Page 1 of 27
IM22.{1,5} | Poisoning Stabilisation and Toxidromes — SDL Guide
Learning Objectives
- Describe the systematic initial approach to stabilising the poisoned patient using the ABC framework and targeted history
- List the essential investigations in acute poisoning and interpret them in clinical context
- Identify the five major toxidromes (cholinergic, anticholinergic, sympathomimetic, opioid, sedative-hypnotic) from clinical findings
- Match toxidrome pattern to causative agent and immediate antidote where one exists
- Describe the principles of decontamination including indications and contraindications for activated charcoal
INSTRUCTIONS
Acute poisoning demands simultaneous stabilisation and diagnosis. This module teaches you to resuscitate the poisoned patient systematically, recognise the toxidrome pattern that points to the causative agent, and apply decontamination and antidote therapy in a logical sequence. These skills underpin competency IM22.1 (initial stabilisation) and IM22.5 (toxidrome recognition).
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 454 — Poisoning and Drug Overdose (textbook)
- API Textbook of Medicine, 10th ed., Ch. 26 — Poisoning (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 9 — Poisoning (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old man is brought to the emergency department by his family, unconscious, with a history of consuming something from the agricultural store an hour ago. On arrival: pulse 48 bpm, blood pressure 80/50 mmHg, pupils pinpoint and unresponsive, profuse sweating, salivation streaming from the corners of his mouth, and audible wheeze. His trousers are soaked in urine and there is faecal incontinence. Within 30 seconds of his arrival, a second patient is wheeled in from the same village — a 56-year-old woman, febrile at 39°C, tachycardic at 136 bpm, pupils maximally dilated, flushed dry skin, and confused, saying she ate wild berries. Same emergency room; two profoundly ill patients; two entirely different poisoning syndromes. Your clinical ability to recognise what each of these patients has — before any blood test returns, before any toxicology screen — determines the antidote you reach for in the next 60 seconds. One needs atropine and pralidoxime. The other needs supportive cooling and physostigmine consideration. Recognising the toxidrome is the difference between timely antidote therapy and a catastrophic delay.
WHY THIS MATTERS
Acute poisoning is one of the most common medical emergencies in India, accounting for a significant proportion of emergency department presentations across all tertiary care hospitals. The epidemiology in India is distinct: organophosphate and carbamate pesticides dominate agricultural regions, aluminium phosphide (celphos) is highly prevalent and carries near-100% mortality without early recognition, and paracetamol overdose is the most common pharmaceutical poisoning in urban centres. As a final-year MBBS student rotating through general medicine and emergency medicine, you will encounter poisoning cases directly. The NMC competencies IM22.1 and IM22.5 require you to describe initial stabilisation and identify toxidromes at the KH level — meaning you must apply this knowledge to a real clinical encounter, make decisions under uncertainty, and provide a rational initial management plan without waiting for specialist input.
RECALL
Activate your prior knowledge before proceeding. Recall the ABC framework of resuscitation: Airway — is it patent? Is there a gag reflex? Breathing — rate, depth, oxygen saturation. Circulation — pulse, blood pressure, perfusion. From pharmacology, recall the autonomic nervous system: the parasympathetic system acts through muscarinic receptors (acetylcholine ligand; effects include miosis, bradycardia, bronchospasm, increased secretions) and nicotinic receptors (at neuromuscular junctions; effects include muscle fasciculations and paralysis). The sympathetic system uses adrenergic receptors (alpha: vasoconstriction, mydriasis; beta: tachycardia, bronchodilation, sweating). From your pharmacology module, recall that opioids act on μ, κ, and δ receptors predominantly in the CNS and gut, and that naloxone is a competitive antagonist at opioid receptors. Understanding which receptor system is activated or blocked by a toxin is the entire basis of toxidrome recognition.
Initial Approach to Stabilisation of the Poisoned Patient
The initial approach to the poisoned patient is governed by two simultaneous imperatives: resuscitation and identification. Unlike most medical presentations where diagnosis precedes treatment, poisoning forces the clinician to resuscitate first and refine the diagnosis in real time. The primary survey follows the ABC framework and must be completed within the first few minutes of the patient's arrival, before any detailed history or toxidrome assessment.
