Page 20 of 27
IM22.9-13 | Poison Centre and Medico Legal Workflow — SDL Guide (Part 2)
Counselling the Family of a Poisoning Patient
Family counselling in the context of a poisoning admission is a complex clinical and communication task that requires simultaneous management of medical information sharing, emotional support, and — in cases of deliberate self-harm — careful navigation of stigma, guilt, and safety planning. The family's initial encounter with a physician at the emergency department or ICU forms the foundation of the therapeutic alliance that will be essential for the patient's long-term recovery and compliance with psychiatric follow-up. Poorly conducted family communication at this stage causes lasting harm: it can entrench family guilt, delay appropriate psychiatric care, and reduce the patient's chance of receiving post-discharge support.
Provided image
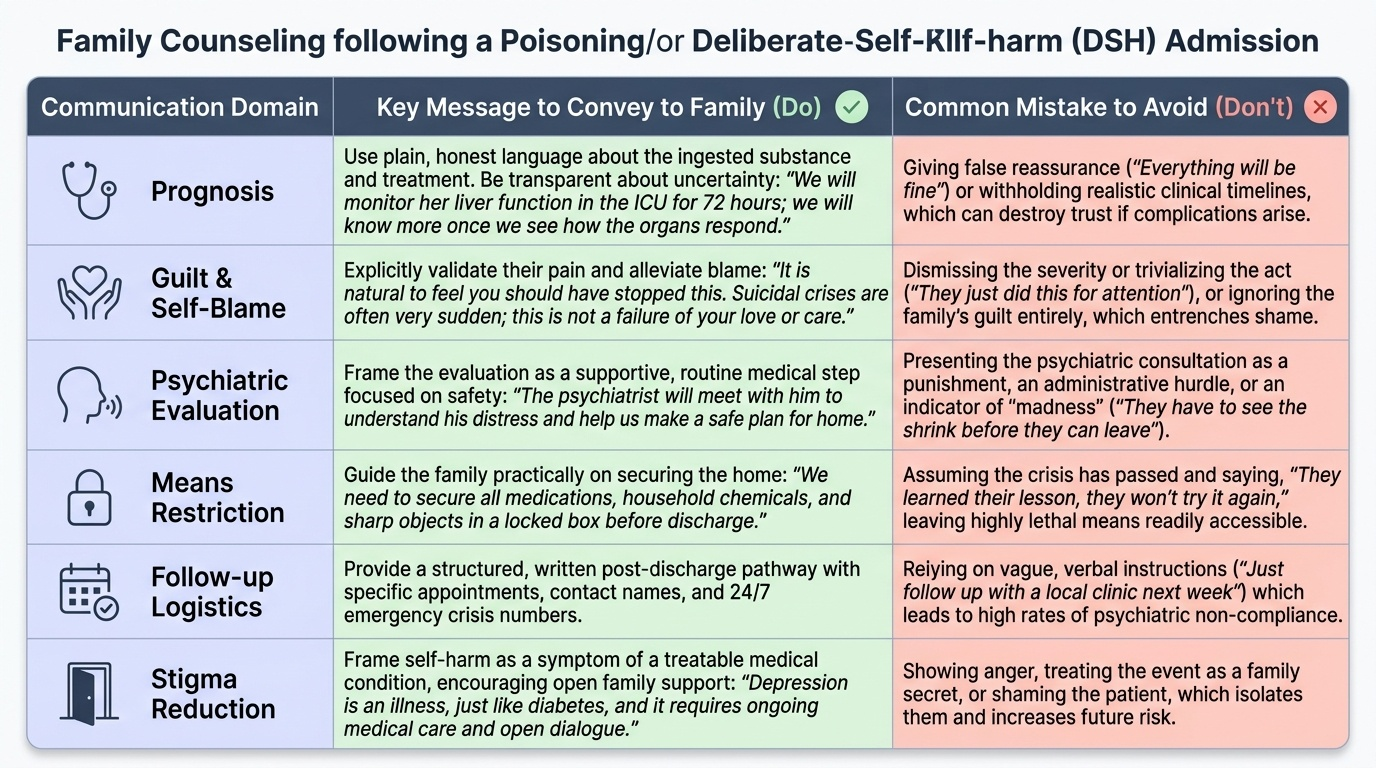
Principles of family counselling in poisoning:
1. Privacy and confidentiality: Counsel the family in a private space, not the corridor or waiting room. Identify the key family member (usually the person most closely connected and most likely to be involved in ongoing care).
