Page 5 of 27
IM22.2-3 | Plant and Corrosive Poisoning — SDL Guide (Part 2)
Corrosive Poisoning: Pathophysiology and Clinical Features
Corrosive poisoning results from ingestion (or exposure) to substances that cause direct chemical destruction of tissue on contact. In India, the most commonly ingested corrosives are mineral acids (hydrochloric acid / spirit of salt, sulphuric acid / battery acid) and alkalis (sodium hydroxide / caustic soda, potassium hydroxide, bleach/hypochlorite). Phenol and concentrated hydrogen peroxide are less common but also encountered. Each class causes tissue destruction by distinct mechanisms with important differences in the depth and extent of injury, which directly determine management.
Acid corrosives cause coagulative necrosis. The hydrogen ion denatures surface proteins, forming a firm eschar (slough) that self-limits further penetration. This is the pathological basis for the observation that acids tend to cause more severe injury to the stomach (particularly the antrum and pylorus) than to the oesophagus, because: (a) the oesophageal squamous mucosa is relatively more resistant than gastric mucosa; (b) the cardiac sphincter remains open during the rapid transit of a liquid bolus, allowing acid to pool in the stomach; and (c) the eschar formation limits transmural penetration. Clinical consequences of acid ingestion: severe burning pain in the mouth, throat, chest, and abdomen; nausea and vomiting (which may worsen injury — do NOT induce); oral and pharyngeal burns; haematemesis (severe gastric injury); gastric perforation (risk highest in pyloric injury → acute abdomen); and delayed pyloric stenosis (from scarring, weeks to months later).
Alkali corrosives cause liquefactive necrosis. The hydroxyl ion saponifies membrane lipids and solubilises proteins, causing a liquefying, penetrating injury that does not self-limit. This is why alkali injuries penetrate more deeply and the oesophagus bears the brunt of the injury — the oropharynx is exposed during swallowing, and the oesophagus is traversed slowly enough for sustained contact. Clinical consequences: severe burns of the lips, oral mucosa, oropharynx, and oesophagus; supraglottic oedema and laryngeal oedema (causing hoarseness, stridor, and airway emergency); oesophageal perforation (most dangerous acute complication); and delayed oesophageal stricture (the most common long-term complication, leading to dysphagia months after the acute event).
Clinical features of corrosive ingestion begin immediately: burning pain in the mouth, throat, chest, and abdomen; salivation and difficulty swallowing (dysphagia, odynophagia); hoarseness or complete loss of voice (laryngeal involvement); respiratory distress (stridor = supraglottic oedema, a critical sign); haematemesis; and in severe cases, features of perforation — peritonitis (tenderness, guarding, rigidity) or mediastinitis (severe chest pain, fever, surgical emphysema).
The severity of burn is graded endoscopically. The Zargar classification (modified) is widely used:
- Grade 0: normal
- Grade 1: mucosal oedema and erythema
- Grade 2a: superficial ulcers, blisters, exudates
- Grade 2b: deep discrete ulcers, or circumferential Grade 2a
- Grade 3a: multiple deep ulcers, areas of necrosis
- Grade 3b: extensive necrosis
Grade 2b and above carry significant risk of stricture formation; Grade 3 indicates risk of perforation and death.
