Page 13 of 20
IM21.9 | Bee Sting and Other Envenomation — SDL Guide
Learning Objectives
- Distinguish anaphylaxis from direct toxic envenomation in bee and wasp sting, and describe the specific management for each
- Describe the first-aid management of jellyfish envenomation, including the role of vinegar and what must be avoided
- Describe the clinical presentation of centipede and black widow spider envenomation and their management principles
- Apply adrenaline 0.5 mg IM as the correct first-line treatment for anaphylaxis from any envenomation source
- Recognise the renal risk from massive bee/wasp envenomation and describe the supportive management targeting pigment nephropathy
INSTRUCTIONS
Bee stings, jellyfish, and arthropod envenomation form the broad and diverse end of the envenomation spectrum. This module equips you to recognise the two critical distinctions — anaphylaxis versus toxic envenomation, and the specific first-aid steps for each arthropod — so that you can act correctly in the first minutes of any envenomation emergency.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Arthropod Envenomation; Anaphylaxis (textbook)
- API Textbook of Medicine, 10th ed. — Chapter on Envenomation (textbook)
- World Allergy Organization (WAO) Anaphylaxis Guidelines, 2020 Update (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two cases arrive at the same emergency department on the same afternoon. The first: a 32-year-old beekeeper, stung by hundreds of bees when a hive collapsed on him in his apiary. He has diffuse oedema, dark brown urine, and his serum creatinine has jumped to 4.2 mg/dL in six hours. He denies any prior history of bee allergy. The second: a 19-year-old woman who was stung by a single bee on the forearm while gardening. She has generalised urticaria spreading across her trunk, stridor, blood pressure of 75/40 mmHg, and is barely responsive. The first patient has been stung five hundred times; the second, once. Yet the second patient is in greater immediate danger of dying in the next ten minutes. What is happening in each case? What is the one drug that saves the second patient, and what organ system is at risk in the first? Can you recall the specific antidote for the most common household chemical exposure that kills by cholinergic crisis?
WHY THIS MATTERS
Bee stings and other envenomations — including jellyfish, centipede, spider, and wasp stings — are encountered by any doctor working in rural, agricultural, or coastal India. NMC competency IM21.9 requires the ability to describe the diagnosis, initial approach, stabilisation, and therapy of bee stings and other envenomation. The competency spans two clinically distinct emergencies: the acute anaphylaxis from a single sting in a sensitised individual (requiring immediate adrenaline), and the direct toxic syndrome from massive envenomation (multiple bee stings causing haemolysis, renal failure, and coagulopathy requiring supportive intensive care). Beyond bees, the module covers jellyfish, centipede, and wasp stings — each with a characteristic presentation and management principle. Understanding these presentations ensures that every physician — not just the toxicologist — can recognise and initiate life-saving treatment within the first critical minutes.
RECALL
Activate relevant prior knowledge. Recall from immunology that anaphylaxis is a type I hypersensitivity reaction: prior sensitisation generates IgE antibodies specific to an allergen; on re-exposure, the allergen cross-links IgE on mast cells and basophils → rapid degranulation → massive release of histamine, prostaglandins, and leukotrienes → systemic vasodilation, increased vascular permeability (urticaria, angioedema), bronchospasm, and cardiovascular collapse. Recall that adrenaline (epinephrine) is the only proven life-saving treatment for anaphylaxis: alpha-1 reverses vasodilation, beta-2 reverses bronchospasm, beta-1 supports cardiac output. Recall from physiology that haemolysis (red cell destruction) releases free haemoglobin into plasma; haemoglobin is filtered at the glomerulus as haemoglobinuria, and haemoglobin casts in the tubules cause pigment nephropathy and AKI — the same mechanism as myoglobinuria from rhabdomyolysis. From pharmacology: atropine blocks muscarinic receptors (reverses bradycardia, bronchoconstriction, hypersecretion); pralidoxime reactivates organophosphate-inhibited acetylcholinesterase.
Bee and Wasp Sting: Clinical Spectrum and Management
Bee and wasp stings produce two entirely distinct clinical syndromes depending on whether the patient is sensitised (prior exposure has generated IgE antibodies) and whether the sting is single or massive. Recognising which syndrome is present within the first few minutes of evaluation determines whether the treatment is adrenaline (anaphylaxis) or supportive ICU care (toxic massive envenomation). Conflating these two syndromes is a dangerous error: giving antihistamines as first-line treatment for anaphylaxis is inadequate, while treating a massively stung patient with only adrenaline misses the unfolding organ-system toxicity.