Airway is assessed first. In poisoning, the airway is threatened by several mechanisms: loss of consciousness with tongue falling back, excessive secretions (cholinergic poisoning), vomiting and aspiration (especially opioid or sedative overdose), and direct corrosive injury to the oropharynx. The gag reflex must be assessed immediately. If absent, the airway is unprotected and endotracheal intubation is required. A lateral head-tilt-chin-lift or jaw thrust, followed by a Guedel airway (oropharyngeal airway), can temporise while preparing for intubation. In opioid overdose, administration of naloxone 0.4–2 mg IV/IM/intranasal may rapidly restore protective airway reflexes.
Breathing assessment includes respiratory rate, tidal volume, and oxygen saturation. Apply high-flow oxygen via a non-rebreather mask at 10–15 L/min in all obtunded or hypoxic patients. Specific breathing patterns are diagnostically useful: central respiratory depression (slow, shallow breathing) is seen in opioid, benzodiazepine, and barbiturate poisoning; hyperventilation occurs with salicylate toxicity (direct stimulation of the respiratory centre) and in toxic alcohol poisoning (as a compensatory response to metabolic acidosis); bronchospasm and wheeze are classic features of cholinergic (organophosphate) poisoning. Pulse oximetry is essential but its limitation must be recognised: it does not detect carboxyhaemoglobin (normal SpO₂ reading in carbon monoxide poisoning) — a co-oximeter is needed in suspected CO poisoning.
Circulation assessment: measure pulse rate, blood pressure, and capillary refill time. Establish large-bore IV access (two lines in severe poisoning) and draw blood simultaneously for investigations. Administer 0.9% normal saline as an initial fluid bolus (500 mL–1 L) for hypotension while the cause is being established. The specific haemodynamic pattern is diagnostically important: bradycardia + hypotension + bronchospasm + excessive secretions points to cholinergic toxidrome (organophosphate); tachycardia + hypertension + hyperthermia points to sympathomimetic toxidrome; bradycardia + hypotension without excessive secretions may indicate beta-blocker or calcium channel blocker poisoning requiring specific antidotes (glucagon for beta-blockers; calcium + high-dose insulin for CCBs).
Disability (neurological assessment): Determine the Glasgow Coma Scale (GCS) score immediately. A GCS ≤ 8 or inability to protect the airway mandates intubation. Assess pupils — the pupillary response is the single most diagnostically informative finding at the bedside in an unconscious patient (see toxidrome section). Blood glucose must be checked by bedside glucometer in every unconscious patient — hypoglycaemia can mimic any poisoning and must be corrected immediately with 50 mL of 50% dextrose IV.
Exposure and environment: Remove all clothing to look for skin contamination (especially important in organophosphate, corrosive, and dermal absorption poisonings), rashes, injection sites, and any transdermal patches (remove all patches immediately). Monitor core temperature — hyperthermia is a feature of sympathomimetic and serotonin syndrome; hypothermia occurs with opioid, barbiturate, and alcohol intoxication.
After the primary survey, obtain a targeted history from the patient, family, or paramedics using the SLUDGE mnemonic context: substance involved (name, formulation, amount), time of ingestion, route (oral, dermal, inhalational, intravenous), any emesis or prior treatments given, and the circumstances (suicidal attempt? accidental? occupational exposure?). Bring the container, tablet foil, or agricultural bottle to the ED — the label often confirms the toxin.
ABCDE Management and Toxidrome Recognition in Poisoning
Pathophysiology and Recognition of Toxidromes
A toxidrome (toxic syndrome) is a cluster of clinical signs and symptoms that results from the specific pharmacological mechanism of a class of toxin acting on a defined receptor system. Recognising a toxidrome transforms the seemingly overwhelming complexity of hundreds of possible poisons into five clinical patterns, each pointing to a physiological mechanism and — in many cases — a specific antidote. The concept was formally systematised by Mofenson and Greensher in 1970, but the practice of using symptom clusters to identify poisons is centuries older. In India, where rapid toxicology screening is rarely available at the point of care, the toxidrome approach is the primary diagnostic tool in the emergency department, and proficiency in it is a non-negotiable clinical skill.
