Page 5 of 17
IM23.8-12 | Acid Base Disorders and ABG Interpretation — SDL Guide (Part 2)
Metabolic Alkalosis, Respiratory Acidosis, and Respiratory Alkalosis
The remaining three primary acid-base disorders complete the framework. Each has a characteristic biochemical signature, a pathophysiological mechanism, a set of causes, and — crucially — a compensation that can be calculated to determine whether a mixed disorder is present.
Metabolic alkalosis is characterised by a primary rise in HCO₃⁻ (>26 mmol/L) with pH >7.45. It is generated by one of two mechanisms: loss of H⁺ (from vomit, renal H⁺ excretion, or gastric drainage — removing acid raises plasma HCO₃⁻), or gain of HCO₃⁻ (administration of NaHCO₃, citrate from blood transfusions, or contraction alkalosis — loss of chloride-rich fluid concentrates HCO₃⁻). The key pathophysiological principle is that metabolic alkalosis is maintained (perpetuated) by conditions that prevent the kidney from excreting the excess HCO₃⁻. In a normal kidney, a high HCO₃⁻ would simply spill into urine. However, volume depletion, chloride depletion, and hypokalaemia all force the kidney to retain Na⁺ (and with it HCO₃⁻) at the expense of perpetuating alkalosis. This explains why the treatment of metabolic alkalosis is primarily volume and chloride repletion, not bicarbonate-lowering agents. Causes: vomiting (most common), nasogastric suction, loop and thiazide diuretics (urinary H⁺ and K⁺ losses), primary hyperaldosteronism (aldosterone drives H⁺ secretion in the collecting duct), post-hypercapnia (when chronic CO₂ retention is suddenly corrected by ventilation, the compensatory high HCO₃⁻ remains temporarily — post-hypercapnic alkalosis), milk-alkali syndrome, liquorice excess (glycyrrhizin has mineralocorticoid-like activity). Compensation: PaCO₂ rises by 0.7 × (HCO₃⁻ − 24) mmHg; maximum PaCO₂ compensation is approximately 55–60 mmHg (the hypoxic drive limits further hypoventilation). Clinical features: neuromuscular irritability, paraesthesiae, muscle cramps, tetany (reduced ionised calcium — alkalosis increases albumin binding of calcium). Arrhythmias, especially in the presence of hypokalaemia. Urine Cl⁻ is the key test: chloride-responsive alkalosis (urine Cl <20 mmol/L — kidneys avidly retaining Cl): treat with 0.9% saline and KCl. Chloride-resistant alkalosis (urine Cl >20 mmol/L — primary hyperaldosteronism, severe hypokalaemia, Bartter/Gitelman): treat the underlying cause.
Respiratory acidosis is defined by primary CO₂ retention — PaCO₂ >45 mmHg — causing pH <7.35. It arises from any cause of reduced alveolar ventilation: decreased respiratory drive (CNS depression from opioids, sedatives, general anaesthesia, brainstem lesions), neuromuscular weakness (GBS, myasthenia gravis, ALS, cervical cord injury, phrenic nerve palsy), obstructive lung disease (COPD — the most important clinical cause; asthma in a severe episode), chest wall restriction (kyphoscoliosis, morbid obesity with OHS — obesity hypoventilation syndrome), upper airway obstruction. The HCO₃⁻ rises as compensation: acutely (hours), by 1 mmol/L per 10 mmHg rise in PaCO₂ (intracellular buffering); chronically (days), by 3.5 mmol/L per 10 mmHg (renal HCO₃⁻ retention). This difference between acute and chronic compensation is clinically crucial: a patient with a PaCO₂ of 70 mmHg and HCO₃⁻ of 36 is chronically adapted (a known COPD patient); the same PaCO₂ of 70 with HCO₃⁻ of 26 is acute hypercapnia without renal compensation — a respiratory emergency. Clinical features: headache (CO₂-mediated cerebral vasodilatation), confusion, papilloedema, flapping tremor (CO₂ narcosis at extreme levels), cyanosis (if hypoxaemia is present). Management is directed at the cause: bronchodilators and NIV for COPD, reversal of opioids with naloxone, airway management. Supplemental O₂ must be used cautiously in chronic CO₂ retainers (hypoxic drive mechanism) — titrate to SpO₂ 88–92%.
