OASIS-5 trial showed equivalent efficacy to enoxaparin with lower major bleeding). Do NOT use as sole anticoagulant during PCI — risk of catheter thrombus; supplement with UFH intra-procedurally.
Bivalirudin (direct thrombin inhibitor): reserved for PCI in patients with heparin-induced thrombocytopaenia (HIT) as alternative to UFH.
4. Pharmacological cardioprotection:
Beta-blockers (metoprolol succinate 25–50 mg oral, or metoprolol tartrate 5 mg IV × 3 doses for hypertensive tachycardic STEMI): reduce myocardial oxygen demand (HR reduction is the primary benefit), suppress arrhythmias (VT/VF prevention), reduce infarct size. Initiate oral beta-blocker within 24 hours if no contraindications. IV beta-blocker only if persistent hypertension, tachycardia, or ongoing ischaemia despite oral loading. Absolute contraindications to beta-blocker in acute MI: cardiogenic shock (Killip IV), acute decompensated heart failure (significant pulmonary oedema), severe bradycardia (HR <60), second or third-degree AV block, reactive airways disease (severe asthma — relative contraindication; COPD with reactive component).
ACE inhibitors/ARBs: initiated within 24 hours if LVEF ≤40%, anterior MI, hypertension, or diabetes. Reduce LV remodelling (dilation and wall thinning of the infarcted zone) by blocking angiotensin II-mediated fibrosis. Ramipril (2.5 mg BD titrated up), lisinopril (5 mg OD), or enalapril. Demonstrated survival benefit in STEMI: SAVE, AIRE, TRACE trials. ARBs (valsartan, losartan) are equivalent for patients intolerant of ACE inhibitors (dry cough). Contraindications: hypotension (SBP <100 mmHg), bilateral renal artery stenosis, serum potassium >5.5 mmol/L, pregnancy.
Statins (high-intensity): initiated immediately on admission regardless of baseline LDL (A-to-Z, MIRACL trials). Pleiotropic benefits in ACS beyond LDL reduction: anti-inflammatory, plaque-stabilising, endothelial-protective effects evident within days. Atorvastatin 40–80 mg or rosuvastatin 20–40 mg as first-line.
Aldosterone antagonists (eplerenone 25–50 mg daily; spironolactone as alternative): indicated in post-MI patients with LVEF ≤40% plus either heart failure symptoms OR diabetes. EPHESUS trial: eplerenone started within 3–14 days of MI reduced all-cause mortality by 15% in this population. Contraindication: serum creatinine >2.5 mg/dL in men or >2.0 mg/dL in women, potassium >5.0 mmol/L.
ACS Pharmacotherapy Summary and Contraindication Checkpoint
SELF-CHECK
A 68-year-old man presents with an inferior STEMI. He took sildenafil 25 mg approximately 20 hours ago for erectile dysfunction. His BP is 120/80 mmHg, HR 85/min, and he has no signs of heart failure. He is in pain (NRS 8/10). Which drug is CONTRAINDICATED in this patient RIGHT NOW?
A. Aspirin 300 mg oral loading dose
B. Sublingual glyceryl trinitrate (GTN) 0.4 mg
C. IV morphine 2 mg titrated
D. Unfractionated heparin IV bolus
Reveal Answer
Answer: B. Sublingual glyceryl trinitrate (GTN) 0.4 mg
Nitrates are absolutely contraindicated within 24 hours of sildenafil or vardenafil use (and within 48 hours of tadalafil). Both nitrates and PDE5 inhibitors increase intracellular cGMP — nitrates via cGMP generation, PDE5 inhibitors by blocking cGMP breakdown. Their combination causes massive synergistic vasodilatation and can produce catastrophic, refractory hypotension. The patient took sildenafil 20 hours ago, which is within the 24-hour contraindication window. His pain should be managed with IV morphine instead. Aspirin and heparin are both appropriate and indicated now. Once 24 hours have elapsed from sildenafil use, nitrates can be cautiously administered.