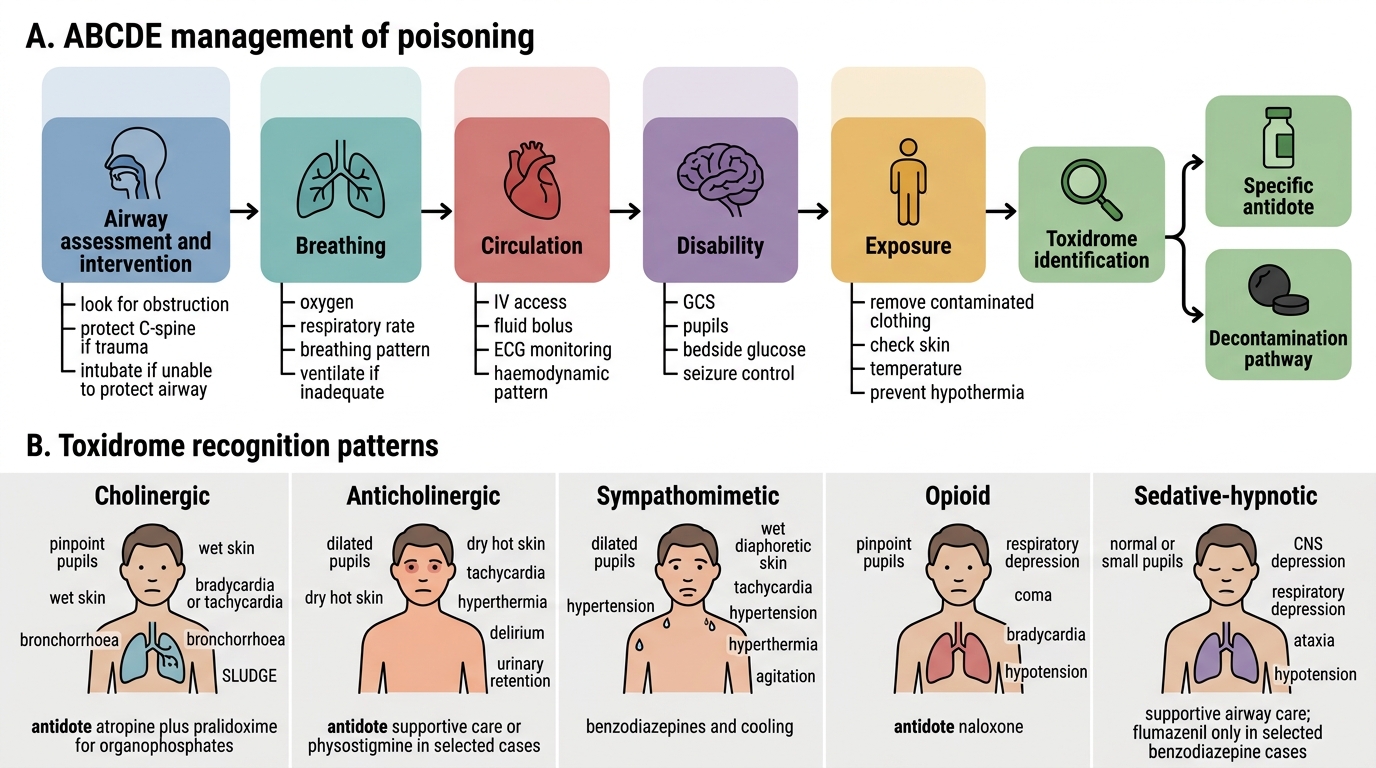
Provided image
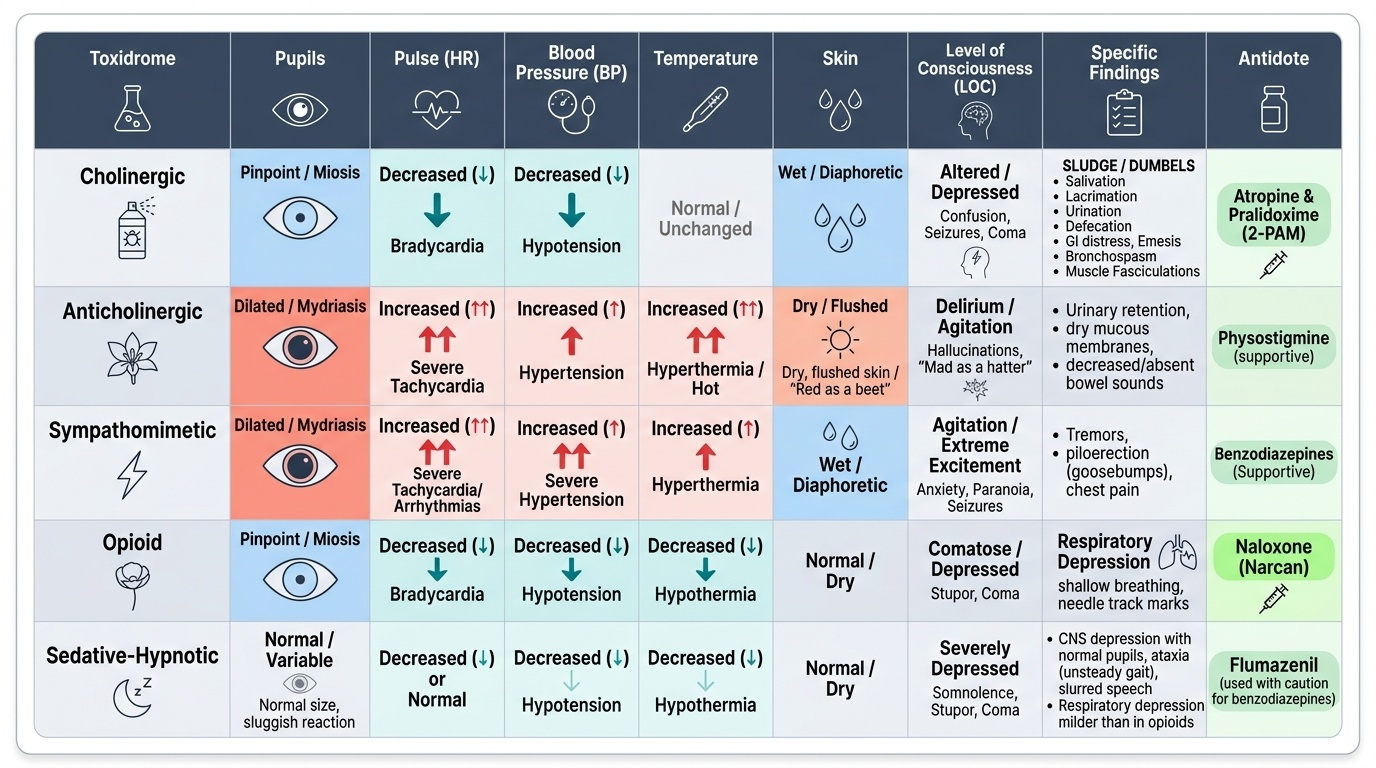
The Cholinergic Toxidrome arises from excess acetylcholine accumulation at muscarinic and nicotinic receptors. This occurs when acetylcholinesterase — the enzyme that normally breaks down acetylcholine — is inhibited. The canonical cause in India is organophosphate and carbamate insecticide poisoning (discussed in detail in the insecticide SDL), but it also occurs with carbamate drugs (physostigmine, neostigmine overdose) and certain mushrooms (Clitocybe, Inocybe species — containing muscarine). The clinical signs are conveniently remembered by two mnemonics: SLUDGE (Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis) captures the excessive exocrine secretions from muscarinic stimulation; DUMBELS (Diarrhoea, Urination, Miosis, Bradycardia, Bronchospasm/Bronchorrhoea, Emesis, Lacrimation, Salivation) is the same set with additional neurological and cardiovascular features. Nicotinic stimulation at neuromuscular junctions causes muscle fasciculations, progressing to weakness and paralysis. Nicotinic stimulation at sympathetic ganglia causes an initial phase of tachycardia and hypertension before the muscarinic bradycardia dominates. Seizures and coma occur with severe cholinergic crisis. The antidote for muscarinic features is atropine (large, repeated doses until secretions dry — see insecticide SDL); nicotinic (neuromuscular) paralysis requires pralidoxime (oxime that reactivates inhibited acetylcholinesterase if given before ageing).
