Page 14 of 24
IM2.{17,21-22,24} | ACS Resuscitation and Rehabilitation — SDL Guide
Learning Objectives
- Describe the indications and methods of cardiac rehabilitation after ACS
- Demonstrate and perform basic life support (BLS) on a mannequin including chest compressions and rescue breathing
- Observe and understand the key components of an Advanced Cardiac Life Support (ACLS) programme
- Counsel and communicate with patients and families about lifestyle modification after ACS — including smoking cessation, diet, exercise, and medication adherence
INSTRUCTIONS
ACS resuscitation and rehabilitation skills are at the intersection of immediate life-saving technique (BLS/ACLS) and long-term behaviour change (cardiac rehabilitation). This module equips you to perform BLS correctly, understand the ACLS programme structure, design a cardiac rehabilitation plan, and counsel patients effectively on the lifestyle modifications that determine their long-term prognosis after MI.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 296 — Cardiac Rehabilitation (textbook)
- API Textbook of Medicine, 10th ed., Ch. on Cardiac Rehabilitation (textbook)
- AHA/ACC 2022 Guideline on Cardiac Rehabilitation after ACS (guideline)
- Indian Council of Medical Research (ICMR) Guidelines on Cardiac Rehabilitation in India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two weeks after Suresh's anterior STEMI and primary PCI, he is being discharged from the cardiology ward with a drug-eluting stent in his LAD and an LVEF of 45%. His wife asks you: 'What should he do when he gets home? Can he walk? Can he go back to work? Does he still need to take all these tablets?' On the same ward, a 60-year-old man with no prior cardiac history collapses suddenly in the corridor. A nurse finds him unresponsive with no breathing. Three minutes later, the ward team has confirmed VF on the monitor. The crash trolley is 30 metres away. You are the first medical person at the bedside. These two scenarios — the survivor beginning rehabilitation and the patient in cardiac arrest — represent the two ends of the ACS outcomes spectrum. Both require specific skills: for the collapsed patient, you need CPR technique that is correct enough to sustain cerebral perfusion for the three minutes until the defibrillator arrives; for Suresh, you need the counselling skills and rehabilitation knowledge to transform a frightened post-MI patient into an empowered self-manager who reduces his recurrence risk by 25%. This module builds both skill sets.
WHY THIS MATTERS
The competencies IM2.22 (BLS — performance level P, meaning you must demonstrate the skill, not merely know the concept) and IM2.21 (ACLS observation and participation) are unique in the IM2 set as procedural skills requiring hands-on practice, not just knowledge acquisition. In India, unexpected cardiac arrest in hospital (in-hospital cardiac arrest, IHCA) carries a survival-to-discharge rate of approximately 15–20% — substantially lower than the >30% survival rates reported in countries with systematic BLS/ACLS programmes. Improving BLS quality by healthcare providers is one of the most directly actionable steps toward better IHCA outcomes, and the final-year student who can deliver high-quality chest compressions with correct depth and rate is a first-responder asset on any ward. Cardiac rehabilitation, by contrast, addresses the chronic disease self-management gap that contributes to the 10–15% one-year post-MI mortality — particularly in India where structured CR programmes are limited and outpatient follow-up is inconsistent.
RECALL
Recall from earlier modules: STEMI and other large MIs reduce LVEF (left ventricular ejection fraction); post-MI patients with LVEF ≤40% are at highest risk of recurrent events and sudden cardiac death (SCD) from ventricular arrhythmias. From anatomy: the carotid artery is the preferred pulse check site in an unconscious adult (femoral artery is acceptable in the ICU setting). From physiology: effective chest compressions generate approximately 25–30% of normal cardiac output — sufficient to maintain coronary and cerebral perfusion during arrest but inadequate to restore spontaneous circulation without defibrillation in VF/VT. From pharmacology: adrenaline (epinephrine) 1 mg IV every 3–5 minutes is the vasopressor of choice in cardiac arrest — it increases coronary and cerebral perfusion pressure by α1-adrenoceptor-mediated peripheral vasoconstriction. Amiodarone is the first-line antiarrhythmic in refractory VF (300 mg IV bolus after third shock).