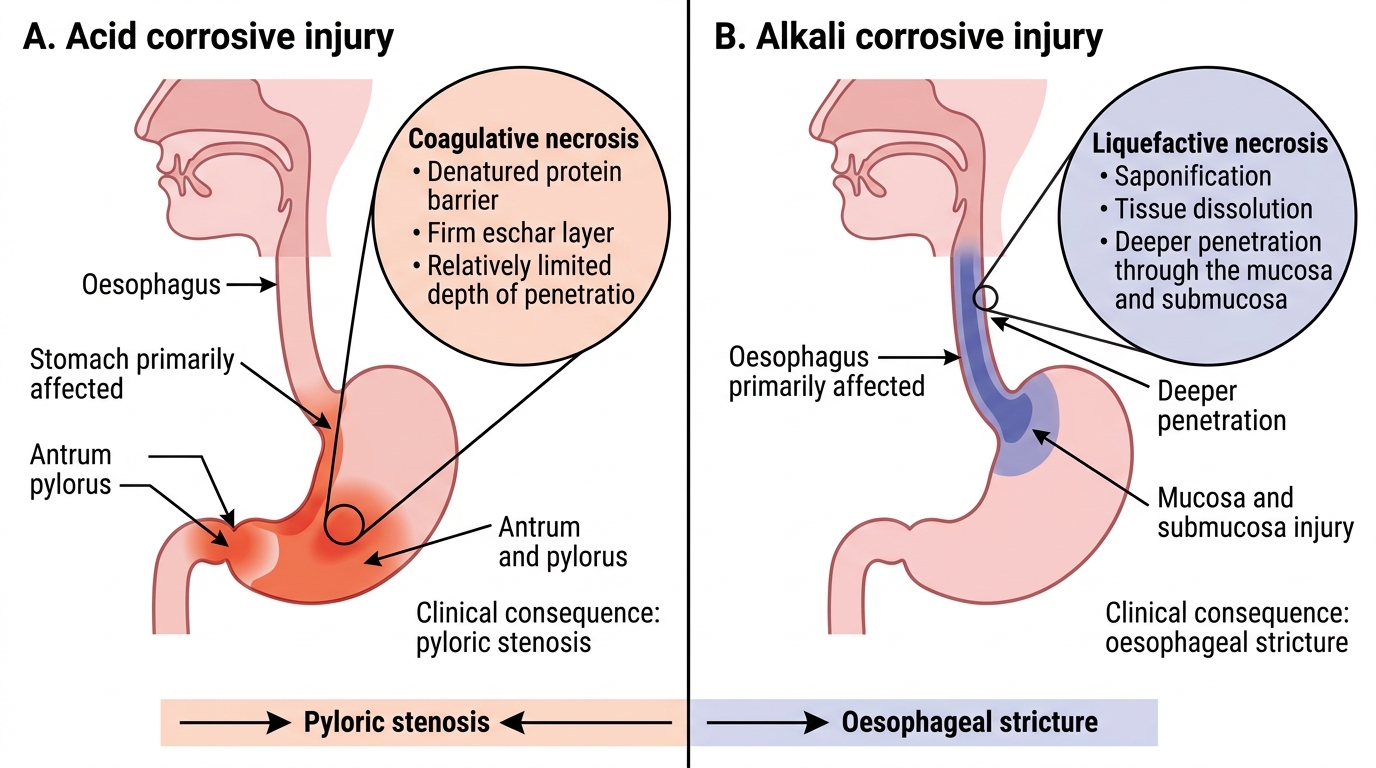
Acid vs Alkali Corrosive Injury
Management of Corrosive Poisoning
Corrosive poisoning management demands an immediate shift in the clinician's default toxicological reflexes, because every standard poisoning manoeuvre — inducing vomiting, giving activated charcoal, passing a nasogastric tube — is not merely unhelpful but actively dangerous in corrosive ingestion. The management is instead built around two absolute priorities: securing and protecting the airway (because supraglottic and laryngeal oedema from alkali burns can cause complete airway obstruction within minutes of ingestion, and death can occur before any other intervention is possible); and preventing additional chemical exposure by restricting what the patient swallows, avoiding procedures that re-expose damaged tissue, and deferring endoscopy to the optimal time window. Unlike other forms of poisoning, where gastrointestinal decontamination is a priority, in corrosive poisoning the gastrointestinal tract has already been damaged — the therapeutic goal is to limit ongoing injury, support the patient through the acute phase, grade the injury by endoscopy, and manage the predictable complications (perforation acutely, stricture chronically). The role of the emergency physician and the general medicine team is therefore to stabilise the patient, define the injury grade, and work in close partnership with the surgical and gastroenterology teams for definitive care.