Reperfusion Therapy: Thrombolysis, Primary PCI, and CABG
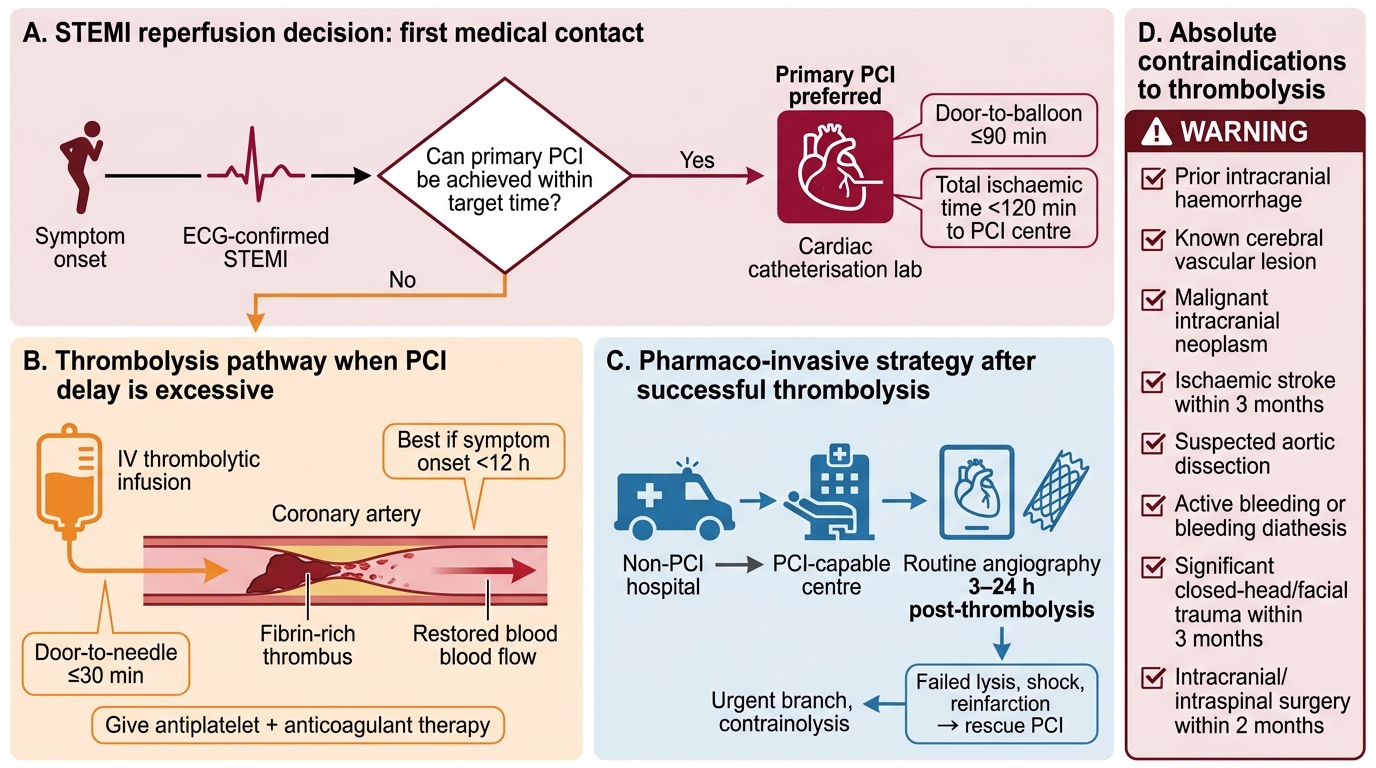
Reperfusion — restoring coronary blood flow in a completely occluded artery — is the most time-critical intervention in STEMI. The principle is simple: every minute of complete coronary occlusion destroys approximately 1 gram of myocardium, and the wavefront of necrosis advances from endocardium to epicardium over 3–6 hours. The therapeutic goal is to restore flow before irreversible infarction is complete. Two reperfusion strategies are available: pharmacological (thrombolysis) and mechanical (primary PCI). The choice between them is determined by the time to achieve reperfusion, local facility availability, and patient-specific contraindications.