Syndrome 1 — Anaphylaxis from a single (or few) sting(s) in a sensitised individual:
Bee venom contains phospholipase A2 and melittin as major allergens. In a sensitised person (previous bee sting with sensitisation), re-exposure triggers a type I IgE-mediated anaphylactic reaction. The clinical presentation is characterised by rapid onset (seconds to minutes) of: generalised urticaria and pruritus, angioedema (face, lips, tongue), bronchospasm (wheeze, breathlessness), stridor (laryngeal oedema), hypotension, tachycardia, and potentially loss of consciousness. Anaphylaxis is defined clinically as a severe, life-threatening systemic hypersensitivity reaction — and bee sting is one of the most common triggers in India. Without immediate treatment, cardiovascular collapse and death can occur within minutes.
Management of bee sting anaphylaxis:
- Adrenaline 0.5 mg IM (1:1000 solution, 0.5 mL) into the anterolateral thigh — the first and only life-saving treatment, given before anything else. This is the same action as for antivenom anaphylaxis. Repeat every 5–15 minutes if response is inadequate.
- Remove the stinger by scraping (not pinching — pinching squeezes residual venom from the venom sac into the wound).
- Lay flat with legs elevated if hypotensive (unless respiratory distress — then semi-recumbent).
- IV access and IV normal saline 500–1000 mL for hypotension.
- IV chlorphenamine 10 mg and IV hydrocortisone 200 mg as adjuncts (onset delayed).
- Salbutamol nebulisation for persistent bronchospasm.
- Monitor for biphasic anaphylaxis (recurrence 1–8 hours later) — observe for minimum 4–6 hours.
- Prescribe an auto-injector adrenaline pen (EpiPen) and allergy referral for long-term management.
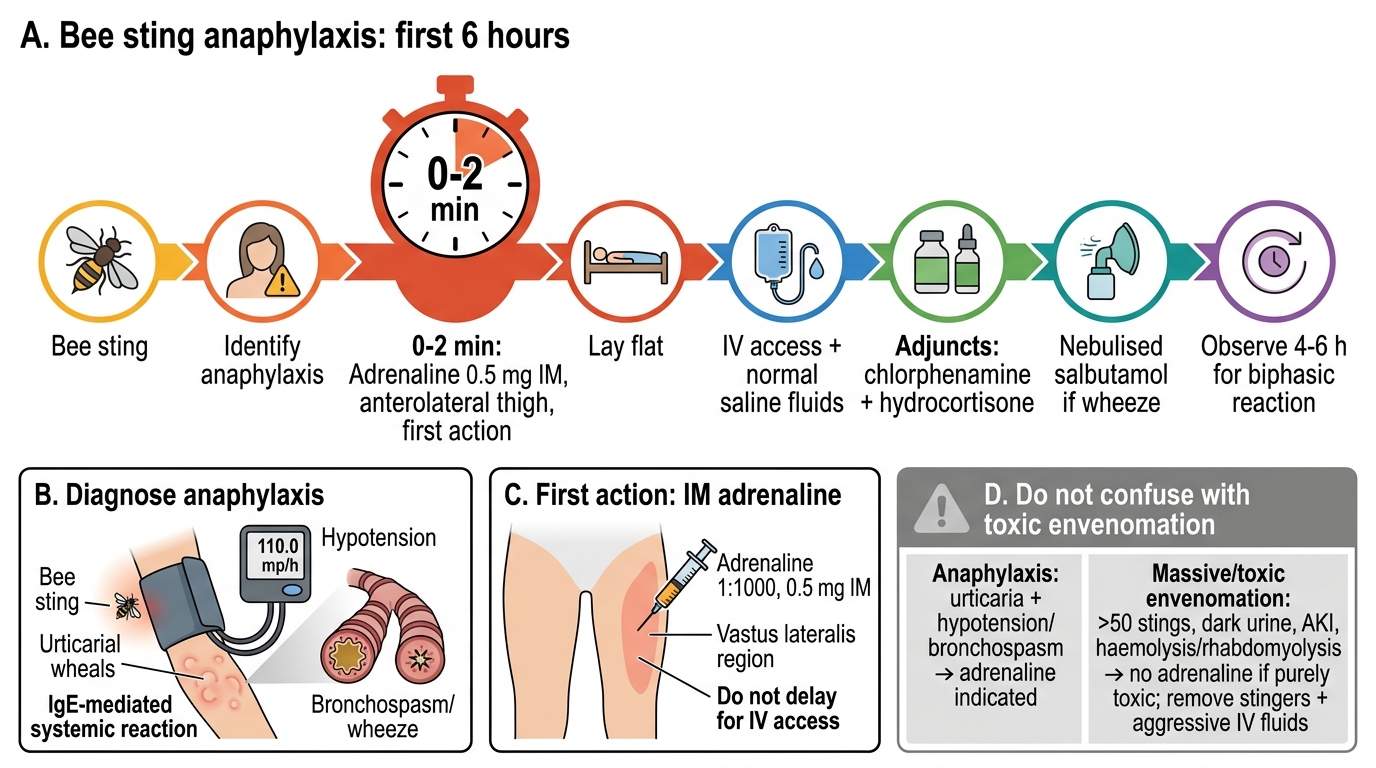
Bee Sting Anaphylaxis Management Algorithm
Syndrome 2 — Massive/toxic bee envenomation (>50 stings, typically >100):
When a large number of stings occur simultaneously — as in an attack by an entire hive (50–1000+ stings) — the cumulative venom load produces direct toxicity independent of prior sensitisation. The venom components cause: haemolysis (phospholipase A2 destroys red cell membranes → haemoglobinuria → pigment nephropathy), rhabdomyolysis (melittin-mediated myonecrosis → myoglobinuria), hepatotoxicity, direct nephrotoxicity, and in severe cases a consumption coagulopathy. The clinical presentation is systemic collapse without the urticarial/bronchospasm pattern of anaphylaxis: dark urine, jaundice, diffuse oedema, and acute kidney injury developing over hours to days. There is NO role for adrenaline in purely toxic envenomation — the mechanism is not IgE-mediated.
Management of massive bee envenomation:
- Remove all stingers by scraping.
- Aggressive IV fluid hydration (normal saline 200–300 mL/hour) targeting urine output ≥200 mL/hour — the priority is to flush haemoglobin and myoglobin casts from the renal tubules.
- Monitor urine colour and dipstick (dark urine + blood on dipstick + no red cells on microscopy = pigment nephropathy).
- Serial serum creatinine, CK, LDH, and liver enzymes.
- Manage acute kidney injury with nephrology input; dialysis if renal failure progresses.
- Antihistamines for any urticarial component.
- ICU admission for systemic toxicity with ≥100 stings.
SELF-CHECK
A 22-year-old woman develops generalised urticaria, stridor, and blood pressure of 70/40 mmHg within 3 minutes of a bee sting. She has no previous history. The MOST important immediate action is:
A. IV chlorphenamine 10 mg to block histamine release
B. IV hydrocortisone 200 mg to reduce the inflammatory response
C. Adrenaline 0.5 mg intramuscularly into the anterolateral thigh
D. Nebulised salbutamol 5 mg for the bronchospasm component
Reveal Answer
Answer: C. Adrenaline 0.5 mg intramuscularly into the anterolateral thigh
This is anaphylaxis — urticaria, stridor, and severe hypotension within minutes of a bee sting. Adrenaline 0.5 mg IM into the anterolateral thigh is the only life-saving treatment and must be given first. It reverses vasodilation (alpha-1), bronchospasm (beta-2), and supports cardiac output (beta-1). Chlorphenamine and hydrocortisone are adjuncts with delayed onset (hydrocortisone takes 4–6 hours to act) — they do not treat the acute phase. Salbutamol is adjunctive for bronchospasm after adrenaline. Delaying adrenaline to give antihistamines or steroids first is a recognised cause of preventable death in anaphylaxis.
