Page 7 of 20
IM21.7 | Snake Bite Antivenom Therapy — SDL Guide
Learning Objectives
- Enumerate the indications for anti-snake venom (ASV), including the distinction between systemic envenomation (indication) and local swelling alone (not an indication)
- Describe the pharmacology of polyvalent ASV, including its mechanism of action, species coverage, and why rapid administration matters
- Specify the correct dose, route, dilution, and infusion rate for polyvalent ASV in systemic envenomation
- Recognise and manage early adverse reactions (anaphylaxis, anaphylactoid) and late reactions (serum sickness) to antivenom
- Describe the 6-hour 20WBCT endpoint for repeat dosing and explain the correct sequence of antivenom before blood products
INSTRUCTIONS
Anti-snake venom is the only cure for systemic snakebite envenomation, yet it is consistently under-dosed, delayed, or incorrectly withheld in Indian practice. This module builds the complete antivenom competency: indication recognition, pharmacology, correct administration protocol, and confident adverse reaction management. By the end, you will be able to run an antivenom infusion safely under any circumstances.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 457 — Venomous Snakebites (textbook)
- API Textbook of Medicine, 10th ed. — Chapter on Envenomation (textbook)
- WHO Guidelines for the Management of Snakebites in South-East Asia, 2nd ed., 2016 (guideline)
- National Snakebite Management Protocol, Ministry of Health and Family Welfare, India, 2008 (revised) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old paddy farmer arrives 90 minutes after a suspected Russell's viper bite. His gums are bleeding, blood drawn for the IV cannula does not clot, and the 20WBCT shows no clot at 20 minutes. You recognise this immediately: venom-induced consumption coagulopathy. You reach for the antivenom. The pharmacy stocks polyvalent anti-snake venom (ASV). But as you begin to prepare the infusion, the nurse asks three questions you realise you have never been clearly taught the answers to: 'How many vials? How fast do we give it? And what do we do if the patient starts to wheeze ten minutes in?' You know antivenom is the only cure. You do not know the dose, the rate, or the anaphylaxis protocol. Now you do not just have a critically envenomated patient — you have an antivenom infusion you are not confident to run. This module closes that gap.
WHY THIS MATTERS
Anti-snake venom is the single definitive treatment for systemic envenomation — nothing else reverses VICC, stops neurotoxic paralysis from progressing, or treats the direct tissue destruction of viper venom. Yet antivenom is among the most under-used and most incorrectly administered treatments in Indian emergency medicine. Studies from India document delays of 6–24 hours from presentation to first dose, sub-therapeutic dosing, and antivenom given for indications it does not treat (local swelling alone). NMC competency IM21.7 requires you to enumerate the indications, describe the pharmacology, specify the dose, and explain the adverse reactions and hypersensitivity management — because knowing when, how much, how fast, and what to do if it goes wrong is the complete competency. An internist who knows the indication but gives the wrong dose, or who withholds antivenom because they fear anaphylaxis without knowing how to treat it, has delivered incomplete care.
RECALL
Activate prior knowledge. Recall from immunology that antisera are raised by immunising horses with sub-lethal doses of venom; the resulting equine IgG antibodies are purified to form antivenom (or anti-snake venom, ASV). Because ASV is a foreign protein (equine), it carries a risk of immediate hypersensitivity (anaphylaxis, anaphylactoid reactions) and late serum sickness. Recall from pharmacology that adrenaline (epinephrine) is the first-line treatment for anaphylaxis — it acts on alpha-1 receptors to reverse vasodilation and on beta-2 receptors to reverse bronchospasm. Recall from pathophysiology that VICC (venom-induced consumption coagulopathy) is a state of defibrination; antivenom neutralises the circulating venom enzymes and arrests further factor consumption, but it cannot instantly replace already-consumed fibrinogen — recovery of coagulation takes 6–24 hours as the liver synthesises new factors. This means the 20WBCT will still be positive for several hours post-antivenom even if the correct dose has been given.