2. Clear communication about prognosis: Use plain language. Explain the substance ingested (as far as known), the treatment given, and the expected clinical course. Be honest about uncertainty — it is better to say 'we will have more information in 48 hours once we see how the liver function responds' than to give false reassurance. Explain any expected complications or observation requirements: 'We will keep her in the ICU for 72 hours to watch for delayed liver damage from the paracetamol.'
3. Address family guilt without false reassurance: In DSH cases, families almost universally feel guilt, self-blame, and helplessness. Acknowledge these feelings explicitly: 'It is very natural to feel like you should have seen this coming or stopped it — many families feel that way. Suicidal crises are often very sudden, and it is not a failure of love or attention that this happened.' Do NOT offer false reassurance: 'Everything will be fine' or 'She just did this for attention' are both harmful — the first may prove wrong, the second trivialises a medical emergency.
4. Explain the psychiatric follow-up pathway: In DSH cases, the family must understand that: (1) the patient will be evaluated by a psychiatrist before or shortly after discharge; (2) the evaluation is not a punishment or a legal action — it is a clinical assessment of mental health needs; (3) their cooperation (sharing information with the psychiatrist, supporting attendance at follow-up appointments) is essential for recovery. Under MHCA 2017, the patient must be referred for psychiatric assessment; the family's role is to facilitate, not to resist.
5. Safety planning and means restriction: In DSH cases, a critical family counselling task is means restriction — reducing access to the method used or other available methods of self-harm. Discuss with the family: storing medications in a locked cabinet; removing pesticides from accessible storage; having a responsible family member manage medications for a patient who has overdosed on prescription drugs. This conversation must be tactful but explicit.
6. Avoid stigmatising language: Do not use terms like 'attention-seeking', 'dramatic', 'tried to scare everyone', or 'selfish' in family counselling. These terms reflect common but harmful misconceptions about DSH and reduce the family's ability to support the patient.
Psychiatric Consultation: Indications and Referral Process
Psychiatric consultation is a mandatory component of the management of poisoning cases involving deliberate self-harm (DSH) and cases where substance use disorder has contributed to the poisoning event. The treating physician's role is to recognise the indications for psychiatric referral, initiate the referral promptly, and provide the psychiatry team with the clinical context they need to conduct an effective assessment. Psychiatric consultation is not the end of the treating physician's involvement — it is a parallel track that runs alongside medical management and begins before discharge.
Mandatory indications for psychiatric consultation in poisoning:
1. Deliberate self-harm (DSH) — all cases: Any poisoning that is intentional (patient states or implies they ingested the substance to harm themselves, or where DSH is the clinically apparent motivation) must be referred for psychiatric assessment before discharge. This is mandated by the Mental Healthcare Act (MHCA) 2017, which requires that persons who attempt suicide be presumed to be under severe stress and must be provided mental health treatment. Discharge without psychiatric assessment is a legal and ethical breach. DSH includes all methods — not just ingestion — but in poisoning practice, a large proportion of cases are DSH.
2. Substance use disorder: When poisoning is the result of chronic substance abuse (alcohol, opioids, benzodiazepines, inhalants), psychiatric evaluation is needed to assess for underlying substance use disorder, comorbid psychiatric illness (depression, PTSD, schizophrenia), and to initiate the addiction medicine and de-addiction pathway.