Immediate assessment and stabilisation:
- Assess the airway immediately and continuously. Hoarseness, stridor, or drooling are signs of supraglottic or glottic oedema — these patients require emergency endotracheal intubation (using a flexible fibre-optic scope if available to avoid worsening mucosal injury) or, if intubation is not possible due to oedema, surgical tracheostomy or cricothyrotomy. Do not delay airway intervention.
- Administer high-flow oxygen.
- Establish IV access; give IV fluids (pain and vomiting cause dehydration).
- IV morphine or fentanyl for pain control — adequate analgesia is a priority.
- NPO (nothing by mouth) — no oral fluids.
What NOT to do — critically important:
- NEVER induce vomiting — re-exposure of the oesophagus and airway to the corrosive during emesis worsens injury dramatically and can precipitate airway compromise.
- NEVER give activated charcoal — it does not adsorb corrosives and, crucially, it obscures the endoscopic view needed for grading injury.
- NEVER attempt to neutralise the acid with alkali or vice versa — exothermic (heat-generating) neutralisation reactions cause thermal injury superimposed on the chemical injury. Give small sips of water or milk to dilute only if the patient is awake and swallowing is possible — dilution not neutralisation.
- NEVER pass a nasogastric tube blindly — risk of perforation.
Decontamination: Dilution with water or milk (100–250 mL) can reduce the corrosive burden if given within minutes of ingestion and if the patient is alert and able to swallow. Skin/eye exposure: copious irrigation with water for at least 20–30 minutes.
Investigations:
- Bloods: FBC, renal function, LFTs, coagulation, ABG (metabolic acidosis in severe injury; systemic absorption in phenol/bleach ingestion).
- Chest X-ray: surgical emphysema (subcutaneous air) or pneumomediastinum suggests oesophageal or tracheal perforation — a surgical emergency.
- CT scan chest/abdomen if perforation is suspected (more sensitive than CXR for pneumomediastinum and free air).
Endoscopy:
- Upper GI endoscopy (rigid or flexible) is the gold standard for grading mucosal injury and predicting risk of stricture and perforation. Timing: optimal at 12–48 hours after ingestion — early enough to grade before inflammation obscures the injury, late enough for haemodynamic stabilisation and initial oedema reduction. Endoscopy is contraindicated in the first 24 hours (maximum oedema/friability) and after 5 days (risk of perforation as sloughing progresses).
- Grade 2b and Grade 3 injuries require close surgical monitoring.
Corticosteroids: previously used to prevent oesophageal stricture — current evidence does NOT support routine steroid use for stricture prevention; their use increases infection risk. They may be considered for severe laryngeal oedema with airway compromise (Grade 2b–3 supraglottic burns), but the evidence is weak.
Surgical referral: indicated for evidence of perforation (peritonitis, pneumomediastinum), haemorrhage not responding to conservative management, or full-thickness (Grade 3) necrosis requiring resection.
Long-term prognosis and follow-up: Oesophageal stricture is the most common long-term complication (affecting 15–40% of Grade 2b and Grade 3 oesophageal injuries). It manifests as progressive dysphagia weeks to months after the acute event. Management: serial oesophageal dilatation (bougienage). Patients with severe injuries should be followed by gastroenterology and the surgical team.