Respiratory alkalosis is defined by primary hyperventilation — PaCO₂ <35 mmHg — causing pH >7.45. Causes: anxiety/hyperventilation syndrome (most common outpatient cause), hypoxaemia (stimulates peripheral chemoreceptors — altitude, pulmonary embolism, pneumonia, severe anaemia), sepsis (central stimulation of respiratory centre — lactic acidosis initially causes respiratory alkalosis before metabolic acidosis predominates), salicylate poisoning (direct central stimulation — classically causes a mixed respiratory alkalosis + metabolic acidosis), hepatic encephalopathy (progesterone-like compounds stimulate respiration), pregnancy (progesterone-driven hyperventilation — physiological — PaCO₂ falls to approximately 30 mmHg). Mechanical ventilation (iatrogenic overventilation). CNS causes: meningitis, stroke, brain injury. HCO₃⁻ falls in compensation: acutely, by 2 mmol/L per 10 mmHg fall in PaCO₂; chronically, by 5 mmol/L per 10 mmHg. Clinical features: lightheadedness, perioral tingling, carpopedal spasm (reduced ionised calcium, same mechanism as metabolic alkalosis), syncope in severe cases.
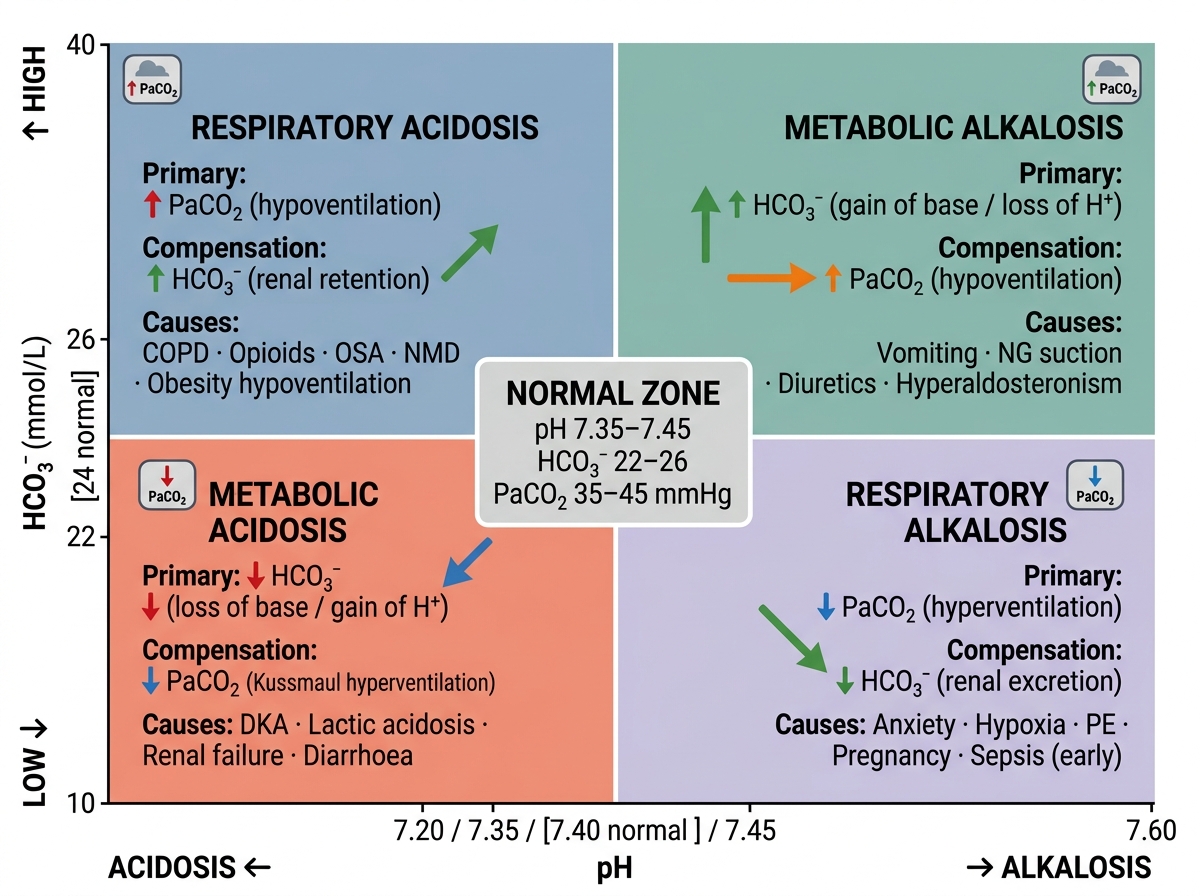
Four Primary Acid-Base Disorders: pH–HCO₃⁻ Axes, PaCO₂, Compensation, and Key Causes
SELF-CHECK
A 45-year-old woman with known COPD presents with worsening breathlessness. ABG: pH 7.30, PaCO₂ 65 mmHg, HCO₃⁻ 31 mmol/L. Her previous baseline ABG (3 months ago) showed pH 7.36, PaCO₂ 58, HCO₃⁻ 32. What is the CORRECT interpretation of her current ABG?