Clinical Indication: When BLS, ACLS, and Cardiac Rehabilitation Apply
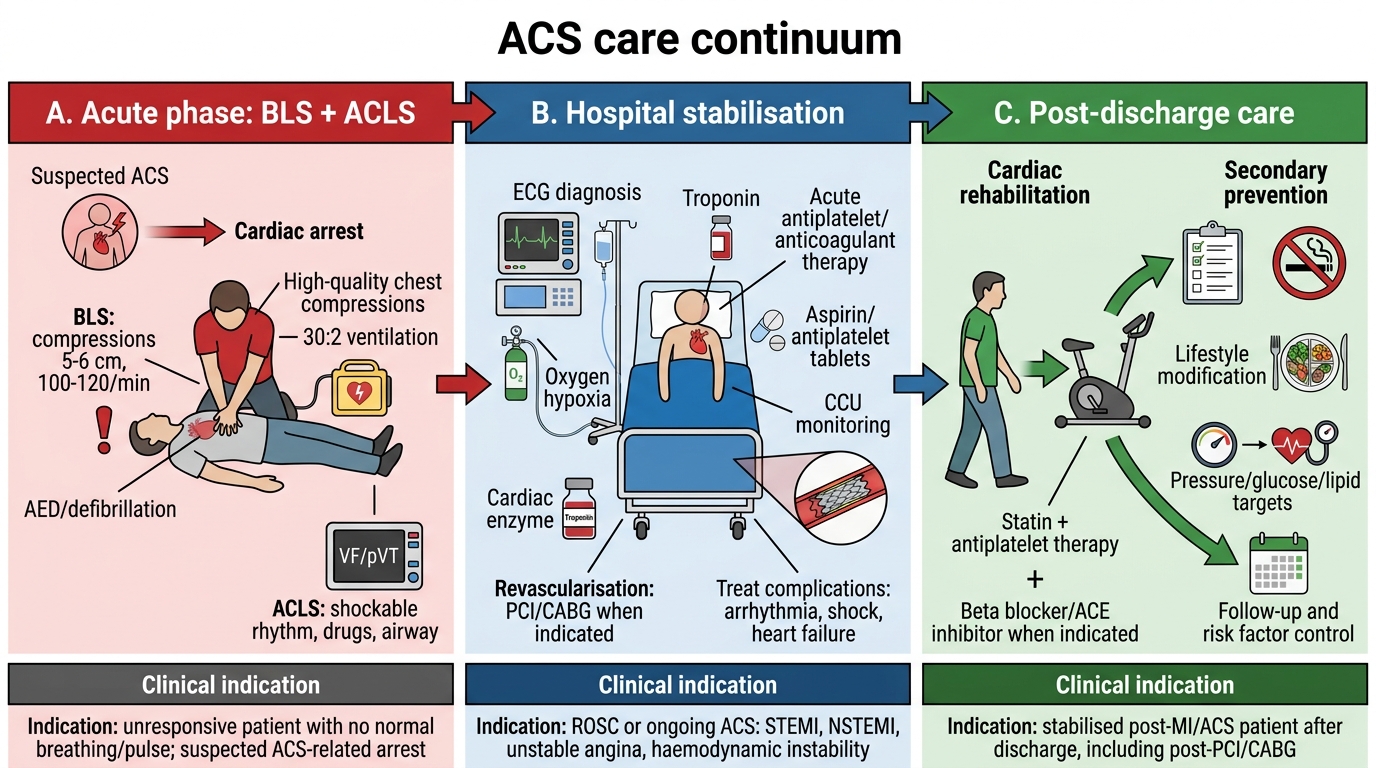
BLS, ACLS, and cardiac rehabilitation address three distinct phases of the ACS continuum: immediate life-support at the point of cardiac arrest; advanced resuscitation in a monitored environment; and structured recovery and secondary prevention over the weeks to months after the acute event. Understanding the clinical indication and the goals of each intervention ensures that the right response is deployed at the right time.