Primary Percutaneous Coronary Intervention (Primary PCI):
Primary PCI is the preferred reperfusion strategy for STEMI when it can be performed within 120 minutes of first medical contact (total ischaemic time <12 hours for definite benefit, extending to 24 hours if evidence of ongoing ischaemia). The goal is a door-to-balloon time of ≤90 minutes (time from patient's arrival at the PCI-capable hospital to balloon inflation in the culprit artery). Mechanism: direct mechanical recanalization of the occluded artery using balloon angioplasty and stenting — more complete, faster, and more sustained recanalization than pharmacological thrombolysis. Primary PCI achieves TIMI 3 flow (normal flow) in >90% of arteries, compared to ~50–60% with thrombolytic agents. Drug-eluting stents (DES) — which elute antiproliferative agents (sirolimus, paclitaxel) — are preferred over bare-metal stents (BMS) for primary PCI as they reduce in-stent restenosis rates. Primary PCI also allows simultaneous haemodynamic assessment and treatment of complications.
Indications for primary PCI: (1) Any STEMI or STEMI equivalent (new LBBB) with total ischaemic time <12 hours AND PCI achievable within 120 minutes of first medical contact; (2) Cardiogenic shock complicating STEMI regardless of time since onset — PCI is the only proven survival benefit in this context (SHOCK trial); (3) Failed thrombolysis (ST elevation not reduced by >50% at 60–90 minutes after thrombolysis) → rescue PCI.
Pharmacological Thrombolysis (Fibrinolytic therapy):
Thrombolysis is indicated when primary PCI is NOT available within 120 minutes of first medical contact AND the patient has no absolute contraindications. In India, where most STEMI patients present to non-catheterisation-capable centres, thrombolysis followed by transfer for angiography ('pharmaco-invasive strategy') is the dominant reperfusion approach. The goal is door-to-needle time ≤30 minutes (time from hospital arrival to fibrinolytic infusion).
Fibrinolytic agents available:
- Streptokinase (SK): 1.5 million units IV over 60 minutes; non-fibrin-specific; cheapest; disadvantage — antigenic (prior streptococcal infection or prior SK use produces neutralising antibodies → cannot re-use within 1 year; check for streptococcal antibodies)
- Alteplase (tPA): 15 mg IV bolus, then 0.75 mg/kg over 30 min (max 50 mg), then 0.5 mg/kg over 60 min (max 35 mg); total dose max 100 mg; fibrin-specific; no antigenic concerns
- Tenecteplase (TNK-tPA): single IV bolus, weight-based dosing (0.5 mg/kg, max 50 mg); fibrin-specific; most convenient (single bolus); equivalent to alteplase in ASSENT-2 trial; preferred for pre-hospital thrombolysis
- Reteplase: two 10-unit IV boluses 30 minutes apart
Absolute contraindications to thrombolysis:
- Any prior intracranial haemorrhage
- Known structural intracranial lesion (AVM, tumour)
- Ischaemic stroke within 3 months (except if presenting within 4.5 hours — alteplase for acute ischaemic stroke; this is a separate indication, not a contraindication)
- Significant closed-head or facial trauma within 3 months
- Active bleeding (excluding menses) or bleeding diathesis
- Suspected aortic dissection
- For streptokinase: prior use within 1 year (antigenicity)
Relative contraindications (risk-benefit assessment required):
- Uncontrolled hypertension on presentation (SBP >180 mmHg or DBP >110 mmHg)
- History of chronic severe hypertension
- Ischaemic stroke >3 months prior
- Dementia or intracranial pathology not covered by absolute contraindications
- Traumatic or prolonged CPR (>10 minutes) or major surgery within 3 weeks
- Recent internal bleeding (2–4 weeks)
- Non-compressible vascular puncture (subclavian/jugular vein)
- Pregnancy
- Active peptic ulcer
- Oral anticoagulant use (INR >2.0–3.0 increases haemorrhagic risk)
The pharmaco-invasive strategy — thrombolysis followed by routine transfer for angiography within 3–24 hours (STREAM, TRANSFER-AMI trials) — is recommended for all post-thrombolysis STEMI patients who do not have immediate PCI access. Angiography within this window identifies residual culprit stenosis for PCI after successful thrombolysis ('facilitated PCI') and manages failed thrombolysis with rescue PCI.