A. Acute respiratory acidosis with appropriate renal compensation
B. Chronic respiratory acidosis — the patient is at a new baseline
C. Acute-on-chronic respiratory acidosis: further CO₂ retention above her baseline
D. Metabolic alkalosis with respiratory compensation
Reveal Answer
Answer: C. Acute-on-chronic respiratory acidosis: further CO₂ retention above her baseline
The patient's baseline already shows chronic CO₂ retention (PaCO₂ 58, HCO₃⁻ 32 — consistent with chronic respiratory acidosis and appropriate renal compensation of 3.5 mmol/L per 10 mmHg rise). Her current PaCO₂ has risen a further 7 mmHg above baseline (65 vs 58). The HCO₃⁻ has not risen further (31 vs 32) — meaning there is no additional renal compensation for the acute increment. This is acute-on-chronic respiratory acidosis: acute CO₂ retention added on top of chronic CO₂ retention. The pH has fallen to 7.30, indicating decompensation. Management: controlled O₂ (target SpO₂ 88–92%), bronchodilators, systemic steroids, non-invasive ventilation (BiPAP).
The Six-Step ABG Interpretation Framework
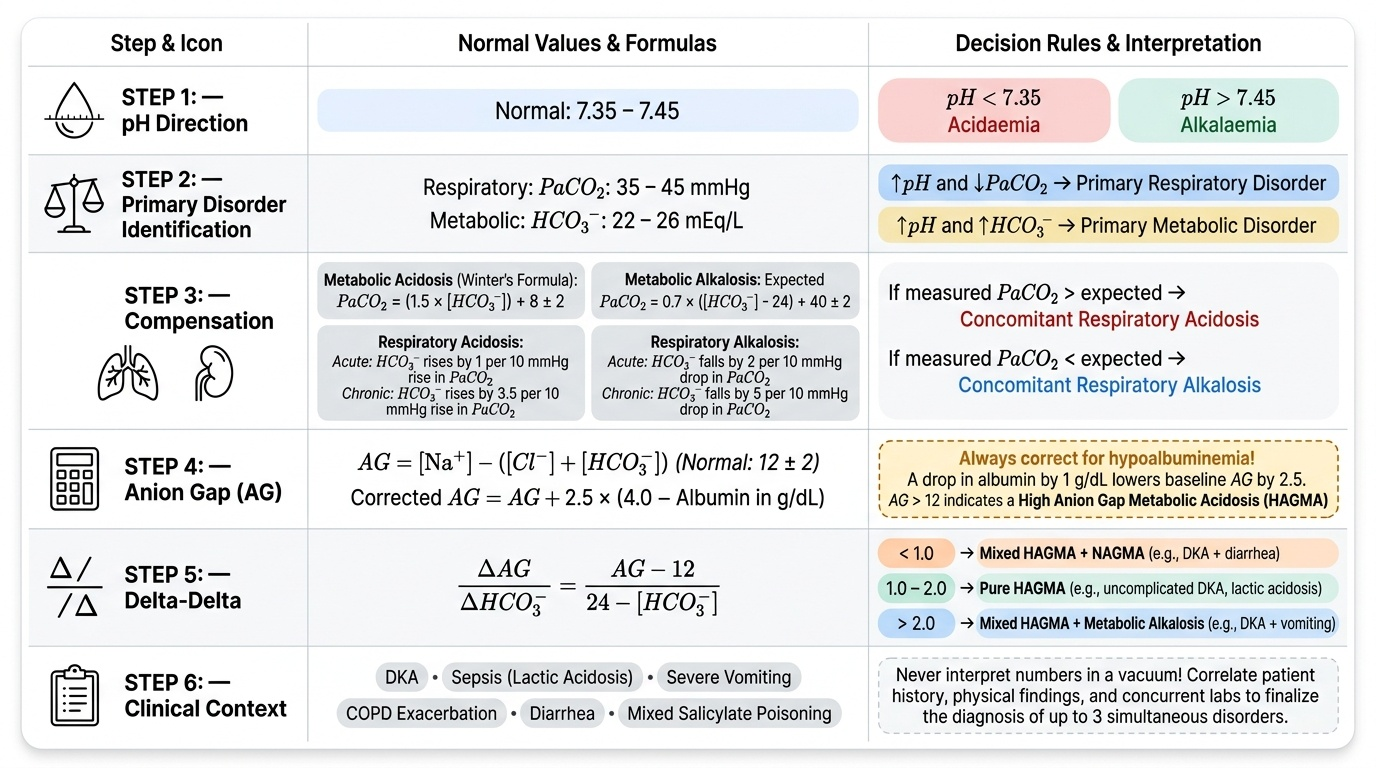
The six-step framework is a systematic approach to arterial blood gas interpretation that identifies the primary disorder, assesses compensation, detects mixed disorders, and applies gap calculations. Applied in order, it takes less than two minutes and cannot miss a standard mixed pattern. The steps are applied to real values from the opening case to demonstrate the method.
ABG from opening case: pH 7.18, PaCO₂ 18 mmHg, HCO₃⁻ 7 mmol/L, Na 138, Cl 98, K 5.2, glucose 42 mmol/L.
The framework proceeds as follows — work through each step before looking at the answer:
Step 1 — Determine the pH: is the patient acidaemic (pH <7.35), alkalaemic (pH >7.45), or normal? Answer: pH 7.18 = severe acidaemia.