3. Altered mental status beyond the toxidrome: When the patient's mental state after clinical stabilisation is inconsistent with the expected recovery from the toxin (persistent confusion, agitation, psychosis, or severe depressive symptoms after physical recovery), psychiatric evaluation is needed to assess for organic mental disorders, adjustment disorders, or acute psychiatric illness unmasked or precipitated by the poisoning event.
4. Homicidal poisoning victim: A patient who has been poisoned by another person has experienced significant psychological trauma in addition to physical toxicity; psychiatric evaluation addresses acute stress disorder, PTSD risk, and safety planning (returning to an environment with the perpetrator).
5. Repeated presentations: A patient with a second or subsequent poisoning admission, regardless of stated intent, should be referred for psychiatric assessment — recurrent self-harm or recurrent accidental poisoning in the context of impaired judgement both require formal evaluation.
How to refer: the psychiatric consultation request:
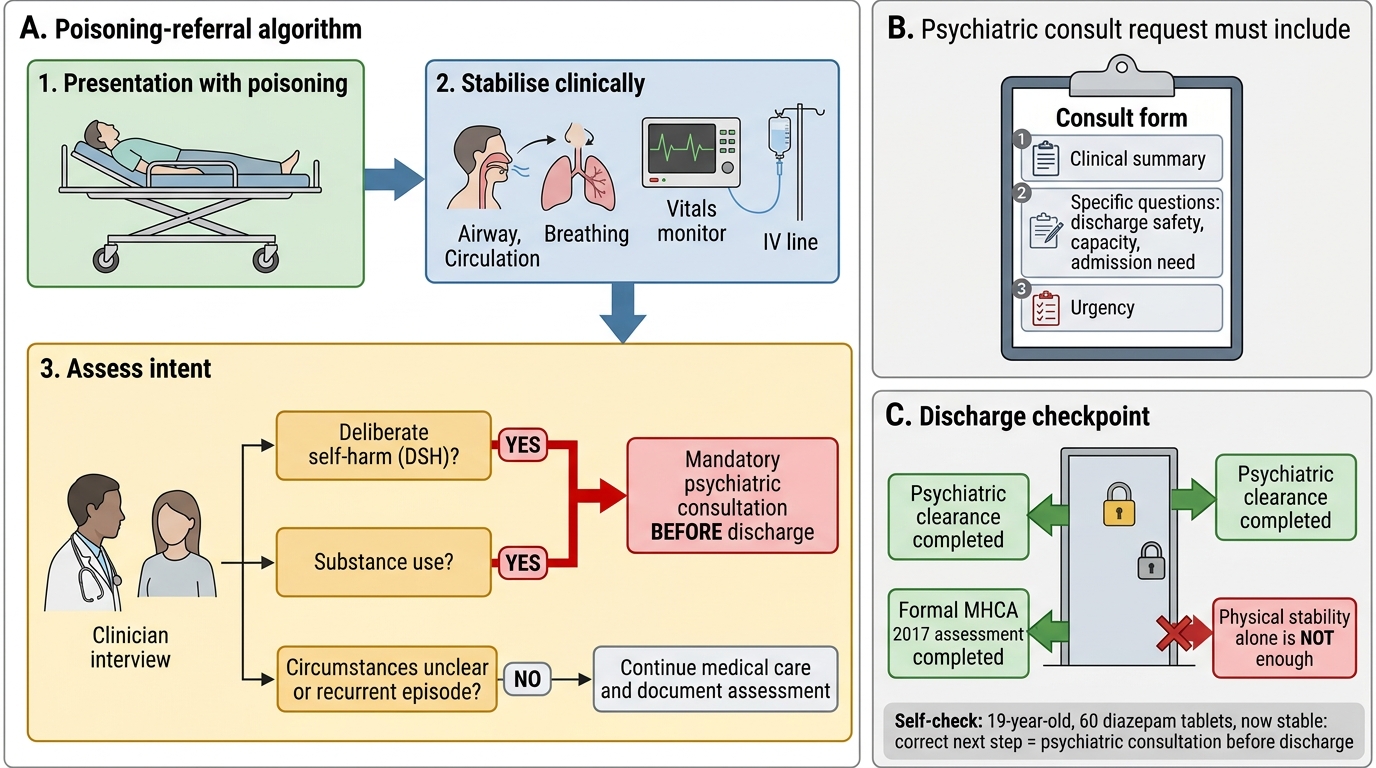
A psychiatric consultation request must include: (1) the reason for the referral (DSH, substance use, altered mental status); (2) the clinical summary (substance ingested, treatment, current status, GCS, ability to communicate); (3) specific questions for the psychiatrist (Is the patient safe for discharge? Does the patient have decision-making capacity? Does the patient require involuntary inpatient psychiatric admission under MHCA 2017?); (4) the urgency (immediate — patient is actively suicidal; routine — patient has stabilised and is appropriate for ward-based assessment).