Jellyfish Envenomation
Jellyfish envenomation is encountered in coastal states of India — Kerala, Tamil Nadu, Karnataka, Andhra Pradesh, Odisha, Maharashtra, Gujarat, and West Bengal — and in the Andaman and Nicobar Islands. The envenomation mechanism is unique: jellyfish tentacles carry thousands of microscopic nematocysts — highly pressurised coiled tubules that discharge on contact with skin, injecting venom through the epidermis. The discharge is triggered by touch and is essentially instantaneous; even tentacles separated from the jellyfish remain capable of firing nematocysts for hours. This is why a common mistake — rubbing the affected area with a towel — causes thousands of additional nematocyst discharges and dramatically worsens envenomation.
Clinical presentation: Most jellyfish stings in India cause local envenomation only: immediate intense burning pain, linear or branching erythema following the tentacle contact pattern ('whiplash marks'), oedema, and vesicle formation over the subsequent hours. The pattern of the marks often retains the branching geometry of the tentacle, which is pathognomonic.
Systemic envenomation is uncommon from the jellyfish species commonly encountered in Indian coastal waters but can occur with specific species (Physalia physalis — Portuguese man-o-war is not a true jellyfish but a siphonophore, but causes similar stings; Chironex fleckeri — the Australian box jellyfish — is not found in Indian waters but is taught for completeness). Systemic features, when they occur, include: nausea, vomiting, muscle cramps, arrhythmias, and in severe cases cardiovascular collapse.
Management:
1. Do NOT rub the area — rubbing discharges additional nematocysts.
2. Remove tentacles by flushing with seawater (NOT fresh water — fresh water changes osmolality and triggers nematocyst discharge) and picking off remaining tentacles with tweezers or a credit card-edge scraping motion.
3. Deactivate remaining nematocysts: Apply 5% acetic acid (household vinegar) to the affected area for 30 minutes — vinegar acidifies the nematocyst and prevents discharge. This is the standard first aid. Isopropyl alcohol 70% is an alternative.
