Page 16 of 27
IM22.8 | Toxic Alcohol Poisoning — SDL Guide
Learning Objectives
- Describe the toxicology and mechanism of toxicity of methanol and ethylene glycol
- Enumerate the clinical features, investigations, and metabolic disturbances of methanol and ethylene glycol poisoning
- Apply the osmolar gap and anion gap to the diagnosis of toxic alcohol poisoning
- Describe the role of alcohol dehydrogenase inhibition (fomepizole or ethanol) as the primary antidote strategy
- Explain the indications for haemodialysis in methanol and ethylene glycol poisoning
INSTRUCTIONS
Methanol and ethylene glycol poisoning are medical emergencies that require early recognition, metabolic investigation, and specific antidote therapy to prevent irreversible organ damage. In India, methanol poisoning from illicit hooch (illegally distilled alcohol) occurs in outbreaks, and ethylene glycol is found in vehicle antifreeze. This module covers the toxicology, clinical recognition, and specific management of both agents.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 454 — Poisoning and Drug Overdose (textbook)
- API Textbook of Medicine, 10th ed., Ch. 26 — Poisoning (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 9 — Poisoning (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
On a Monday morning, your emergency department receives five patients from the same village within two hours. All five attended the same weekend celebration and drank locally produced alcohol. All five now present with varying degrees of confusion, vomiting, and visual disturbance — some complaining of blurred vision, one saying everything looks foggy, one who has already lost vision in both eyes. Their blood sugar is normal. A sixth patient from the same gathering is being brought in by ambulance — this one is unconscious. The pattern is unmistakable once you know what to look for: a methanol poisoning outbreak from illicit hooch. The lethal dose of methanol is approximately 1 mL/kg — a small quantity that produces no immediate intoxication (unlike ethanol), allowing the drinker to consume a potentially fatal amount before symptoms develop. By the time the blindness begins, formic acid has already been accumulating in the optic nerves and retina for hours. Your next decisions — how to confirm the diagnosis without a methanol level (which your lab cannot run), how to give the antidote with the tools available at your hospital, and who needs haemodialysis — will determine who keeps their vision and who survives.
WHY THIS MATTERS
Toxic alcohol poisoning is a recurring public health emergency in India. Methanol poisoning outbreaks from illicit hooch (illegally distilled alcohol contaminated with methanol) cause mass casualty events with dozens to hundreds of affected individuals, as documented in outbreaks in Gujarat (2009 — 136 deaths), Bihar (multiple events), Assam, Andhra Pradesh, and other states. The clinical pattern — apparent intoxication followed by visual disturbance hours later — is distinct and recognisable. Ethylene glycol poisoning from antifreeze ingestion is less common but occurs both accidentally and as a suicide method. NMC competency IM22.8 requires KH-level knowledge of the clinical features, metabolic disturbances, and management of both methanol and ethylene glycol poisoning. Understanding the metabolic investigation (osmolar gap, anion gap) and the specific antidote logic (fomepizole/ethanol as ADH inhibitors) is essential for any physician practising in India.
RECALL
From your biochemistry studies, recall alcohol metabolism: ethanol is oxidised by alcohol dehydrogenase (ADH) to acetaldehyde, then by aldehyde dehydrogenase to acetate. Methanol is also a substrate for ADH, but is oxidised to formaldehyde, then to formic acid (formate) — the toxic metabolite responsible for optic nerve damage and metabolic acidosis. Ethylene glycol is oxidised by ADH to glycolaldehyde, then to glycolic acid, and finally to oxalic acid — the metabolite responsible for renal tubular precipitation and nephrotoxicity. Recall the osmolar gap concept: measured serum osmolality minus calculated osmolality (2×Na + glucose/18 + BUN/2.8); an osmolar gap > 10 mOsm/kg indicates an unmeasured osmole in the serum — methanol, ethylene glycol, and ethanol all elevate the osmolar gap because they are small, osmotically active molecules. The anion gap (Na − [Cl + HCO₃]) measures unmeasured anions; formate and glycolate/oxalate accumulation raises the anion gap in toxic alcohol toxicity.