The MHCA 2017 framework: Under MHCA 2017, a person who attempts suicide shall be presumed to be under severe stress and shall not be tried and punished under Section 309 IPC (decriminalisation of attempted suicide). The government has a positive obligation to provide mental health care to a person who attempts suicide. This framework means that a physician who discharges a DSH patient without psychiatric evaluation may be failing a statutory duty of care. The MHCA 2017 also empowers the patient — the patient has the right to make advance directives about their own mental health care, and has the right to refuse a specific treatment (though not the right to refuse all life-saving emergency care).
Psychiatric Referral Before Discharge in Poisoning
SELF-CHECK
A 19-year-old student is admitted after consuming 60 tablets of diazepam. She is now alert and haemodynamically stable, 24 hours after admission. The resident physician tells the family 'She will be fine, she can go home this evening.' The family is relieved and asks to take her home. What is the CORRECT next step?
A. Psychiatric consultation must be completed before discharge — DSH is a mandatory indication for psychiatric referral under MHCA 2017; discharging without assessment is a breach of legal and ethical duty
B. Discharge is appropriate because she is now physically stable and the benzodiazepine effect has resolved
C. Discharge with an outpatient psychiatry appointment in 2 weeks is adequate — psychiatric consultation does not need to be completed during the admission
D. Ask the family to sign a discharge-against-medical-advice form to protect the hospital from liability
Reveal Answer
Answer: A. Psychiatric consultation must be completed before discharge — DSH is a mandatory indication for psychiatric referral under MHCA 2017; discharging without assessment is a breach of legal and ethical duty
Deliberate self-harm is a MANDATORY indication for psychiatric consultation before discharge. The Mental Healthcare Act 2017 requires that a person who attempts suicide be provided mental health care and be presumed to be under severe stress. Discharge without psychiatric assessment is both a legal breach (MHCA 2017) and a clinical error — the psychiatrist's role is to assess suicide risk, underlying psychiatric illness, and the safety of discharge to the home environment. An outpatient appointment in 2 weeks is inadequate — the acute suicidal risk assessment must happen during this admission. Physical stabilisation does not substitute for psychiatric clearance. A DAMA form does not protect the hospital — a 19-year-old in a post-DSH state may not have full decision-making capacity for discharge decisions, and DAMA cannot override the MHCA 2017 obligation.