Coronary Artery Bypass Grafting (CABG):
CABG is rarely the primary reperfusion strategy in acute STEMI. Indications for CABG in the ACS context: (1) Failed PCI or coronary anatomy not amenable to PCI (left main disease with complex anatomy, three-vessel disease in stable diabetics — FREEDOM trial); (2) Mechanical complications requiring concurrent surgical repair (VSD, free wall rupture, severe papillary muscle rupture requiring mitral valve surgery — CABG can be performed simultaneously); (3) Elective CABG for residual multivessel disease identified after initial PCI for the culprit lesion. CABG carries higher perioperative mortality in the acute MI setting (soft, friable myocardium, haemodynamic instability) and is generally deferred to 3–7 days after stabilisation unless a mechanical complication mandates urgent surgery.
STEMI Reperfusion Strategy Decision Algorithm
SELF-CHECK
A 50-year-old man presents to a district hospital with anterior STEMI 90 minutes after symptom onset. The nearest PCI-capable centre is 3 hours away by ambulance. The patient has no contraindications to thrombolysis. His BP is 150/90 mmHg, and his last ischaemic stroke was 14 months ago. What is the most appropriate reperfusion strategy?
A. Transfer immediately to the PCI centre — primary PCI is always preferred over thrombolysis
B. Thrombolysis (tenecteplase or streptokinase) immediately, followed by transfer for coronary angiography within 3–24 hours (pharmaco-invasive strategy)
C. Watchful waiting with medical management — the 90-minute symptom-to-door time has already elapsed, so reperfusion benefit is minimal
D. CABG at the nearest facility with a cardiac surgical unit
Reveal Answer
Answer: B. Thrombolysis (tenecteplase or streptokinase) immediately, followed by transfer for coronary angiography within 3–24 hours (pharmaco-invasive strategy)
Primary PCI is preferred only when it can be achieved within 120 minutes of first medical contact. The PCI centre is 3 hours (180 minutes) away — well beyond this threshold. With no absolute contraindications (prior ischaemic stroke was 14 months ago, which is beyond the 3-month absolute contraindication; no intracranial haemorrhage history; no aortic dissection; no active bleeding), immediate thrombolysis followed by the pharmaco-invasive strategy (transfer for angiography within 3–24 hours after successful thrombolysis) is the evidence-based approach. The 90-minute symptom duration does not reduce thrombolysis benefit — benefit is substantial up to 6 hours and exists up to 12 hours. Watchful waiting is never the correct answer for an eligible STEMI patient.
Self-Assessment: ACS Management Decision-Making
The self-assessment scenarios in this section present complete ACS cases requiring integration of clinical findings, pharmacological choices, reperfusion decisions, and complication management. Work through each independently before reading the analysis. The cognitive skill being practised is simultaneous processing of multiple management layers — not sequential — because in real clinical care, the medication prescription, reperfusion activation, and complication recognition occur in overlapping rather than sequential steps. This reflects the NMC competency standard at KH level: you must apply ACS management knowledge to patient scenarios with clinical nuance, not merely list drugs in isolation. The scenarios are ordered from the most time-critical (reperfusion decision in STEMI) to the most nuanced (triple therapy in post-MI AF), covering the full range of competencies IM2.14–2.23 at the level of clinical application. For each scenario, explicitly identify the contraindicated drugs before prescribing — the IM known-traps around nitrates, oxygen, and anticoagulation are tested here deliberately.