Basic Life Support (BLS) is indicated for any patient found unresponsive with absent or abnormal breathing (gasping counts as absent breathing for the purposes of starting CPR). The goal is to maintain cerebral and coronary perfusion until a defibrillator is available and advanced support can be provided. BLS is applicable in any setting — ward, corridor, community, home — and requires no equipment beyond a flat surface. The sequence: safety → shout for help → check responsiveness → check breathing → call 999/112/local emergency number → start chest compressions → use AED when available. The 'check for pulse' step is performed simultaneously with breathing check and should take no more than 10 seconds — delay in starting compressions is the most common source of BLS failure.
ACLS (Advanced Cardiac Life Support) is indicated in monitored environments (CCU, ICU, emergency department) where cardiac rhythm can be identified, IV access exists, and advanced airway management is possible. ACLS adds defibrillation (for VF/pulseless VT), rhythm-guided drug therapy (adrenaline, amiodarone), reversible cause identification ('4Hs and 4Ts' — see step 3 below), and post-resuscitation care. ACLS does NOT replace high-quality BLS — it augments it. A common error is interrupting chest compressions for medication preparation, rhythm analysis, or intubation — the rule is: minimise hands-off time to <5 seconds during compressions (acceptable interruption: pulse check every 2 minutes, rhythm analysis, shock delivery).
Cardiac Rehabilitation (CR) is indicated for all post-ACS patients, including post-STEMI, post-NSTEMI, post-PCI, and post-CABG. The indication is established by the ACS event itself — all such patients are eligible and should be offered CR as part of the discharge plan. CR is also indicated for patients with stable angina (CCS class II–III), heart failure with LVEF ≤35% (exercise-based CR reduces hospitalisation — HF-ACTION trial), and post-cardiac surgery patients. In India, formal hospital-based CR centres are limited to tertiary hospitals and major cities — the majority of post-MI patients require a home-based or community-delivered CR equivalent, which makes patient and family education at discharge a critical CR substitute.
ACS Care Continuum
Governing Principles: BLS and ACLS Evidence Base
The principles governing BLS and ACLS are derived from the physiology of cardiac arrest and the evidence from large resuscitation registries and randomised trials. Understanding these principles — not just memorising the algorithm — enables you to improvise correctly when the textbook scenario does not match the real arrest, and to explain to colleagues why each step matters. The chain of evidence from basic physiology through randomised trial data justifies every procedural detail in the BLS and ACLS protocols: the specific compression depth of 5–6 cm, the 100–120/min rate, the 30:2 compression-to-ventilation ratio, and the timing of drug administration relative to shock delivery are not arbitrary conventions — each has a quantitative physiological or clinical outcome basis. Students who understand the 'why' behind the protocol are far more robust under the cognitive load of a real resuscitation than those who can recite the steps but have not internalised the rationale.