Pharmacology of Polyvalent Anti-Snake Venom
Polyvalent anti-snake venom (ASV) is the biological product manufactured in India by immunising horses with a mixture of venoms from the four medically significant Indian snakes: Russell's viper (Daboia russelii), saw-scaled viper (Echis carinatus), Indian cobra (Naja naja), and common krait (Bungarus caeruleus). 'Polyvalent' indicates that a single product contains antibodies against all four species — it is the only antivenom commercially produced and stocked in India and is the standard treatment regardless of which of the big four is suspected. The product is manufactured by the Central Research Institute (CRI) Kasauli, the Haffkine Institute Mumbai, and King Institute of Preventive Medicine Chennai.
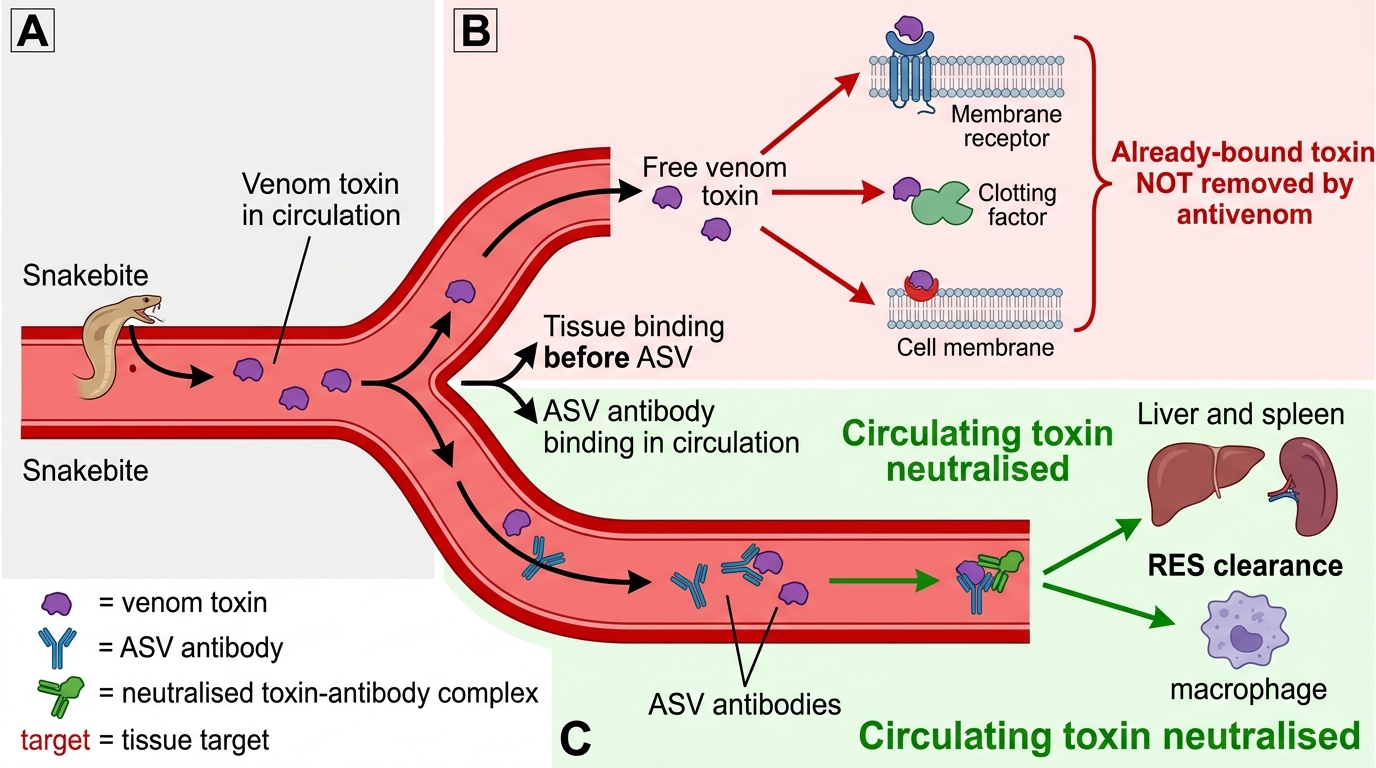
Mechanism of action: ASV works by direct antibody-mediated neutralisation of venom toxins. The equine IgG antibodies bind to the toxin proteins in the patient's circulation, forming antigen-antibody complexes that are cleared by the reticuloendothelial system. This neutralisation prevents further enzyme-substrate interaction: the prothrombin activators in viper venom can no longer activate clotting factors, the alpha-neurotoxins can no longer bind additional acetylcholine receptors, and the phospholipases can no longer damage cell membranes. However — and this is critically important — antivenom can only neutralise circulating (unbound) venom. Toxin that has already bound to its tissue target (receptor, enzyme, cell membrane) is not removed by ASV. This is why rapid administration matters: the sooner ASV is given after envenomation, the more circulating venom is neutralised before it reaches its tissue targets. The corollary is that ASV can stop coagulopathy from worsening but cannot instantly restore already-consumed clotting factors; it can halt further paralysis but cannot reverse already-established neuromuscular blockade.