4. Analgesia: Oral paracetamol or tramadol for pain. Topical lignocaine gel or ice pack for local relief.
5. Antihistamines for urticaria. Systemic features: treat symptomatically. Anaphylaxis (rare): adrenaline IM as above.
6. Tetanus prophylaxis if not up to date.
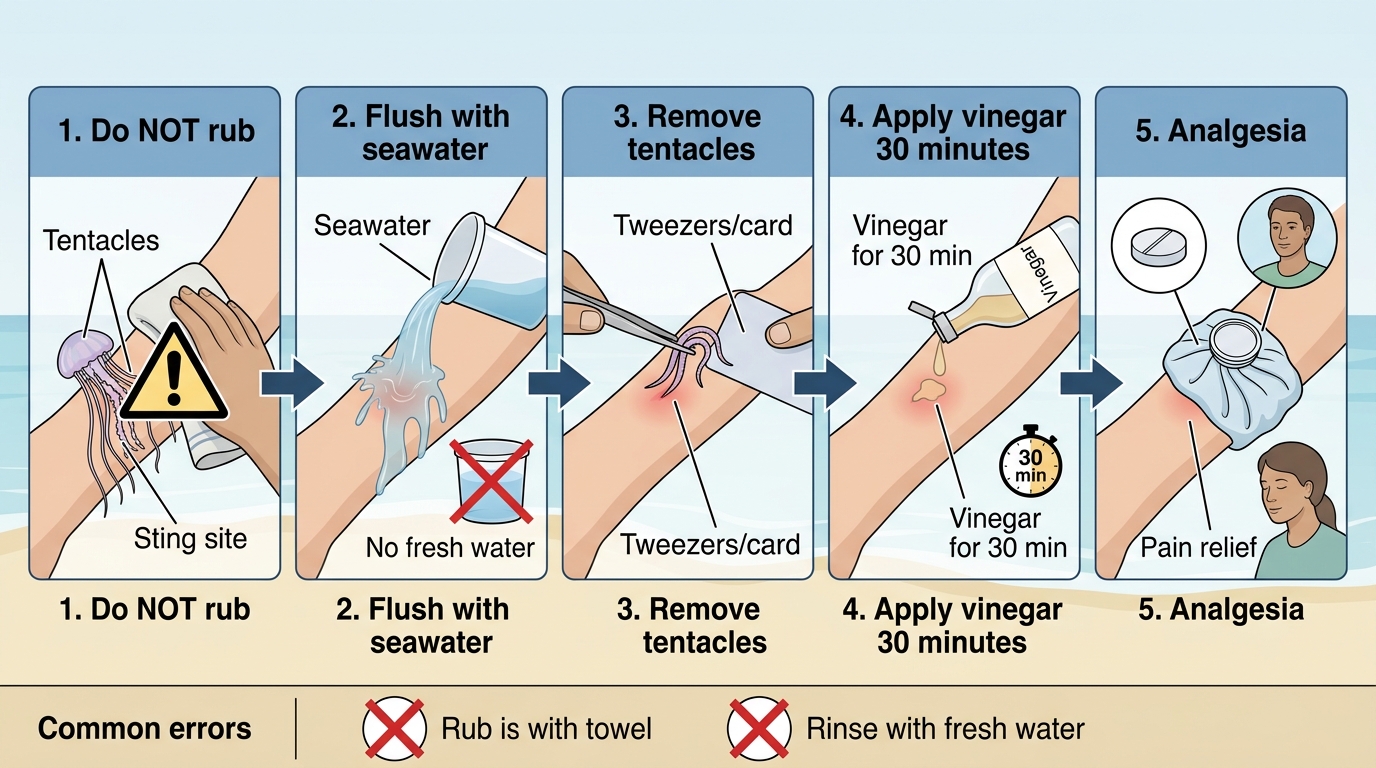
Jellyfish Sting First Aid Sequence
Centipede, Spider, and Other Arthropod Envenomation
Centipede and spider bites are common in India but rarely cause life-threatening envenomation. The clinical importance of these envenomations lies in correct first aid, accurate diagnosis, and avoiding unnecessary treatment based on overestimated danger. There are no species of truly dangerous spider in India comparable to the black widow or brown recluse of North America, though some local species cause significant local reactions.
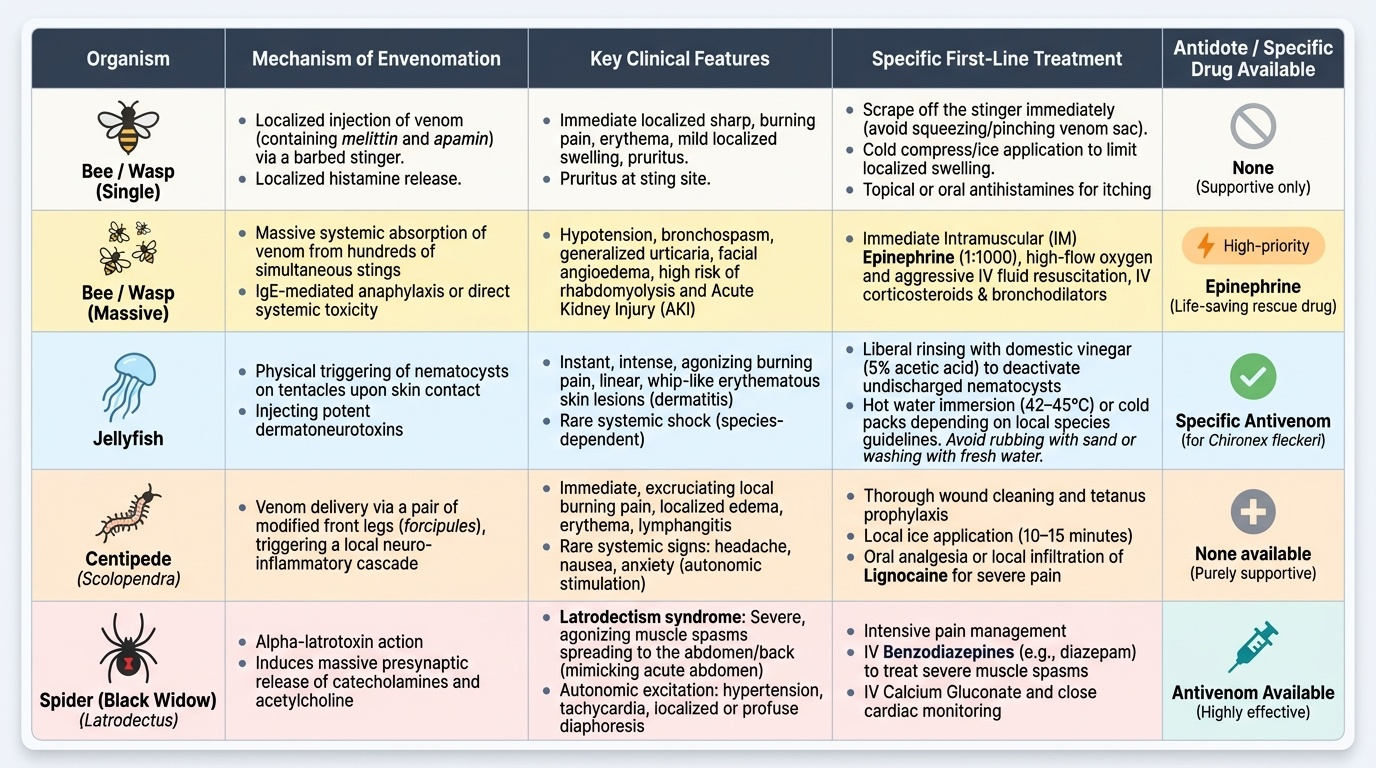
Provided image
Centipede envenomation: The Indian giant centipede (Scolopendra species) can reach 20–30 cm in length and delivers venom via a pair of modified front legs (forcipules), not its mouthparts. The bite causes immediate intense burning pain at the bite site, local oedema, erythema, and sometimes lymphangitis. Systemic features are rare but include headache, nausea, and anxiety from autonomic stimulation. Severe reactions with haemolysis and AKI are reported rarely from massive envenomation. Management is supportive: analgesia (paracetamol, tramadol, or local infiltration of lignocaine for severe pain), wound cleaning, tetanus prophylaxis, and observation for 4–6 hours for systemic features. Ice application for 10–15 minutes reduces local pain. No antivenom is available.
Spider envenomation: Most spider bites in India cause only local reactions — pain, erythema, and minor swelling. The black widow spider (Latrodectus species) is present in India and produces the latrodectism syndrome: severe abdominal cramps, diffuse muscle spasm (mimicking acute abdomen), tachycardia, hypertension, and diaphoresis — caused by massive catecholamine and acetylcholine release from spider venom (similar mechanism to scorpion). Management is supportive: opioid