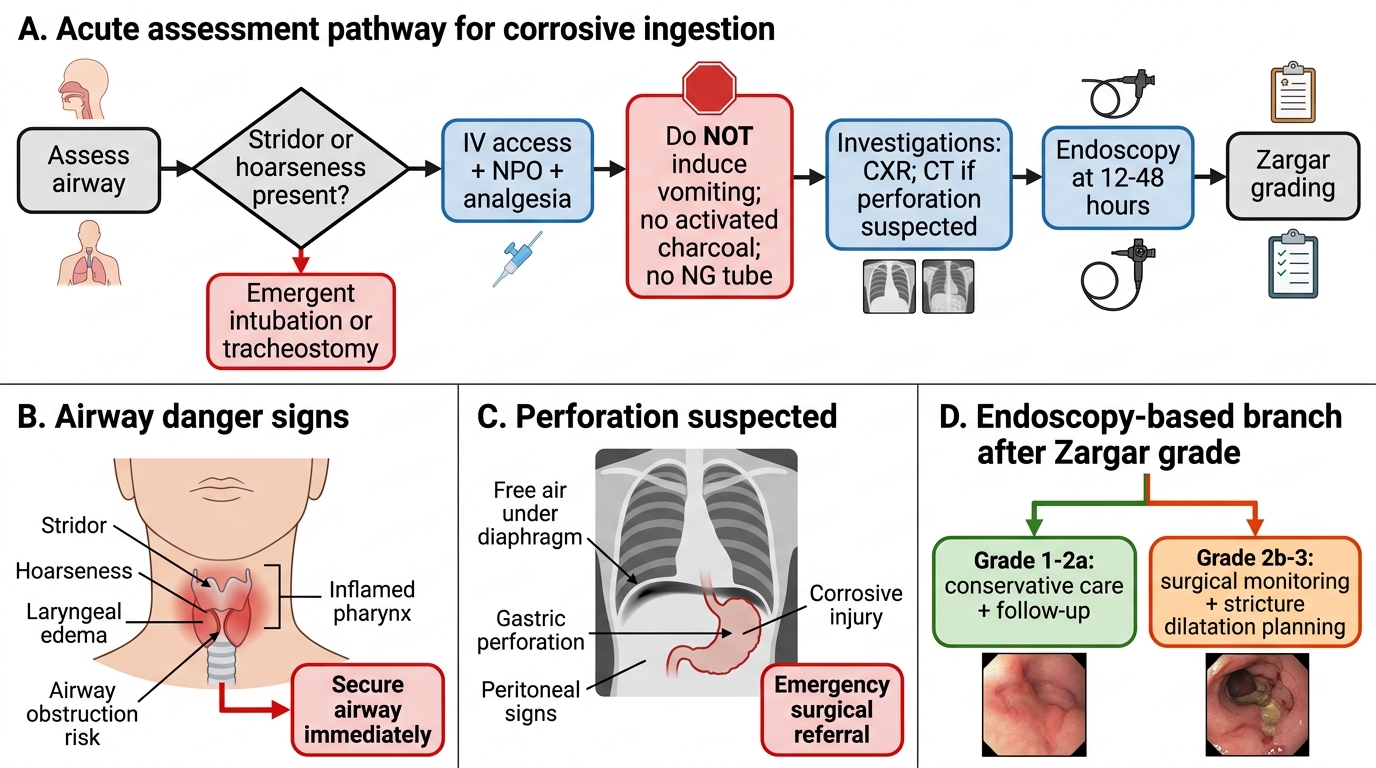
Acute Management Algorithm for Corrosive Ingestion
SELF-CHECK
A 23-year-old man ingests approximately 100 mL of concentrated sulphuric acid (battery acid). He arrives conscious but in severe pain, with haematemesis and peritoneal signs on examination. Chest X-ray shows free air under the diaphragm. Which of the following is the MOST appropriate next step?
A. Administer activated charcoal via nasogastric tube immediately
B. Perform upper GI endoscopy within the next hour
C. Emergency surgical referral for suspected gastric perforation
D. Induce vomiting to clear the acid from the stomach
Reveal Answer
Answer: C. Emergency surgical referral for suspected gastric perforation
Free air under the diaphragm on CXR indicates gastric or intestinal perforation — a surgical emergency. Acid ingestion (sulphuric acid) causes coagulative necrosis predominantly in the stomach (antrum and pylorus), and perforation is the most dangerous acute complication. Immediate emergency surgical referral for laparotomy is the correct response. Activated charcoal is CONTRAINDICATED in corrosive poisoning (does not adsorb corrosives; obscures endoscopy). Endoscopy is contraindicated in suspected perforation. Inducing vomiting is absolutely contraindicated in all corrosive ingestion (re-exposes airway and oesophagus).