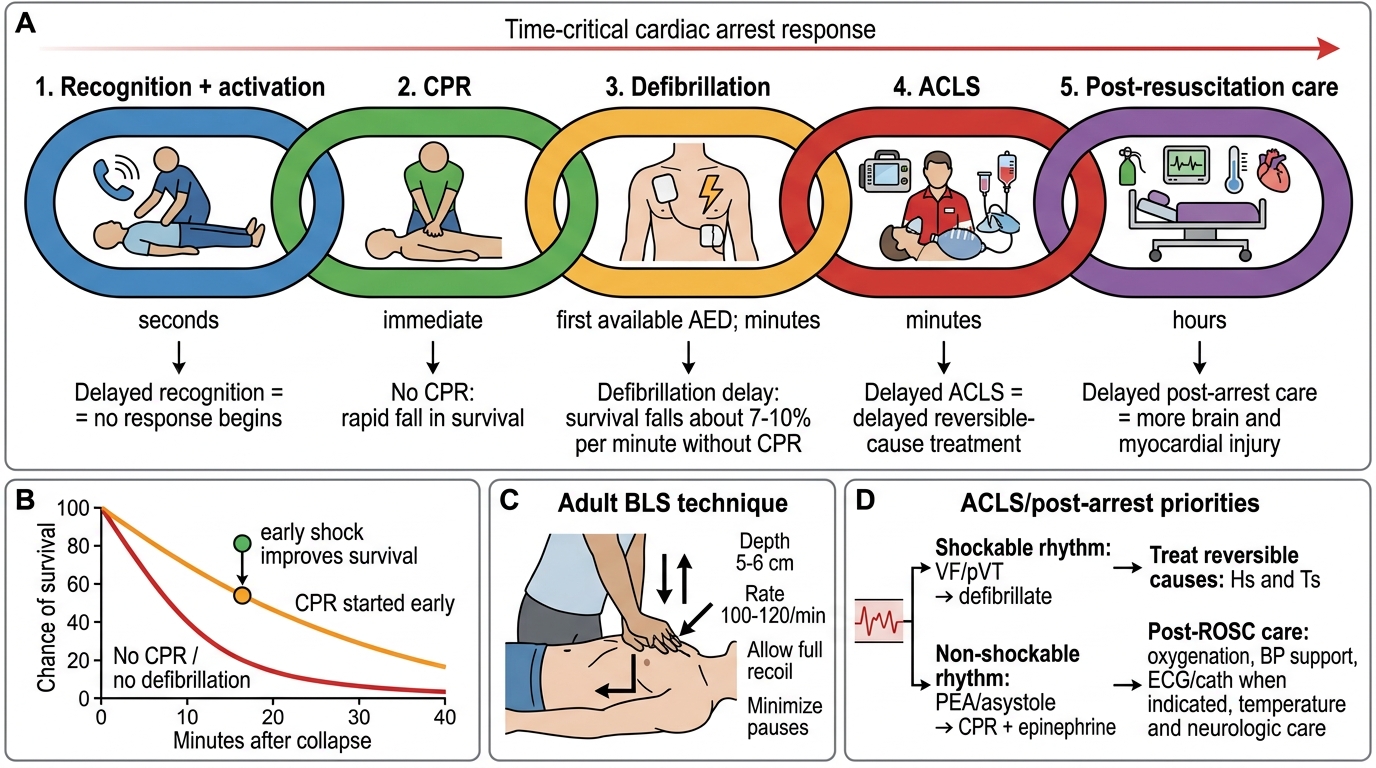
The Chain of Survival (American Heart Association, 5 links) captures the evidence-based sequence of interventions that maximises survival from sudden cardiac arrest:
1. Recognition and activation: immediate recognition of cardiac arrest and activation of the emergency response; survival decreases by approximately 7–10% for every minute without defibrillation for shockable rhythms (VF/pulseless VT)
2. Early CPR: high-quality chest compressions maintain approximately 25–30% of normal cardiac output; importantly, CPR does not terminate VF — it maintains organ perfusion and increases the probability that defibrillation will restore organised rhythm
3. Rapid defibrillation: for every minute of VF without defibrillation, survival decreases by ~10%; early defibrillation is the single most time-critical intervention in VF arrest
4. Advanced resuscitation (ACLS): airway management, vascular access, drug therapy, rhythm-guided interventions
5. Post-resuscitation care: targeted temperature management, percutaneous coronary intervention for ACS-triggered arrest, haemodynamic optimisation in the ICU
Physiology of effective CPR:
Chest compressions generate forward cardiac output via two mechanisms: (1) direct cardiac pump — cardiac chambers are squeezed between the sternum and spine; and (2) thoracic pump — compression raises intrathoracic pressure, driving blood forward. The critical parameters are: rate (100–120 compressions/minute — below 100 reduces output; above 120 reduces diastolic filling time), depth (5–6 cm in adults — insufficient depth is the most common CPR error), recoil (complete chest recoil between compressions is essential to allow venous return — 'do not lean on the chest'), and minimise interruptions (compression fraction — the proportion of time compressions are delivered — should be >60%; ideally >80%).