The Anticholinergic Toxidrome is the mirror image of the cholinergic toxidrome — it results from blockade of muscarinic receptors, producing a picture of excess sympathetic tone unopposed by parasympathetic control. Causes include antihistamines (diphenhydramine, chlorphenamine), tricyclic antidepressants (amitriptyline — also has additional cardiac sodium channel effects), antiparkinsonian drugs (benzhexol/trihexyphenidyl, a common abuse agent in India), antispasmodics (atropine, hyoscine), and plants containing atropine and scopolamine (Datura stramonium — commonly called Datura or Dhatura, responsible for significant poisoning burden in India). The classic presentation is summarised as: hot as a hare, blind as a bat, dry as a bone, red as a beet, and mad as a hatter — hyperthermia (impaired sweating), mydriasis (dilated pupils), dry flushed skin and dry mouth, and delirium/agitation/hallucinations. Unlike the cholinergic toxidrome, secretions are absent (dry), which is the key distinguishing feature. Urinary retention is common. The ECG shows tachycardia; in TCA poisoning, QRS widening and QTc prolongation indicate sodium channel blockade. Physostigmine (a reversible anticholinesterase) can reverse anticholinergic features but is rarely used in India due to its own toxicity risk; supportive care and benzodiazepines for agitation are the mainstay.
The Sympathomimetic Toxidrome results from excessive catecholamine stimulation — either excess release (cocaine, amphetamines, MDMA) or reuptake inhibition (cocaine, amphetamines). Clinical features: tachycardia, hypertension, hyperthermia (three cardinal signs), mydriasis (distinguish from anticholinergic: sympathomimetic patients are diaphoretic — wet — while anticholinergic patients are dry), agitation, tremor, and in severe cases seizures and cardiac dysrhythmias. Cocaine also causes coronary artery vasospasm and can precipitate acute myocardial infarction in young patients. Treatment is primarily supportive: benzodiazepines for agitation and seizures, aggressive cooling for hyperthermia, vasodilators (phentolamine) or nitrates for hypertensive emergencies. Beta-blockers should be avoided in cocaine toxicity as unopposed alpha-stimulation can worsen hypertension.
The Opioid Toxidrome results from stimulation of μ, κ, and δ opioid receptors. The classic triad of opioid toxidrome is: (1) miosis (pinpoint pupils) — preserved even in deep coma; (2) respiratory depression — the most dangerous and life-threatening feature; and (3) decreased level of consciousness — from drowsiness to coma. Additional features include bradycardia, hypotension, decreased bowel sounds, and urinary retention. Causes in India include tramadol (increasingly common overdose), pentazocine, codeine-containing cough syrups, and illicitly obtained morphine or heroin. The antidote is naloxone (a pure opioid antagonist): IV dose 0.4–2 mg, repeated every 2–3 minutes up to a total of 10 mg; titrate to restore adequate ventilation (not full alertness — abrupt reversal in opioid-dependent patients causes acute withdrawal). The half-life of naloxone (60–90 min) is shorter than most opioids, so repeat dosing or an infusion may be required.
The Sedative-Hypnotic Toxidrome results from enhancement of GABA-mediated inhibitory neurotransmission (benzodiazepines, barbiturates, alcohol) or from NMDA receptor antagonism (ketamine). Features: CNS depression (sedation → coma), normal or slightly constricted pupils (distinguish from opioid: pupils are NOT pinpoint in uncomplicated benzodiazepine overdose), respiratory depression (though less severe than opioids in BZD alone), hypotension, hypothermia, and ataxia. There is no muscle fasciculation (distinguishes from cholinergic). Benzodiazepine-specific antidote: flumazenil (0.2 mg IV, repeat to 1 mg); use with caution in patients with chronic BZD use (precipitates acute withdrawal and seizures) and when BZD were co-ingested for seizure control. Barbiturate toxicity has no specific antidote; supportive care and urine alkalinisation (for phenobarbital elimination) are the mainstay.