Prognosis and Prevention
Understanding the prognostic factors in plant and corrosive poisoning helps the clinician counsel patients and families accurately, plan long-term follow-up, and advocate for preventive measures.
Provided image
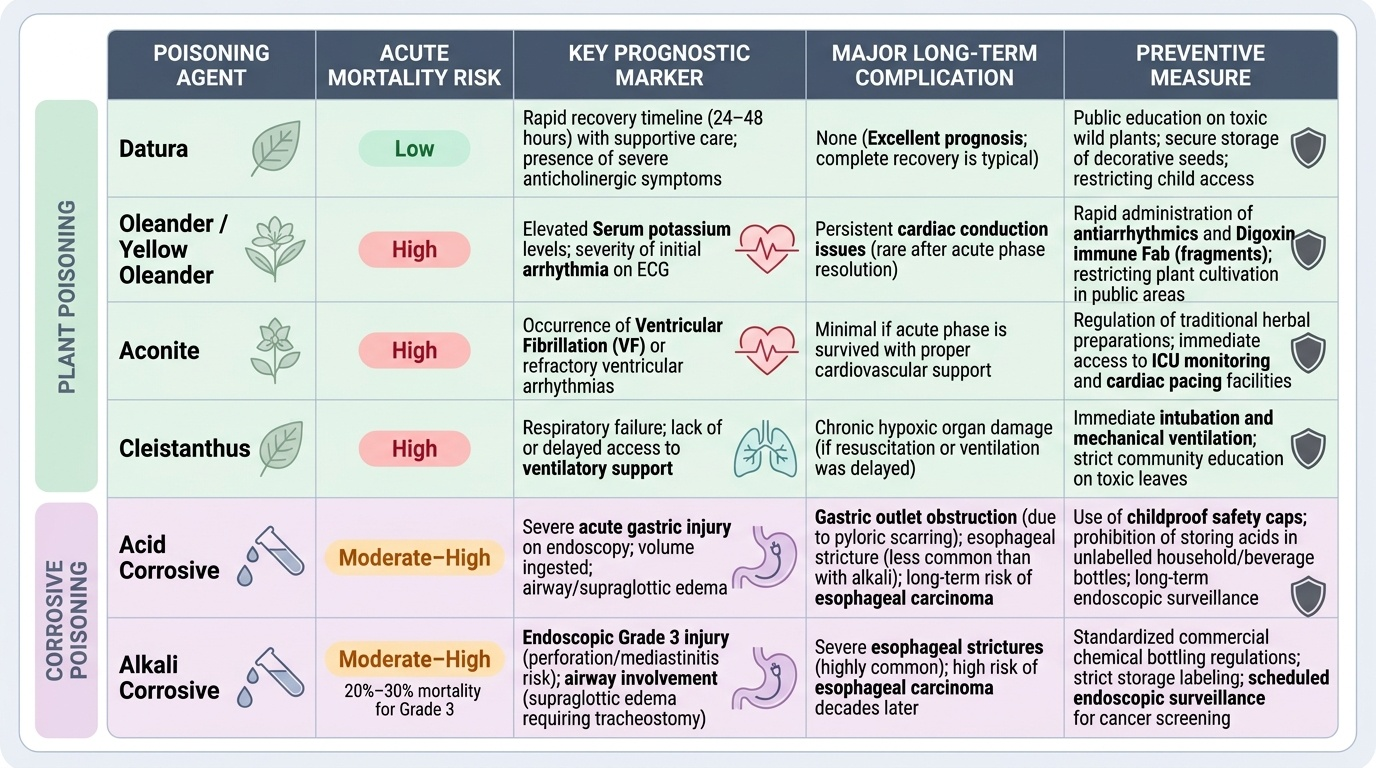
For plant poisoning, prognosis is largely determined by: (1) the specific toxin (oleander and aconite carry higher mortality than Datura; Cleistanthus has high mortality without ventilatory support); (2) the time to presentation and institution of specific therapy (particularly antiarrhythmic therapy and Fab fragments for cardiac glycoside poisoning); (3) the severity of cardiac involvement (serum potassium and initial arrhythmia are the most important prognostic markers for oleander; presence of VF for aconite); and (4) access to ICU care, cardiac monitoring, and pacing facilities. The majority of Datura cases recover fully within 24–48 hours with supportive care alone.