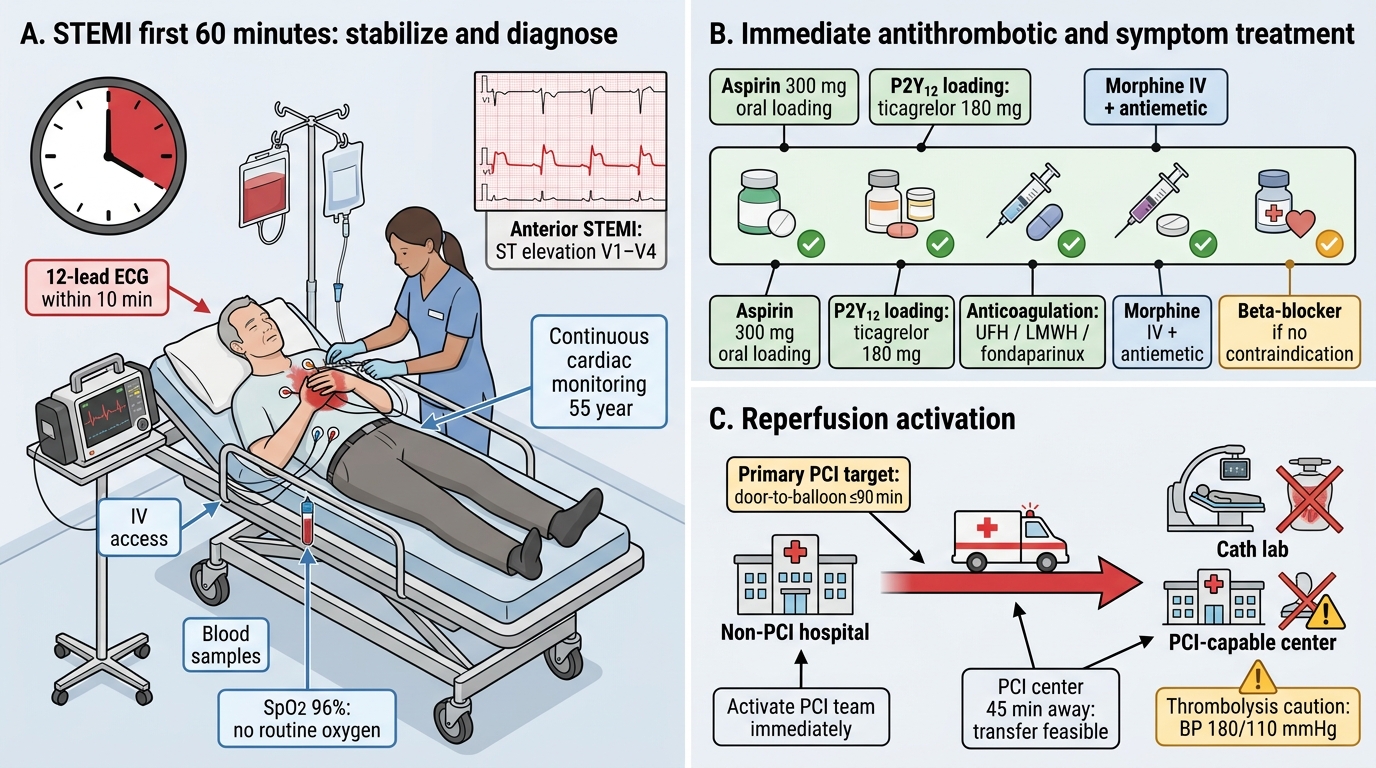
STEMI First 60-Minute Management Bundle
Scenario A: A 55-year-old man is brought in with 1.5 hours of anterior STEMI. BP 180/110 mmHg, HR 100/min, SpO2 96%. He denies any prior stroke, surgery, or bleeding. A PCI-capable centre is 45 minutes away. He has had recent nausea and was given sublingual GTN by the paramedic with no effect. Outline the immediate management bundle.
Analysis: (1) Call PCI centre immediately — activate primary PCI pathway (total door-to-balloon target ≤90 min; 45-min transport + cathlab setup is achievable). (2) Aspirin 300 mg oral (crushed) immediately. (3) Ticagrelor 180 mg oral loading (preferred P2Y12 in STEMI). (4) Unfractionated heparin IV bolus (60 units/kg, max 4000 units) — anticoagulation for PCI. (5) Morphine 2–4 mg IV (GTN has failed, pain is uncontrolled) + metoclopramide 10 mg IV. (6) Oxygen: SpO2 96% → do NOT give routine O2; only if SpO2 falls <94%. (7) BP 180/110 mmHg: thrombolysis is relatively contraindicated (SBP >180); however this patient is going to PCI — uncontrolled hypertension is not a contraindication to PCI. IV metoprolol (5 mg slowly) or IV labetalol can be used for hypertension + tachycardia control if clinically appropriate. (8) No nitrate (GTN failed, no contraindication from sildenafil but prior dose was ineffective — IV GTN may still be considered for pain but is lower priority than analgesia with morphine given the failed sublingual response).