Ventilation in CPR: The current BLS ratio is 30 compressions: 2 rescue breaths (30:2). Each breath should be delivered over 1 second — just enough to produce visible chest rise. Avoid hyperventilation (over-breathing is common and harmful — it increases intrathoracic pressure, reduces venous return, and may cause gastric insufflation with regurgitation risk). If the rescuer is unwilling or unable to deliver rescue breaths (bystander CPR), compression-only CPR is acceptable for the first few minutes and produces equivalent outcomes to standard CPR in adults with witnessed cardiac arrest (PALS guidelines differ — ventilation is more important in paediatric arrest, which is more commonly respiratory in origin).
Defibrillation principles: Biphasic defibrillators (standard in modern AEDs and manual defibrillators) deliver shocks at 120–200 J (first shock) followed by the same or higher energy for subsequent shocks. CPR is resumed immediately after the shock (even if the rhythm appears organised) — the defibrillator does not always restore normal rhythm, and the 2-minute CPR cycle before re-checking rhythm maintains perfusion. In VF/pulseless VT, the sequence is: shock → 2 minutes CPR → rhythm check → shock if still shockable → 2 minutes CPR → drug administration (adrenaline after second shock, amiodarone after third shock).
Adult Chain of Survival: Time-Sensitive Response to Cardiac Arrest
Procedure: BLS Technique and ACLS Algorithm
Correct BLS technique is a procedural skill requiring repeated practice to embed muscle memory — reading the steps is not equivalent to being able to perform them under the stress of a real arrest. The steps below must be practised on a mannequin, with attention to the common technique errors identified by feedback manikins and simulation faculty. Research using real-time CPR feedback devices consistently shows that healthcare providers overestimate their compression depth (mean actual depth in real arrests is approximately 4.2 cm — below the 5-cm floor) and underestimate their compression rate (many providers compress too slowly when focused on depth). The single most reliable way to correct these biases is deliberate practice with objective feedback. The textual description of each step here is the knowledge scaffold; the skill itself must be earned on the mannequin, repeatedly, until the physical parameters become automatic under stress.
BLS sequence for a healthcare provider (AHA 2020 guidelines — adult):
- Scene safety: before approaching — confirm the environment is safe (electrical hazard, traffic, unstable structure). Do not become a second victim.
- Check responsiveness: tap the patient's shoulders firmly and shout 'Are you okay?' simultaneously for both checks.
- Shout for help + call emergency services: if the patient is unresponsive, shout loudly for help immediately; activate the in-hospital emergency response (call 2222 or equivalent) or direct someone specifically ('You — call 112 NOW').
- Check breathing and pulse simultaneously (≤10 seconds): look for chest rise; check carotid pulse with two fingers in the groove beside the trachea. If no breathing AND no pulse (or unsure) → start CPR. Gasping = absent effective breathing; start CPR.
- Positioning: place the patient supine on a flat, firm surface. Kneel beside the patient at shoulder level.