Clinical Presentation of Methanol and Ethylene Glycol Poisoning
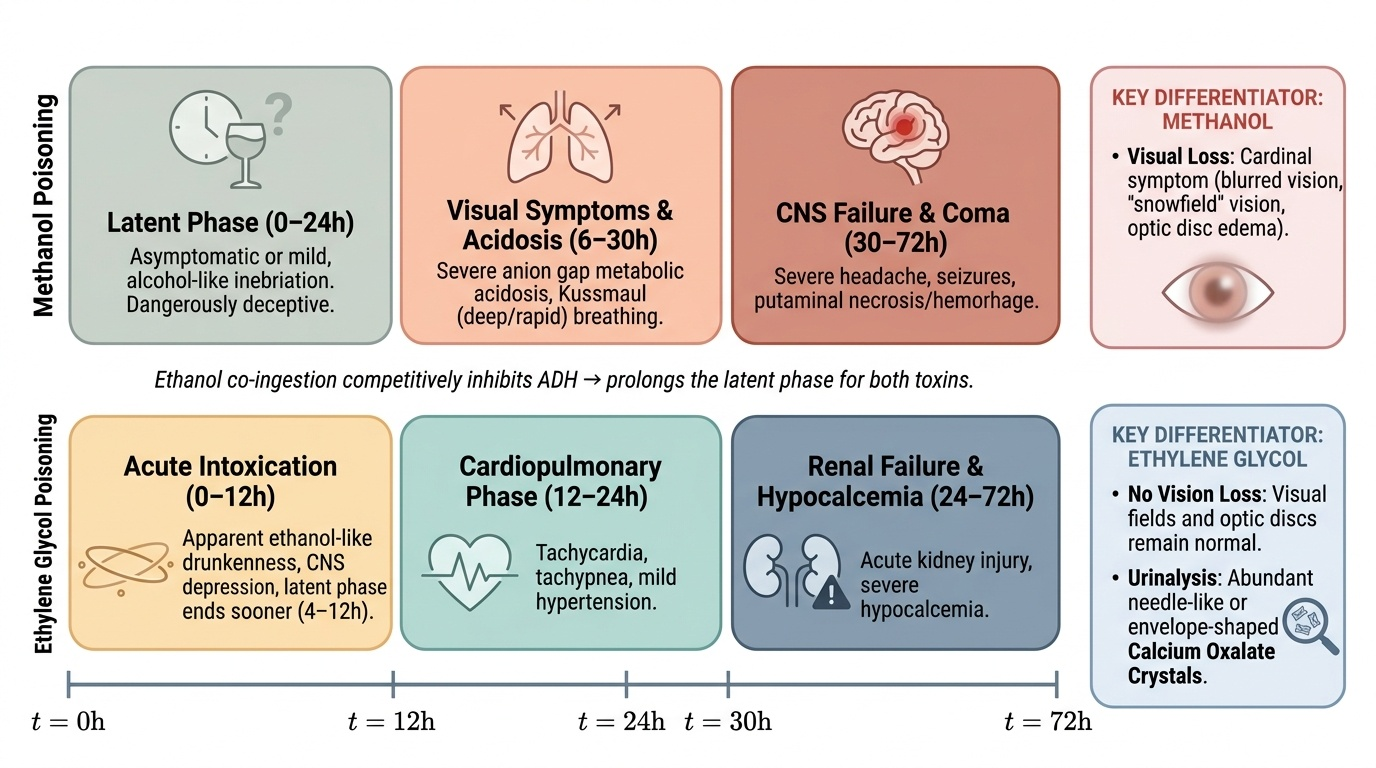
Methanol and ethylene glycol poisoning share a characteristic clinical pattern: an initial period of apparent intoxication (or minimal symptoms) followed by a delayed phase of severe toxicity as the toxic metabolites accumulate. This latent period — 6 to 24 hours for methanol, 4 to 12 hours for ethylene glycol — is clinically dangerous because the patient or their companions may believe the acute danger has passed, when in reality the most toxic phase is imminent. The latent period is longer when ethanol has been co-ingested, because ethanol competitively inhibits ADH, slowing the conversion of methanol and ethylene glycol to their toxic metabolites — this is both a clue (the person who drank illicit hooch and was also drinking ethanol presents later and less severely) and the basis for the ethanol antidote strategy.
Provided image
Methanol poisoning — clinical phases:
Latent phase (1–24 hours post-ingestion): The patient appears mildly intoxicated or may seem entirely well. This is because methanol itself is less intoxicating than ethanol at equivalent concentrations — it produces mild CNS depression but not the pronounced inebriation of ethanol. The absence of prominent intoxication in a patient who claims to have drunk heavily should raise suspicion for methanol.