Scenario B: A 66-year-old woman with inferior STEMI (3 hours of symptoms) presents to a rural facility without PCI. BP 85/60 mmHg, HR 55/min, JVP elevated, lung fields clear. ECG shows ST elevation in II/III/aVF and 1-mm ST elevation in right-sided V4R. What is the clinical diagnosis, and how does it change your management compared to standard inferior STEMI management?
Analysis: RV infarction (inferior STEMI + right-sided V4R elevation + hypotension + elevated JVP + clear lungs). Key management differences from standard STEMI: (a) NO nitrates — will cause catastrophic hypotension by reducing RV preload; (b) IV fluid challenge (0.5–1 L normal saline) to increase RV preload and restore cardiac output — this is the single most important immediate intervention; (c) Avoid diuretics (will worsen hypotension); (d) Reperfusion urgently — the hypotension (haemodynamic compromise) makes this high-risk; thrombolysis is first choice at this rural facility (streptokinase or tenecteplase; BP 85 mmHg is a relative contraindication — risk-benefit favours treatment). (e) Temporary pacing readiness (complete heart block common in inferior + RV MI).
Scenario C: A 58-year-old man with anterior STEMI undergoes primary PCI successfully. On day 2, he develops new-onset AF at 140 bpm. LVEF on echo is 35%. He is currently on aspirin + ticagrelor. What additional management is needed, and what scoring systems guide your anticoagulation decision?
Analysis: New AF at 140 bpm requires: (1) Rate control: IV beta-blocker (metoprolol 2.5–5 mg IV) or diltiazem if beta-blocker contraindicated; target HR <110 bpm initially; (2) Anticoagulation for AF stroke prevention: calculate CHA₂DS₂-VASc score — age 58, male, LVEF ≤35% (heart failure/LV dysfunction = 1 point), MI is CAD/peripheral vascular disease (1 point); total ≈ 2–3 points depending on other factors → score ≥2 in males = oral anticoagulation indicated; (3) Triple therapy consideration: he is already on DAPT (aspirin + ticagrelor) + now needs oral anticoagulant (OAC) for AF → triple therapy = OAC + aspirin + P2Y12. Triple therapy significantly increases bleeding risk. Current ESC guidance: shorten triple therapy to 1 week then drop aspirin, continuing DAPT (P2Y12 + OAC) for 6–12 months. HAS-BLED score (hypertension, abnormal renal/liver function, stroke, bleeding, labile INR, elderly, drugs) assesses bleeding risk and guides duration.
CLINICAL PEARL
The contraindication to nitrates in RV infarction is one of the highest-stakes drug interactions in emergency medicine. The right ventricle in RV infarction is completely dependent on preload to fill the left side of the heart — it has lost its active pumping ability. Any drug that reduces venous return (preload) — nitrates, diuretics, morphine-induced venodilation — will cause catastrophic hypotension. The treatment is the opposite: IV fluid bolus (500 mL–1 L normal saline) to force-fill the passive RV. Recognise the clinical triad — hypotension + elevated JVP + clear lung fields in inferior STEMI — and switch from the standard 'nitrate the chest pain' reflex to the 'give fluid, withhold nitrate' protocol.
Second pearl: the CHA₂DS₂-VASc score must be calculated for every patient with new AF post-MI. The score includes a point for 'vascular disease' — prior MI, peripheral arterial disease, or aortic plaque — meaning most post-MI patients with AF will score ≥2 and require oral anticoagulation. When DAPT is already running, this creates triple therapy with its attendant bleeding risk — knowing the ESC guidance to shorten triple therapy duration is a high-yield clinical fact.