Pharmacokinetics: ASV distributes in the vascular compartment. The half-life of equine IgG is approximately 5–7 days. After administration, the antigen-antibody complexes are cleared over hours to days. Antivenom does not cross the blood-brain barrier in significant quantities, which is why it is ineffective against already-established presynaptic neurotoxicity at the brainstem level.
Species coverage: Polyvalent Indian ASV covers all four big four species but does NOT cover king cobra (Ophiophagus hannah), sea snakes, or exotic species. Regional specific antivenoms exist for specific circumstances but are not in general hospital stock.
Mechanism of Antivenom Action
Indications for Antivenom: When to Give and When to Withhold
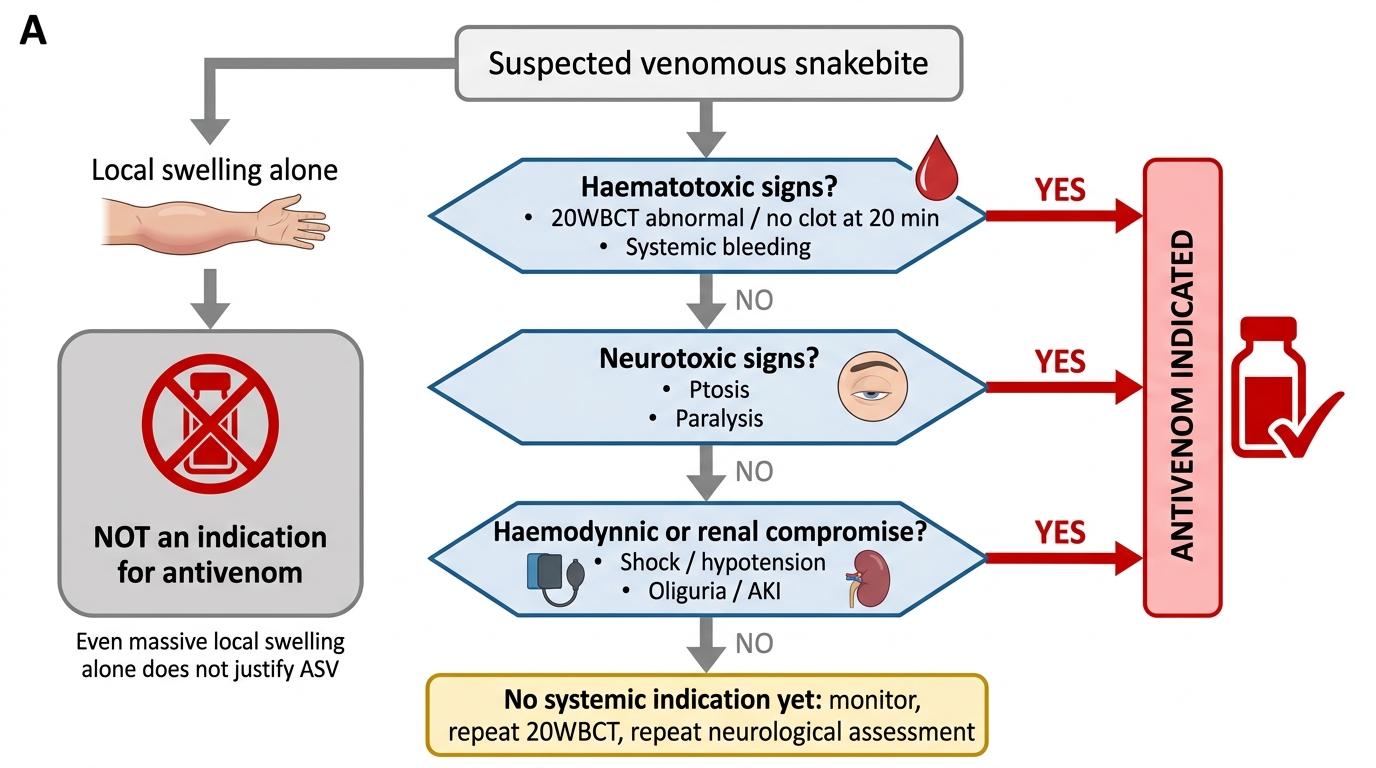
The most important clinical decision in snakebite management is whether the patient meets an indication for antivenom administration. Anti-snake venom is not a routine treatment for every snakebite — it is a biological product with real risks (anaphylaxis, serum sickness) and it should only be given when there is clear evidence of systemic envenomation. Equally important is the recognition that antivenom must NOT be withheld from a patient with systemic envenomation out of fear of adverse reactions, because the risk of death from untreated envenomation exceeds the risk of managed anaphylaxis in every case. The clinician who understands the indications precisely is the one who gives antivenom to every patient who needs it while sparing those who do not from a dangerous unnecessary infusion. Two equally serious errors are made in practice: giving antivenom for local swelling alone (needless exposure to anaphylaxis risk), and withholding it in true VICC out of fear (preventable death from haemorrhage or respiratory failure). Both errors are corrected by memorising the indication list. The indications are as follows.
Absolute indications (any one criterion is sufficient):