For corrosive poisoning, the determinants of prognosis are: (1) the type of corrosive (alkali is associated with worse long-term oesophageal complications than acid; concentrated acids cause more acute gastric injury); (2) the volume ingested; (3) the endoscopic grade of injury (Grade 3 injuries have mortality approaching 20–30% from perforation and mediastinitis; Grade 1 injuries have an excellent prognosis); and (4) airway involvement (supraglottic oedema requiring tracheostomy is an independent predictor of poor outcome).
Long-term complications include: oesophageal stricture (acid and alkali, more common with alkali); gastric outlet obstruction from pyloric scarring (acid more than alkali); oesophageal carcinoma (a long-term risk after severe corrosive oesophagitis — increased risk over decades, necessitating long-term endoscopic surveillance).
Prevention is a crucial public health dimension. In India, the following measures are relevant: mandatory child-resistant closures for household chemicals (bleach, caustic soda); safe storage of agricultural pesticides and industrial chemicals; community awareness about Datura toxicity (seeds and leaves are toxic, not just berries); regulation of traditional herbal preparations containing Aconitum (detoxification protocols are inconsistent); restriction of access to corrosives for individuals with known mental illness or suicidal ideation; and poison centre helplines (AIIMS Poison Management Centre: 1800-116-117) for first-aid advice. The physician's responsibility extends beyond the bedside to community education and preventive advocacy.
SELF-CHECK
A 45-year-old woman is brought in 90 minutes after ingesting sodium hydroxide (drain cleaner). She is hoarse, drooling, and in severe pain. SpO₂ 91% on room air. No peritoneal signs. Which combination of management steps is CORRECT?
A. Induce emesis + activated charcoal + immediate rigid endoscopy
B. Ensure airway (intubate if needed) + IV analgesia + NPO + endoscopy at 12-48 hours
C. Neutralise with oral dilute acid + activated charcoal + chest X-ray
D. Nasogastric tube for gastric lavage + corticosteroids + immediate endoscopy
Reveal Answer
Answer: B. Ensure airway (intubate if needed) + IV analgesia + NPO + endoscopy at 12-48 hours
Alkali (sodium hydroxide) causes liquefactive necrosis with risk of supraglottic oedema and oesophageal perforation. The correct management is: (1) prioritise airway — hoarseness and low SpO₂ indicate imminent airway compromise; prepare for intubation via fibre-optic or surgical airway; (2) IV analgesia; (3) NPO; (4) endoscopy should be scheduled at 12–48 hours (not immediately — maximum oedema/friability at <24 hours; endoscopy at >5 days risks perforation). NEVER induce emesis (re-exposes airway). NEVER give activated charcoal (doesn't adsorb; obscures endoscopy). NEVER neutralise (exothermic reaction). NEVER pass NGT blindly (perforation risk). Steroids are not routinely recommended for stricture prevention.
CLINICAL PEARL
The single most dangerous error in corrosive poisoning management is inducing vomiting — it re-exposes the already-burned oesophagus and larynx to the corrosive and can precipitate complete airway obstruction. Train yourself to pause on every corrosive case: NO emesis, NO charcoal, NO NG tube, NO neutralisation. The only permissible oral administration is small volumes of water or milk for dilution, and only if the patient is fully conscious and able to swallow.
For plant cardiac glycoside poisoning (oleander), remember that serum potassium at presentation is the single best bedside prognostic marker: K > 5.5 mEq/L in oleander poisoning is associated with high mortality and is an absolute indication for Fab fragment therapy. Do not wait for a serum digoxin level (the cross-reactive assay is useful but may not be available immediately) — treat on clinical grounds.