Applied Practice: Integrating the Five Competencies
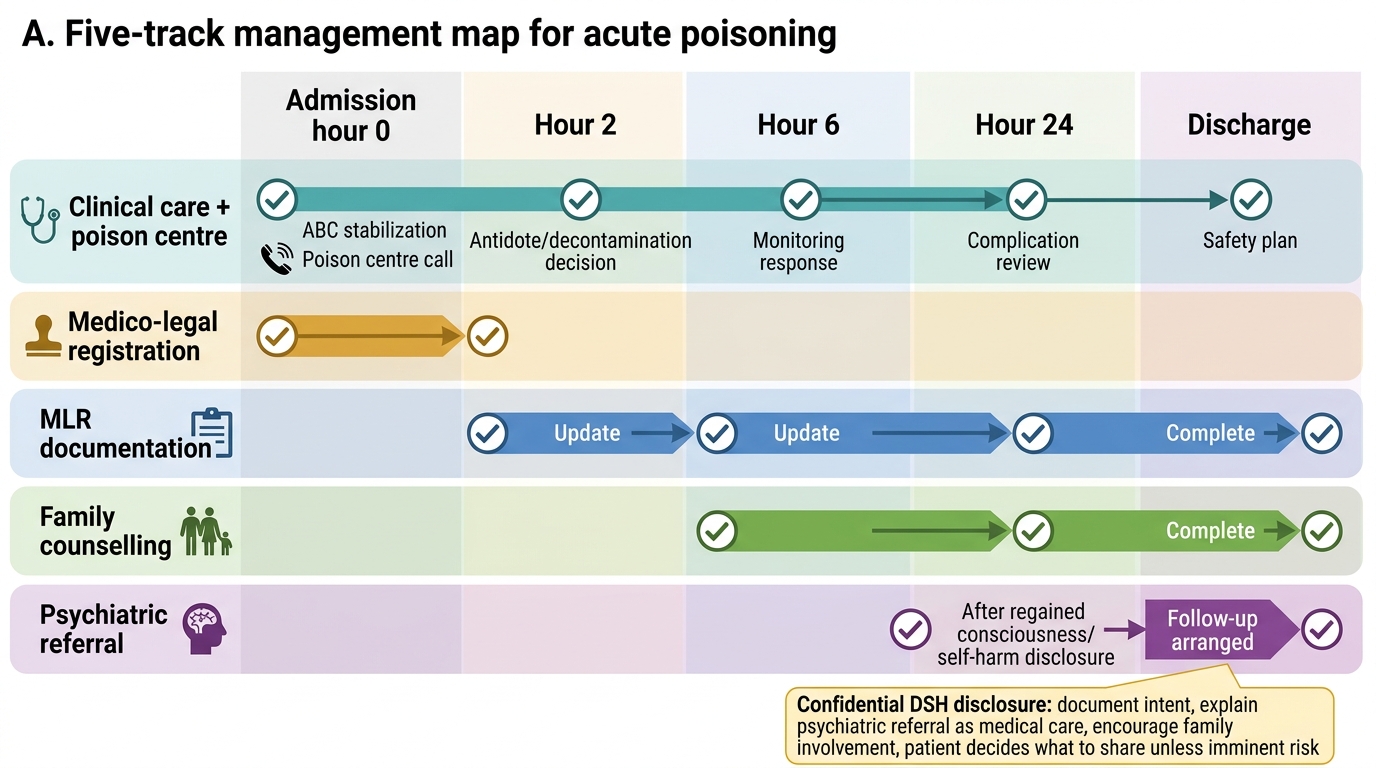
The five competencies covered in this module — poison centre contact, medico-legal management, MLR writing, family counselling, and psychiatric referral — are not sequential steps but parallel tasks that run simultaneously from the moment the patient is admitted. A skilled junior doctor manages all five tracks concurrently, in the correct priority order (treatment first, documentation concurrent, counselling and psychiatric referral initiated early). The following scenario integrates all five skills.
Integrated scenario: The 24-year-old farmer:
A 24-year-old male farmer is brought to the emergency department after his family found him unconscious in the field, next to an empty bottle of a common agricultural insecticide (organophosphate — brand name unfamiliar to the treating team). He is unresponsive, with pinpoint pupils, profuse secretions, bradycardia 42/min, and muscle fasciculations.