- Haematotoxic envenomation — Coagulopathy: A positive 20-minute whole-blood clotting test (20WBCT) — no clot formed at 20 minutes in a clean, dry glass tube. This is the most commonly applied indication in viper envenomation. It signifies VICC and is independently life-threatening (intracranial haemorrhage, uncontrolled visceral bleeding). Formal coagulation studies showing prolonged PT/INR, low fibrinogen, or elevated D-dimer are confirmatory but the 20WBCT alone is sufficient to initiate treatment.
- Haematotoxic envenomation — Spontaneous systemic bleeding: Active bleeding from any site that is not explained by a local wound — gingival oozing, epistaxis, haematuria, haematemesis, conjunctival haemorrhage, or blood at venepuncture sites. The presence of spontaneous bleeding means VICC is already clinically manifest; antivenom is indicated immediately without waiting for the 20WBCT result.
- Neurotoxic envenomation — Any sign of neurotoxicity: Ptosis (eyelid drooping), ophthalmoplegia, bulbar palsy (nasal voice, dysphagia), neck flexion weakness, or respiratory muscle compromise. Any neurotoxic sign is an indication for antivenom because the progression from ptosis to respiratory arrest can occur over hours and antivenom halts further toxin binding to unreached receptors. Established paralysis will not be immediately reversed, but the natural history of unresisted progression is fatal.
- Haemodynamic instability: Hypotension, shock, or cardiovascular compromise attributable to envenomation — viper venoms can cause direct vasodilation and distributive shock.
- Acute kidney injury attributable to envenomation: Rising serum creatinine in the context of snakebite, particularly Russell's viper, is an indication for antivenom to neutralise circulating nephrotoxic venom components.
NOT an indication for antivenom:
- Local swelling alone — even extensive swelling of the bitten limb — is NOT an indication for ASV. Local oedema is caused by locally acting enzymes already deposited at the bite site; circulating antivenom cannot reach and neutralise venom already fixed in tissue. Giving ASV for local swelling alone exposes the patient to anaphylaxis risk without therapeutic benefit. The only exception is rapidly expanding swelling threatening the airway (e.g., bite on the neck or face with airway oedema).