Toxic phase (onset 6–30 hours, faster without co-ingested ethanol): As formic acid accumulates:
- Visual disturbance — the cardinal and pathognomonic symptom of methanol toxicity. Patients describe blurred vision, reduced visual acuity, central scotoma, photophobia, or complete loss of vision. Fundoscopy reveals optic disc hyperaemia, papilloedema, and retinal oedema — findings that directly reflect formic acid toxicity to the optic nerve. Visual loss can be permanent even with treatment if there is a significant delay.
- Severe metabolic acidosis — high anion gap metabolic acidosis from formate accumulation. Patients develop rapid, deep breathing (Kussmaul respiration) as a compensatory response to the acidosis.
- CNS features — headache, confusion, and in severe cases, seizures and coma. Putaminal haemorrhage and necrosis (visible on MRI) are a characteristic finding in severe methanol poisoning — a unique feature not seen in ethylene glycol toxicity.
- GI features — nausea, vomiting, and abdominal pain are common.
Ethylene glycol poisoning — clinical phases:
Stage 1 (30 minutes – 12 hours): CNS effects from ethylene glycol itself — intoxication resembling ethanol (ataxia, slurred speech, agitation), but disproportionately drowsy given the degree of apparent intoxication, because ethylene glycol is more sedating than ethanol. Metabolic acidosis and elevated osmolar gap develop early.
Stage 2 (12–24 hours): Cardiopulmonary features — tachycardia, hypertension, and pulmonary oedema from calcium oxalate deposition in myocardial and pulmonary vessels.
Stage 3 (24–72 hours): Renal failure — flank pain (from renal tubular obstruction by oxalate crystals), haematuria, oliguria progressing to anuric acute kidney injury. Hypocalcaemia from oxalate chelating calcium (calcium oxalate precipitation removes ionised Ca²⁺ from circulation); tetany and seizures from hypocalcaemia. Unlike methanol, ethylene glycol does NOT cause visual disturbance — the absence of visual symptoms in an antifreeze ingestion is consistent.
Toxicology and Metabolic Pathophysiology
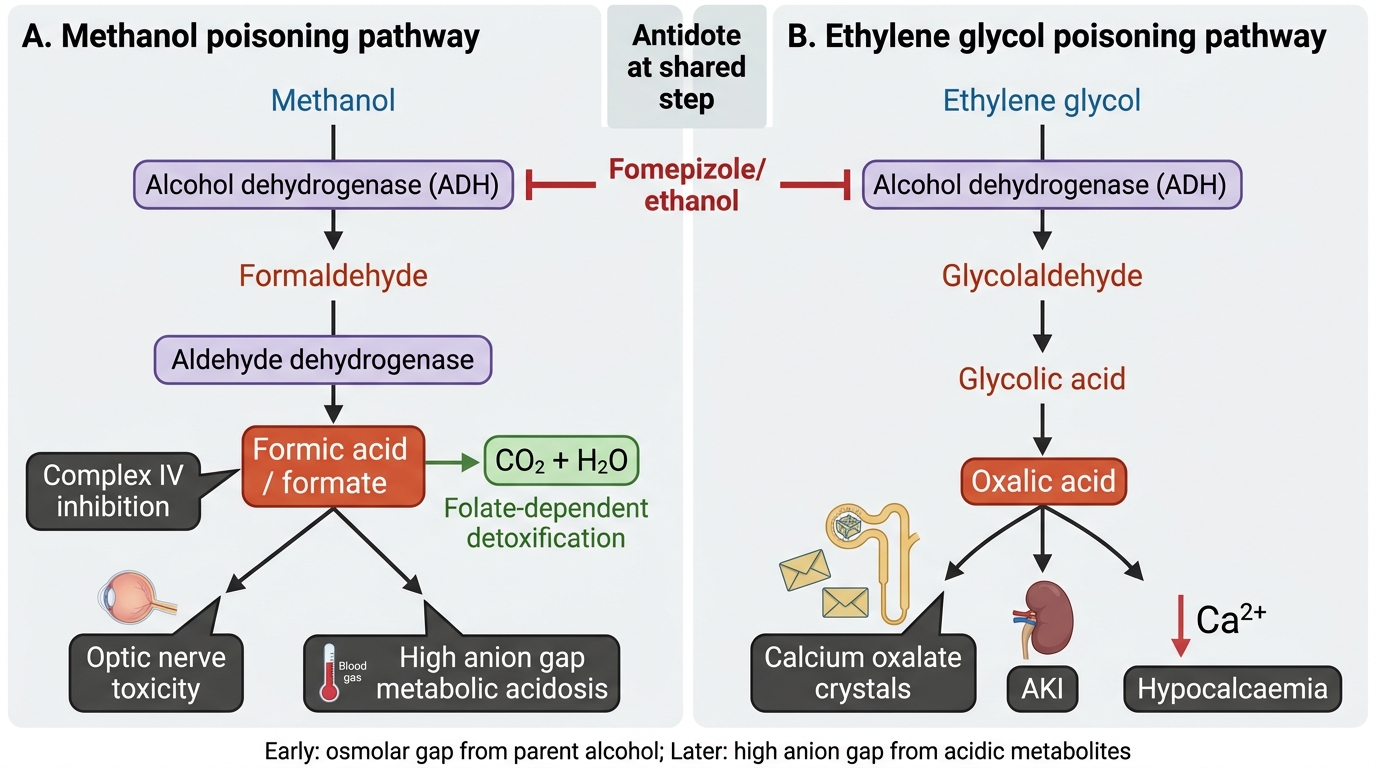
The toxicology of methanol and ethylene glycol poisoning is entirely driven by their metabolic conversion by alcohol dehydrogenase (ADH) to toxic end-products. The parent compounds themselves are relatively non-toxic — it is the metabolites that cause organ damage. This understanding is the direct rationale for the antidote strategy: blocking ADH prevents formation of the toxic metabolites, giving the kidney time to excrete the parent alcohol and haemodialysis time to remove it if needed. Without ADH inhibition, every minute that passes with active metabolism converts more alcohol to the lethal metabolite.
