Page 7 of 13
IM20.3-5 | Seizure Disorder Management and Safety — SDL Guide (Part 3)
Self-Assessment: Management Scenarios
You have now covered the acute management algorithm for a seizure and status epilepticus (with timings and drug doses), the principles of AED selection by seizure type and syndrome (including the contraindicated drug pairings), drug interactions (enzyme induction, valproate inhibition, phenytoin zero-order kinetics), and the structured safety counselling domains (driving, occupation, swimming, sleep, alcohol, adherence, women of childbearing age). The scenarios below test application of these competencies at the NMC IM20.3–IM20.5 level. For each, formulate your answer before reading the analysis.
Scenario A: A 40-year-old man with a history of alcohol dependence is brought to the emergency department at 3 AM by his wife. He had his last drink approximately 36 hours ago and has been trying to quit without medical help. He is now having a generalised tonic-clonic seizure, which has lasted 7 minutes at the time of arrival. Blood glucose: 52 mg/dL (2.9 mmol/L). He is thin, with signs of chronic liver disease.
Analysis: This is status epilepticus (>5 minutes). However, there is a critical metabolic cause: hypoglycaemia (glucose 52 mg/dL) AND alcohol withdrawal (36 hours after last drink — classic window for withdrawal seizures). Sequence of treatment: (1) immediately give thiamine 100 mg IV before glucose — in a malnourished chronic alcoholic, glucose administration without thiamine can precipitate Wernicke's encephalopathy; (2) then 50 mL of 50% dextrose IV; (3) if seizure continues after glucose correction, proceed with IV lorazepam for status epilepticus. AED therapy: alcohol withdrawal seizures are provoked seizures — long-term AED therapy is NOT indicated once the patient achieves sustained abstinence. The management is thiamine replacement, alcohol withdrawal management (chlordiazepoxide detox regime), and nutritional support.
Scenario B: A 16-year-old girl with a recent diagnosis of childhood absence epilepsy (confirmed by 3 Hz spike-and-wave on EEG during hyperventilation) is brought to your outpatient clinic with her mother. She has no tonic-clonic seizures — pure absence only. The mother has read online about epilepsy and asks if 'carbamazepine, which is the most commonly used epilepsy drug, would be suitable'. She also asks whether her daughter can continue to swim on the school swimming team.
Analysis: Carbamazepine is absolutely contraindicated in childhood absence epilepsy — it will worsen absence frequency. The correct first-line drug is ethosuximide (absence only, no GTCS). Counsel the mother clearly about this contraindication. Regarding swimming: competitive swimming is a significant drowning risk in uncontrolled epilepsy. Until absence seizures are well controlled on AED therapy, solo competitive swimming is not recommended. Once seizures are controlled for a sustained period and the neurologist agrees, competitive swimming with a designated lifeguard who is aware of her diagnosis may be permitted. Document both counselling points.
Scenario C: A 65-year-old woman with hypertension, atrial fibrillation (on warfarin, INR 2.4), and a previous ischaemic stroke 2 years ago develops a new-onset focal impaired awareness seizure affecting her right hand. MRI confirms a gliotic area in the left temporal lobe corresponding to the old infarct. She has two further seizures over the next week. What AED would you choose and what monitoring is required?
Analysis: This is new-onset epilepsy in an elderly patient with structural aetiology (post-stroke, focal). Preferred AED: lamotrigine or levetiracetam. Both have minimal interactions with warfarin (levetiracetam is virtually interaction-free). Avoid carbamazepine and phenytoin: carbamazepine induces CYP3A4 and will lower warfarin levels, leading to under-anticoagulation and stroke risk; phenytoin has complex interactions with warfarin (may increase or decrease INR unpredictably). Monitoring: INR must be checked more frequently during AED titration regardless of the drug chosen; falls risk assessment (most AEDs cause dizziness); bone density (long-term).