- Pain at the bite site alone — not an indication.
- Dry bite — no envenomation, no indication.
Antivenom Indication Decision Flowchart
SELF-CHECK
A 40-year-old man is bitten by a snake on the right forearm. He has swelling of the entire right arm from wrist to shoulder (massive local envenomation). His 20WBCT shows a normal clot at 20 minutes, there is no gingival bleeding, no ptosis, and he is haemodynamically stable. Should antivenom be administered?
A. Yes — the massive local swelling indicates severe envenomation requiring antivenom
B. Yes — all patients with significant swelling after a suspected venomous bite should receive antivenom
C. No — local swelling alone is not an indication for antivenom; monitor with serial 20WBCT and repeat neurological assessment
D. No — antivenom is only indicated if the species is positively identified as a viper
Reveal Answer
Answer: C. No — local swelling alone is not an indication for antivenom; monitor with serial 20WBCT and repeat neurological assessment
Local swelling, even massive, is not an indication for antivenom. Antivenom neutralises circulating venom; the venom responsible for local tissue injury has already deposited in tissue and cannot be reached by systemic antivenom. Giving ASV for local swelling alone exposes the patient to anaphylaxis risk without benefit. The correct management is close monitoring: serial 20WBCT every 30–60 minutes for 6 hours, serial neurological examination, and haemodynamic monitoring. If any systemic sign develops (positive 20WBCT, bleeding, ptosis, hypotension), antivenom should then be given immediately. Species identification is not required — the indication is the syndrome.
Dose, Route, and Administration of Anti-Snake Venom
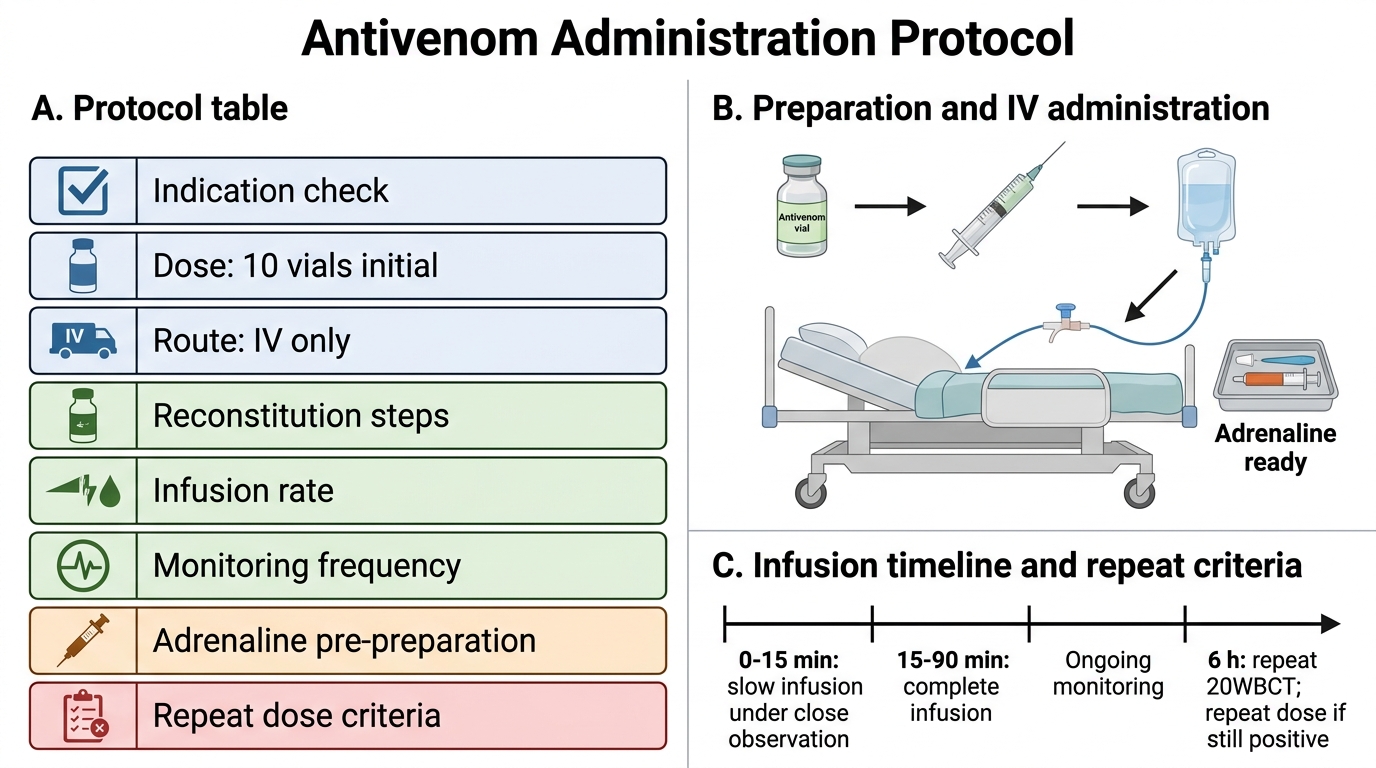
Correct administration of antivenom requires knowledge of the dose, route, dilution, infusion rate, and the monitoring required during and after infusion. Errors in any of these dimensions — giving too few vials, infusing too fast, or monitoring inadequately — lead to preventable deaths or adverse events. The following protocol is based on the WHO snakebite management guidelines and the National Snakebite Management Protocol of India.
Standard initial dose: The recommended initial dose for systemic envenomation in adults and children (same dose regardless of body weight — venom neutralisation is based on venom quantity, not patient size) is 10 vials of polyvalent ASV, each vial typically containing lyophilised powder reconstituted to 10 mL, giving a total volume of 100 mL reconstituted ASV. Some formulations are liquid; check the package insert for vial content. In severe envenomation (positive 20WBCT, active bleeding, established neurotoxic signs), 10 vials as the initial dose is the minimum. Do not give fewer vials in children — children are not less envenomated because they are smaller; they may in fact have a proportionally higher venom load per kilogram.