Methanol metabolic pathway:
Methanol → (ADH) → formaldehyde → (aldehyde dehydrogenase) → formic acid (formate). Formic acid is the toxic metabolite responsible for all serious methanol-related pathology. Its mechanism of toxicity is inhibition of cytochrome c oxidase (Complex IV of the ETC) — the same enzyme inhibited by phosphine and cyanide. In the optic nerve and retinal ganglion cells, formate-mediated Complex IV inhibition causes selective metabolic failure and cell death (why the optic nerve is uniquely vulnerable — possibly due to high metabolic demand and limited mitochondrial reserve of these cells). The resulting optic nerve demyelination and retinal oedema produce the characteristic visual toxicity. Formate also accumulates as an anion, driving the high anion gap metabolic acidosis. Folate-dependent metabolism of formate to CO₂ + H₂O is the endogenous detoxification pathway; this is why folate deficiency (prevalent in malnourished populations) worsens methanol toxicity — the body cannot adequately detoxify formate even if methanol metabolism is slowed.
Ethylene glycol metabolic pathway:
Ethylene glycol → (ADH) → glycolaldehyde → (aldehyde dehydrogenase) → glycolic acid → glyoxylic acid → oxalic acid. The key toxic metabolites are glycolic acid (causes metabolic acidosis, renal tubular toxicity) and oxalic acid (precipitates with calcium as calcium oxalate crystals in the renal tubules, causing obstructive nephropathy and AKI). Hypocalcaemia results from calcium oxalate precipitation removing ionised calcium from the circulation — this is a direct cause of tetany and QTc prolongation. On urinalysis, calcium oxalate crystals (both monohydrate and dihydrate forms) in the urine are a characteristic and diagnostically useful finding, though they may not appear until 4–8 hours post-ingestion.
Osmolar gap and anion gap dynamics:
The osmolar gap is elevated EARLY (before significant metabolism has occurred) because the parent alcohols (methanol, ethylene glycol) are osmotically active molecules that increase measured osmolality but are not included in the standard osmolality formula. As ADH metabolises the parent alcohol to ionic metabolites (formate, glycolate, oxalate), the osmolar gap FALLS while the anion gap RISES (the metabolites are charged anions contributing to the anion gap but not measurably affecting osmolality). In very early presentation (< 6 hours), the osmolar gap is elevated but the anion gap may be normal. In late presentation (> 12–24 hours), the anion gap is elevated but the osmolar gap has normalised. Understanding this temporal relationship prevents the diagnostic error of ruling out toxic alcohol poisoning because the osmolar gap is normal at late presentation.