A critically important clinical point: mixed poisoning is common, particularly in deliberate self-harm, where patients may take several substances simultaneously. A pure textbook toxidrome is less common than an overlapping clinical picture. Always consider mixed ingestion when the clinical picture does not fit neatly into one toxidrome.
SELF-CHECK
A 30-year-old man is brought in unconscious. Pulse 44 bpm, BP 70/40 mmHg, pupils 1 mm and fixed, profuse salivation, audible bronchial secretions, muscle fasciculations in both arms, and urinary incontinence. Which antidote combination is immediately indicated?
A. Naloxone + N-acetylcysteine
B. Flumazenil + sodium bicarbonate
C. Atropine + pralidoxime
D. Physostigmine + diazepam
Reveal Answer
Answer: C. Atropine + pralidoxime
This is a classic cholinergic toxidrome — miosis, bradycardia, hypotension, SLUDGE features (salivation, bronchorrhoea, incontinence), and nicotinic signs (muscle fasciculations). The cause is organophosphate or carbamate poisoning (acetylcholinesterase inhibition). The correct antidote combination is atropine (large repeated doses to dry secretions — targets muscarinic receptor blockade) plus pralidoxime (reactivates inhibited cholinesterase at nicotinic NMJ — targets muscle paralysis). Naloxone is for opioid toxidrome (miosis with respiratory depression, no secretions). Flumazenil is for benzodiazepine toxidrome. Physostigmine is the antidote for anticholinergic toxidrome — the opposite of what is needed here.
Essential Investigations in Acute Poisoning
Investigations in acute poisoning serve three purposes: confirm the diagnosis, assess severity and organ damage, and guide specific interventions. They are ordered rapidly and in parallel with resuscitation. While toxicology screens are occasionally available, the majority of Indian emergency departments rely on clinical diagnosis supplemented by routine biochemistry; the ability to interpret these results in the context of the toxidrome is therefore a critical skill.
Blood glucose (bedside glucometer) is the single most important immediate investigation — must be done in every obtunded or unconscious patient within the first minute of assessment. Hypoglycaemia must be treated before attributing impaired consciousness to any other cause.
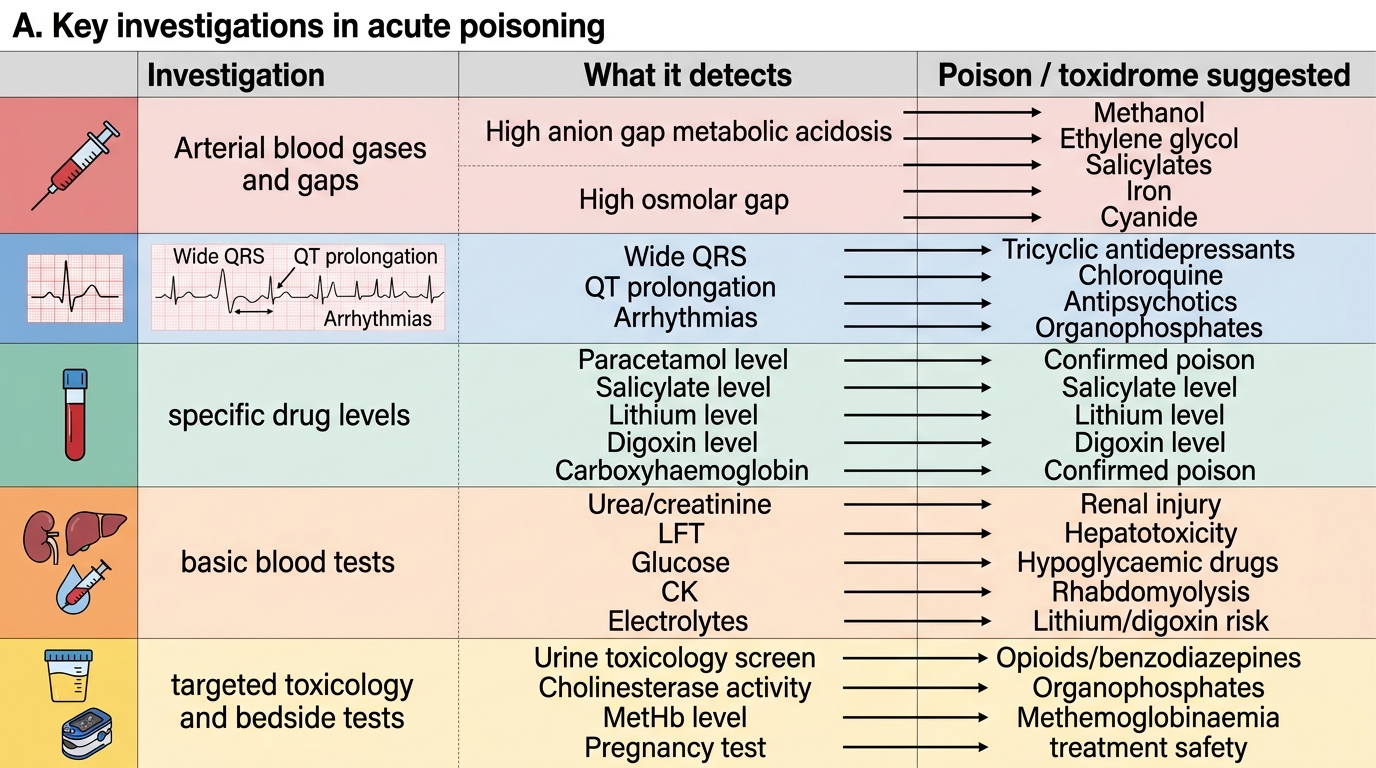