analgesia for cramps, benzodiazepines for muscle spasm, antihypertensives if needed. Black widow antivenom is available in some countries but not routinely in India; supportive management is the standard of care. The brown recluse spider (Loxosceles species) is not native to India but causes a necrotic local wound where present globally.
Wasp envenomation: Wasp stings follow the same principle as bee stings — single sting in a sensitised individual → anaphylaxis (treat with adrenaline IM); massive sting attack → direct toxicity with haemolysis and AKI (supportive care, aggressive IV fluids). The distinction between anaphylaxis and toxic envenomation applies to all Hymenoptera (bees, wasps, hornets) stings.
SELF-CHECK
A coastal fisherman in Kerala is brought in with linear branching erythematous marks on his forearm after handling a fishing net. He has intense pain and the marks are swelling. What is the first-aid intervention that should be applied to the sting area, and what should be specifically avoided?
A. Apply fresh water compresses to soothe the area; avoid salt water which may worsen the reaction
B. Apply 5% acetic acid (vinegar) for 30 minutes; avoid rubbing or fresh water which trigger nematocyst discharge
C. Apply a tourniquet above the marks to limit venom spread; avoid ice which may cause frostbite
D. Apply topical corticosteroid cream immediately; avoid acetic acid which may cause chemical burns
Reveal Answer
Answer: B. Apply 5% acetic acid (vinegar) for 30 minutes; avoid rubbing or fresh water which trigger nematocyst discharge
The linear branching erythematous marks following tentacle contact patterns are pathognomonic of jellyfish envenomation. The correct first aid is to apply 5% acetic acid (vinegar) to deactivate nematocysts, preventing further venom discharge. Two critical things to avoid: (1) rubbing the area, which mechanically triggers thousands of additional nematocyst discharges; (2) fresh water irrigation, which changes osmolality and also triggers nematocyst discharge. Seawater should be used for flushing/rinsing. Tourniquets are contraindicated. Topical steroids have no role in nematocyst deactivation.