Route: Always intravenous (IV) — never intramuscular (IM), never subcutaneous. IM administration results in erratic, delayed absorption and cannot achieve the rapid serum concentrations needed to neutralise circulating venom. IV is the only route proven effective.
Reconstitution and dilution: Reconstitute each vial with the diluent provided (typically 10 mL water for injection per vial). The reconstituted ASV (100 mL for 10 vials) is further diluted in 100–500 mL of normal saline (0.9% NaCl) or 5% dextrose for infusion. Do not use Ringer's lactate for dilution in coagulopathic patients (contains calcium).
Infusion rate: Begin the infusion slowly for the first 10–15 minutes — start at a rate of approximately 10–20 mL/min while observing the patient closely for early anaphylactic signs (urticaria, flushing, wheeze, hypotension). If no adverse reaction occurs after 15 minutes, the rate can be increased to complete the infusion over 60–90 minutes total. The slow initial rate allows time to detect and respond to early anaphylaxis before a large volume has been administered.
Monitoring during infusion: The patient must be under continuous direct observation during the entire antivenom infusion. Record vital signs (pulse, blood pressure, respiratory rate, SpO2) every 5 minutes for the first 30 minutes and every 15 minutes thereafter. Have adrenaline 0.5 mg (0.5 mL of 1:1000 solution) drawn up and immediately available before starting the infusion — this is non-negotiable. Have IV antihistamine (chlorphenamine 10 mg IV) and IV hydrocortisone (100–200 mg IV) ready but note these are adjunctive, not primary, for anaphylaxis.
Repeat dosing: If the 20WBCT remains positive at 6 hours post-antivenom, or if neurotoxic signs continue to progress or bleeding continues, a second dose of 10 vials may be given. There is no absolute maximum number of doses — dose sufficiency is guided by clinical response. In severe Russell's viper envenomation with persistent VICC, 20–30 total vials may be required. After antivenom, recovery of coagulation (fibrinogen synthesis by the liver) takes 6–24 hours; do not interpret a still-positive 20WBCT at 2 hours post-antivenom as evidence of inadequate dose — use the 6-hour mark as the assessment point.
Antivenom Administration Protocol