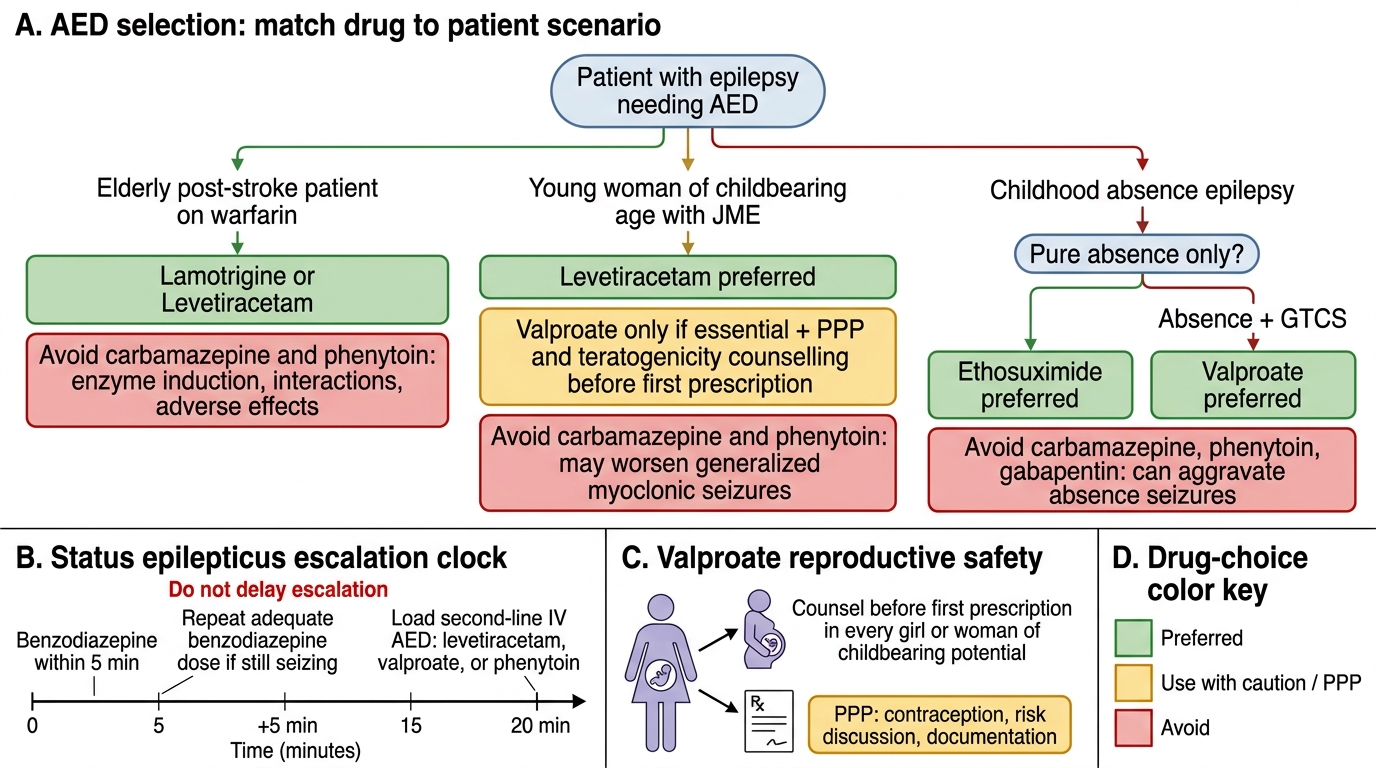
AED Selection Decision Tree for Key Clinical Scenarios
CLINICAL PEARL
Two high-yield management pearls that each carry patient-safety weight.
First: in status epilepticus, give benzodiazepine within 5 minutes — then escalate on time, not on hope. The single most common error in managing status epilepticus is waiting too long before escalating from benzodiazepines to a second-line IV AED. After one adequate benzodiazepine dose without response, wait only 5 minutes, then give a repeat dose; if still seizing after 20 minutes from onset, the second-line IV AED (levetiracetam, valproate, or phenytoin) must be loaded immediately. Every additional 10 minutes of seizure activity beyond 20 minutes exponentially increases neuronal injury and mortality.
Second: sodium valproate teratogenicity counselling is mandatory before first prescription in every girl or woman of childbearing potential — not when pregnancy is confirmed, not when the patient announces she wants a baby, but at the very first prescription. The harm to the developing brain occurs in the first trimester, often before a pregnancy is even detected. NICE 2022, EU regulatory authorities, and the UK Medicines and Healthcare products Regulatory Agency (MHRA) have issued explicit guidance on mandatory Pregnancy Prevention Programmes for valproate. A physician who prescribes valproate to a young woman without this documented counselling is both clinically and medicolegally exposed.