Methanol vs Ethylene Glycol Poisoning Pathways
SELF-CHECK
A 40-year-old man presents 8 hours after drinking illicit hooch. He complains of visual blurring and headache. ABG: pH 7.18, HCO₃ 8 mEq/L. Calculated osmolality 295 mOsm/kg; measured osmolality 302 mOsm/kg (osmolar gap = 7). Serum Na 138, Cl 100, HCO₃ 8 → anion gap = 30 mEq/L. What is the MOST likely diagnosis and how do you interpret the normal osmolar gap with a high anion gap?
A. Ethylene glycol poisoning — the normal osmolar gap excludes methanol; the high anion gap is from glycolate
B. Diabetic ketoacidosis — the high anion gap and acidosis are from ketoacids; osmolar gap is irrelevant
C. Methanol poisoning — at 8 hours, most methanol has been metabolised to formate; the parent alcohol (which causes the osmolar gap) is low while formate (which causes the anion gap) is high
D. Salicylate poisoning — high anion gap metabolic acidosis with visual symptoms from optic nerve toxicity
Reveal Answer
Answer: C. Methanol poisoning — at 8 hours, most methanol has been metabolised to formate; the parent alcohol (which causes the osmolar gap) is low while formate (which causes the anion gap) is high
The temporal relationship between osmolar gap and anion gap is critical in toxic alcohol poisoning. At 8 hours, most of the ingested methanol has been oxidised by ADH to formate. The parent methanol (which elevated the osmolar gap) is mostly metabolised, so the osmolar gap has returned towards normal. The formate (which causes the anion gap acidosis) has accumulated. A normal osmolar gap at 8 hours does NOT exclude methanol — the absence of an elevated osmolar gap in late presentation is expected and predicted by the metabolic pathway. The clinical picture (illicit alcohol, visual blurring, severe metabolic acidosis, high anion gap) is classic methanol poisoning. Ethylene glycol causes renal failure and calcium oxalate crystals, not visual toxicity. Salicylates do not cause visual loss.
Diagnosis: Osmolar Gap, Anion Gap, and Confirming Toxic Alcohol
Diagnosis of toxic alcohol poisoning requires a systematic metabolic investigation because direct measurement of methanol and ethylene glycol levels is not available in most Indian laboratories. The diagnosis is made clinically — based on the history, presenting symptoms, and the characteristic pattern of metabolic abnormalities — using the osmolar gap and anion gap as the primary diagnostic tools. Understanding how to interpret these gaps together, and recognising their temporal relationship, is the core investigative skill for toxic alcohol poisoning.
Step 1: Clinical suspicion. The history and symptoms provide the first diagnostic clue: consumption of illicit or home-distilled alcohol (methanol), or possible antifreeze ingestion (ethylene glycol); visual symptoms (highly specific for methanol); excessive sedation out of proportion to apparent intoxication (ethylene glycol); community outbreak pattern (methanol from contaminated hooch).
Step 2: Serum osmolality and osmolar gap.
Order both measured osmolality (by freezing point depression) and calculated osmolality simultaneously. Calculated osmolality = 2×Na + glucose(mmol/L) + urea(mmol/L) [or glucose/18 + BUN/2.8 in mg/dL units]. Osmolar gap = measured − calculated; normal < 10 mOsm/kg. An elevated osmolar gap (> 10) indicates an unmeasured osmotically active molecule in the serum. In the setting of alcohol ingestion, this strongly suggests toxic alcohol. However, remember: (1) ethanol itself elevates the osmolar gap — if blood ethanol level is available, include it in the calculated osmolality formula (add ethanol/4.6 in mg/dL); (2) the osmolar gap can be elevated by other causes (mannitol, severe hyperglycaemia, isopropanol); (3) a NORMAL osmolar gap at late presentation does NOT exclude toxic alcohol (metabolised parent compound — see pathophysiology).
Step 3: Anion gap and ABG.
Calculate anion gap: Na − (Cl + HCO₃); normal 8–12 mEq/L. Toxic alcohol poisoning causes high anion gap metabolic acidosis from formate (methanol) or glycolate/oxalate (ethylene glycol) accumulation. Serial ABGs assess the progression of acidosis and guide treatment decisions. pH < 7.2 indicates severe poisoning with high metabolite burden.
Step 4: Urinalysis.