Track 1 — Clinical management + Poison Centre:
While the team initiates ABCDE resuscitation (oxygen, IV access, monitoring), the intern calls the Poison Control Helpline (1800-116-117) and reads out the brand name on the bottle. The toxicologist identifies the active ingredient as chlorpyrifos (organophosphate) and confirms: atropine IV to effect (dry secretions) + pralidoxime (within the first 12 hours) + ventilatory support. This confirms what the clinical team suspected and provides confidence to push atropine aggressively.
Track 2 — Medico-Legal:
The emergency MO registers this as an MLC (case number assigned). As circumstances of the poisoning are unclear (found alone in the field — accidental or deliberate?), police intimation is made via the standard form. Gastric lavage fluid is collected and labelled (1 sample for forensic analysis). The family is asked who found him and what they know.
Track 3 — MLR:
The SH documents: history as given by the wife ('found unconscious, empty bottle of [brand name] next to him'); clinical findings at admission with time; all investigations; treatment chronologically. The medical opinion section states: 'The clinical findings, including miotic pupils, secretory features, bradycardia, and cholinergic toxidrome, are consistent with organophosphate poisoning. Whether the ingestion was accidental or intentional cannot be determined from medical evidence alone and requires further investigation.'
Track 4 — Family counselling:
The wife is taken to a private area by the nurse and SH. The SH explains: he is in the ICU on life support, the treatment is started, he will be on the ventilator for probably 1–3 days while the poison is cleared from his system. She is told there may be complications (respiratory failure, prolonged weakness) and that the team will update her twice daily. Her distress is acknowledged. She discloses he had told her he was worried about his harvest failing and debt.
Track 5 — Psychiatric referral:
Based on the wife's disclosure of severe psychosocial stress and the possibility of DSH, the team flags the case for psychiatric review as soon as the patient regains consciousness and can communicate. The referral request is written: 'Suspected DSH in context of agricultural debt stress; please assess when patient is responsive; specific question: is this DSH, and what is the inpatient psychiatric management plan?'
Five-Track Management Map for Acute Poisoning
SELF-CHECK
In the integrated scenario above, the farmer regains consciousness on day 2. He tells you privately that he drank the pesticide deliberately because he could not repay a moneylender. His wife is in the room. He asks you not to tell her. What is the MOST appropriate response?
A. Tell him that you must refer him for psychiatric assessment as part of his medical care (which you would do for all serious poisoning cases) and that the psychiatrist will need his honest account to help him — the decision about what to share with his wife is his to make, but you encourage him to involve his family as it will help his recovery
B. Respect his confidentiality completely — do not tell the wife and do not document the DSH intent anywhere, as he asked you not to
C. Tell the wife immediately so she can supervise him and prevent a second attempt
D. Discharge him as soon as he is physically stable, as he is now competent and can make his own decisions about psychiatric care
Reveal Answer
Answer: A. Tell him that you must refer him for psychiatric assessment as part of his medical care (which you would do for all serious poisoning cases) and that the psychiatrist will need his honest account to help him — the decision about what to share with his wife is his to make, but you encourage him to involve his family as it will help his recovery
This question tests the balance between patient confidentiality and duty of care. Option A is correct: the psychiatric referral is mandatory (MHCA 2017, DSH) and does not require the patient to tell the wife — the physician can proceed with psychiatric consultation without disclosing the patient's disclosure to the family, while encouraging the patient's voluntary disclosure. The patient's confidentiality about the specific reason for the DSH (financial debt) should be respected, but the psychiatrist needs this information to conduct an effective assessment — explain to the patient that what he tells the psychiatrist is confidential. Option B is wrong — not documenting DSH intent and not referring for psychiatric assessment is a legal and ethical breach; concealing DSH intent from the clinical record creates patient safety and liability risks. Option C is wrong — disclosing against the patient's wishes without clinical necessity violates confidentiality; the wife will learn through the psychiatric process in a structured way. Option D is wrong — physical stability does not confer discharge clearance for a DSH patient; psychiatric assessment first.