Arterial blood gas (ABG) is the most informative single investigation in acute poisoning. Key parameters: pH (acidosis or alkalosis?), PaCO₂ (respiratory pattern), PaO₂ (oxygenation), bicarbonate (metabolic component), and lactate (tissue perfusion and metabolic poison). The anion gap = Na+ minus (Cl- + HCO3-); normal 8-12 mEq/L. A high anion gap metabolic acidosis (HAGMA) is produced by toxic alcohols (methanol, ethylene glycol), salicylates, and cyanide. Calculate the osmolar gap = measured osmolality minus calculated osmolality (2xNa + glucose/18 + BUN/2.8); an osmolar gap greater than 10 mOsm/kg is strongly suggestive of toxic alcohol ingestion.
Serum electrolytes (Na, K, Cl, bicarbonate), renal function (creatinine, urea): essential for all poisoning cases. Hyperkalaemia can occur in severe acidosis (digitalis, fluoride poisoning). Acute kidney injury occurs with ethylene glycol (oxalate crystalluria), NSAIDs, and heavy metal poisoning.
Liver function tests (LFTs): Elevated transaminases indicate hepatotoxicity. Paracetamol is the classic hepatotoxin; LFT and INR should be checked at 4 and 24 hours after paracetamol ingestion and plotted against the Rumack-Matthew nomogram.
12-lead ECG: Must be done in all cases — prolonged QTc (tricyclic antidepressants, antimalarials, antipsychotics, organophosphates), QRS widening (TCAs), bradycardia and heart block (beta-blockers, digoxin, CCBs), and tachyarrhythmias are all diagnostically useful. The ECG can be diagnostic before any blood result is available.
Full blood count: Anaemia, thrombocytopaenia (lead, benzene, anticoagulants), and leukocytosis (aspiration, systemic inflammatory response).
Urine: Dipstick for blood (haemoglobinuria/myoglobinuria in severe poisoning), protein (renal injury). Specific gravity and urine output are monitored hourly in severe cases. Urine toxicology screen (where available): qualitative detection of opioids, benzodiazepines, amphetamines, cannabis, cocaine.
Specific levels where available and actionable: paracetamol serum level at 4 hours post-ingestion (plot on Rumack-Matthew nomogram to determine NAC need); salicylate level; digoxin level; methanol/ethanol level; carboxyhaemoglobin (co-oximetry in CO poisoning); serum cholinesterase (RBC and plasma) in organophosphate poisoning.
Key Investigations in Acute Poisoning