In ethylene glycol poisoning: calcium oxalate crystals in urine (monohydrate — envelope shape; dihydrate — dumbbell shape) — appear at 4–8 hours post-ingestion. Haematuria. Fluorescent urine under Wood's lamp (UV light): many commercial antifreeze products contain fluorescein as a leak-detection dye — fluorescent urine is a fast bedside clue to ethylene glycol ingestion (sensitivity ~80%). Absence of fluorescence does not exclude EG (many products do not contain fluorescein).
Step 5: Specific investigations.
Where available (reference lab or academic centre): serum methanol level (toxic > 20 mg/dL; level > 50 mg/dL = severe, mandates haemodialysis), ethylene glycol level (toxic > 20 mg/dL). Serum calcium (hypocalcaemia in EG poisoning). ECG (QTc prolongation from hypocalcaemia and metabolic acidosis). Renal function (AKI in EG). Fundoscopy in methanol: disc hyperaemia, papilloedema, retinal oedema = confirming optic nerve toxicity.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
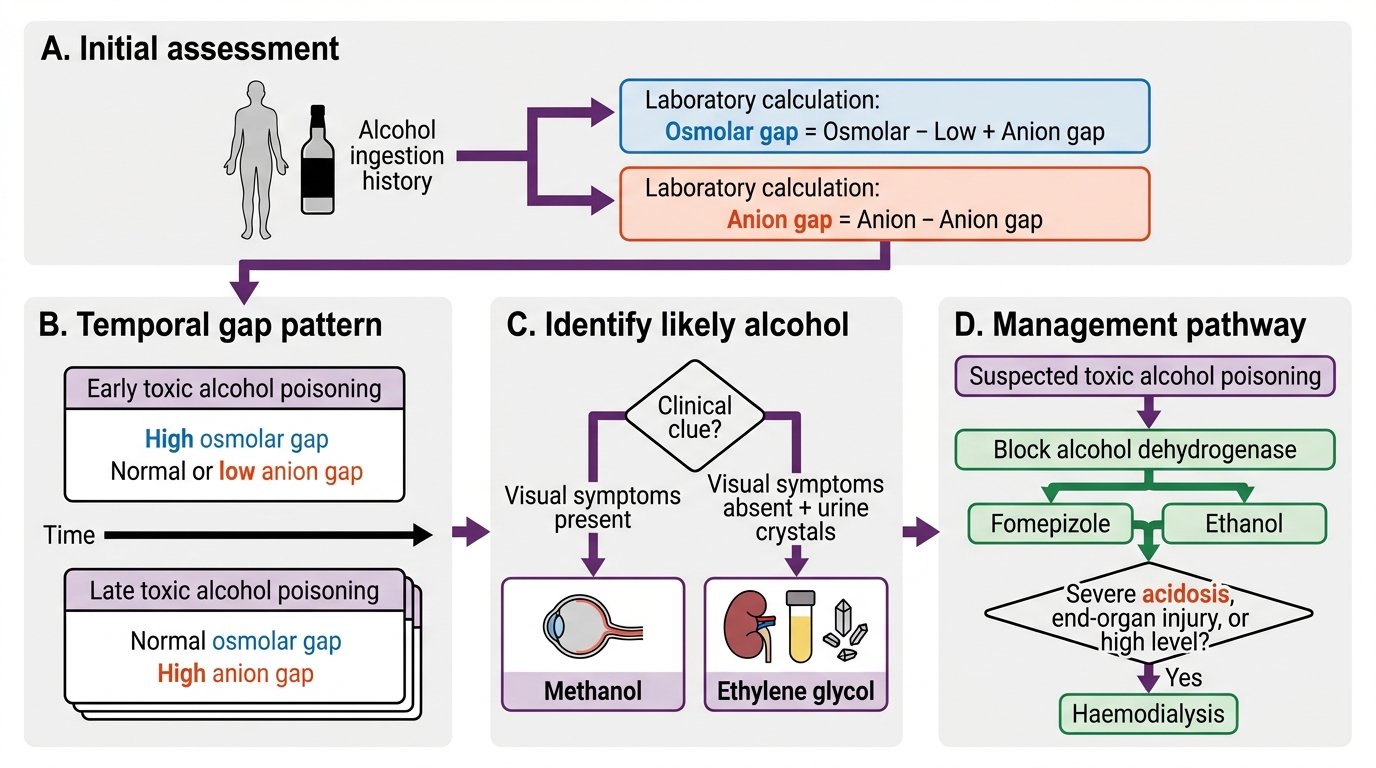
Diagnostic Algorithm for Toxic Alcohol Poisoning