6. Chest compressions — technique (the most skill-dependent step):
- Heel of one hand on the lower half of the sternum (NOT over the xiphoid process, which can cause liver laceration)
- Second hand interlocked on top; fingers raised off the chest
- Arms fully extended, elbows locked; shoulders directly over the heel of the hand
- Depth: 5–6 cm (approximately 2 inches) — feel the sternum move; do not estimate
- Rate: 100–120/minute — count aloud or use a metronome
- Complete recoil: allow the chest to fully rise after each compression; do not lean on the chest
- Minimise interruptions: no breaks for >10 seconds except for rhythm check (every 2 min) and shock
- Rotate compressors every 2 minutes in multi-rescuer CPR — fatigue causes compression depth to drop significantly after 2 minutes
7. Rescue breathing (after 30 compressions):
- Head-tilt chin-lift (or jaw-thrust if cervical spine injury suspected)
- Pinch the nose, make a seal, deliver 1 breath over 1 second — chest should rise visibly
- Repeat once (total 2 breaths), then immediately resume compressions
- If unable or unwilling to provide rescue breaths: compression-only CPR
8. Use AED as soon as available:
- Apply pads (right of sternum below clavicle; left lateral chest wall)
- Follow AED voice prompts; stand clear during rhythm analysis and shock
- Resume CPR immediately after shock delivery
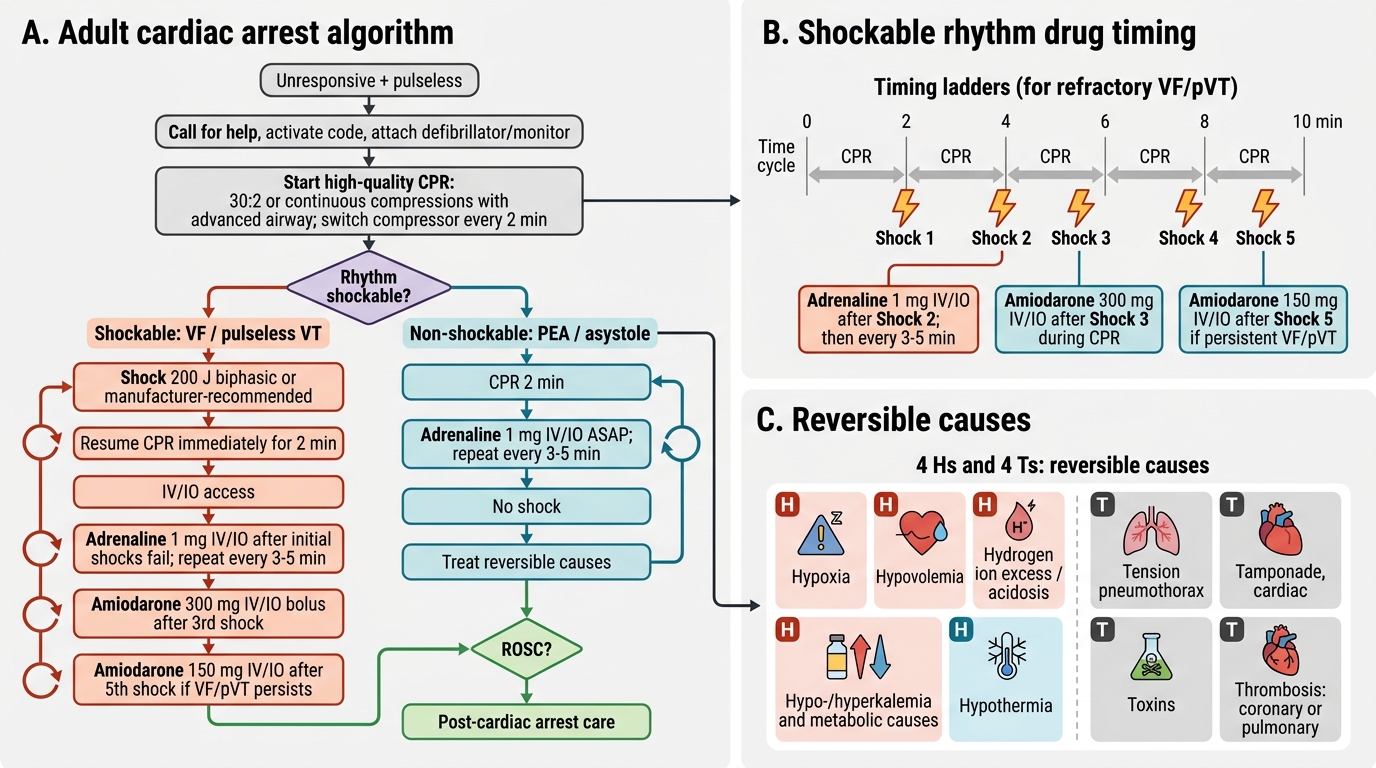
ACLS algorithm for shockable rhythms (VF/pulseless VT):
The ACLS algorithm applies to a monitored patient in the CCU or ICU where the rhythm is known:
1. Confirm cardiac arrest (unresponsive, pulseless, no breathing)
2. Call for help; start CPR (30:2 or continuous compressions with advanced airway)
3. Attach monitor/defibrillator
4. If shockable (VF/pulseless VT):
- Shock 1: charge to 200 J biphasic (or maximum device energy); clear, confirm no one touching patient; deliver shock
- Immediately resume 2 minutes CPR → rhythm check
- If still VF/pulseless VT: Shock 2
- Resume CPR → adrenaline 1 mg IV every 3–5 minutes (starting from this point; ideally after 2nd shock; to be given every alternate cycle thereafter)
- Rhythm check → if still VF/pulseless VT: Shock 3
- Resume CPR → amiodarone 300 mg IV bolus (after 3rd shock; second dose 150 mg after 5th shock if still VF)
- Continue CPR cycles: shock → 2 min CPR → drug (adrenaline every other cycle) → shock
5. Reversible causes ('4Hs and 4Ts') — search and treat throughout:
- 4Hs: Hypoxia (ensure adequate oxygenation + ventilation), Hypovolaemia (IV fluids), Hypo/Hyperkalaemia + metabolic disorders (correct electrolytes), Hypothermia (rewarm)
- 4Ts: Tension pneumothorax (needle decompression), Tamponade cardiac (pericardiocentesis), Toxins (antidote as appropriate), Thrombosis — pulmonary (thrombolysis) or coronary (consider PCI post-ROSC)
Non-shockable rhythms (PEA/Asystole):
- CPR immediately, no shock
- Adrenaline 1 mg IV as soon as IV access established, then every 3–5 minutes
- Search for and treat reversible causes (4Hs and 4Ts) — PEA especially demands rapid identification of the cause
- Asystole: confirm in two leads; atropine is NOT recommended in current guidelines (removed from 2010 guidelines onward — no evidence of benefit)
Post-resuscitation care (ROSC achieved):
- 12-lead ECG immediately: identify STEMI → activate cath lab for primary PCI even if comatose
- Targeted temperature management (TTM): if comatose post-ROSC, cool to 32–36°C for 24 hours (TTM trial — improves neurological outcomes in unconscious survivors)
- ICU admission: haemodynamic and ventilatory support; avoid hyperoxia (target SpO2 94–98%)
Adult BLS/ACLS Cardiac Arrest Algorithm
SELF-CHECK
During an in-hospital cardiac arrest in the CCU, a 64-year-old man is found in VF. Three shocks have been delivered (200 J each) with 2-minute CPR cycles between them, and the rhythm remains VF. IV access is established. Which drug should be given NEXT, in what dose, and at what point in the CPR cycle?
A. Adrenaline 1 mg IV after every shock — it is the first-line vasopressor regardless of shock count
B. Amiodarone 300 mg IV bolus — given after the third shock (during the next 2-minute CPR cycle), with adrenaline also due at this point
C. Lignocaine 1 mg/kg IV — it is preferred over amiodarone after three shocks in current guidelines
D. Magnesium sulphate 2 g IV — first-line antiarrhythmic in refractory VF
Reveal Answer
Answer: B. Amiodarone 300 mg IV bolus — given after the third shock (during the next 2-minute CPR cycle), with adrenaline also due at this point
After the third shock in refractory VF, the ACLS protocol calls for amiodarone 300 mg IV bolus — this is the current first-line antiarrhythmic recommendation (AHA 2020, ILCOR). A second dose of amiodarone 150 mg is given if VF persists after the fifth shock. Adrenaline 1 mg IV should have been administered after the second shock and continues every 3–5 minutes (every alternate 2-minute CPR cycle). At the third shock point, adrenaline is also due if it has been ≥3–5 minutes since the last dose. Lignocaine 1.5 mg/kg IV is an alternative to amiodarone (not preferred, but listed as acceptable in AHA 2020 if amiodarone is unavailable). Magnesium is indicated specifically for torsades de pointes (polymorphic VT with long QT), not generic refractory VF.