Step 2 — Identify the primary disorder: look at PaCO₂ and HCO₃⁻. Which one is abnormal in the direction that explains the pH change? PaCO₂ 18 (low — would cause alkalosis). HCO₃⁻ 7 (low — would cause acidosis). The HCO₃⁻ change explains the pH direction (acidosis), so the primary disorder is metabolic acidosis. The low PaCO₂ is in the 'wrong' direction relative to pH — it is compensatory.
Step 3 — Assess compensation using the appropriate formula: metabolic acidosis → expected PaCO₂ by Winter's formula = 1.5 × HCO₃⁻ + 8 ± 2 = 1.5 × 7 + 8 = 10.5 + 8 = 18.5 ± 2 (i.e., 16.5–20.5). Measured PaCO₂ = 18. This falls within the expected range. Conclusion: single metabolic acidosis with appropriate respiratory compensation. No concurrent respiratory disorder.
Step 4 — Calculate the anion gap: AG = Na − (Cl + HCO₃⁻) = 138 − (98 + 7) = 138 − 105 = 33. This is a markedly elevated anion gap (normal 8–12). Correct for albumin if needed (assume albumin is normal here). The primary disorder is a HIGH anion gap metabolic acidosis. Given the clinical context (glucose 42, DKA likely), the elevated AG is from ketones.
Step 5 — Apply the delta-delta ratio to detect a concurrent metabolic disorder: DDR = (measured AG − 12) / (24 − measured HCO₃⁻) = (33 − 12) / (24 − 7) = 21 / 17 = 1.24. A DDR of 1.0–2.0 indicates pure HAGMA — no concurrent metabolic alkalosis or NAGMA in this case. The bicarbonate fall corresponds closely to the AG rise.
Step 6 — Correlate clinically: the complete picture is severe DKA (glucose 42, HAGMA, AG 33, appropriate respiratory compensation). The peaked T waves on ECG reflect concurrent hyperkalaemia (K 5.2, likely higher intracellularly — DKA causes transcellular K shift). Management: IV insulin infusion, IV fluid resuscitation (0.9% saline initially), potassium monitoring (K will fall rapidly with insulin), and careful monitoring of HCO₃⁻. Bicarbonate is NOT given in DKA unless pH <6.9 — insulin eliminates the ketone-producing process.
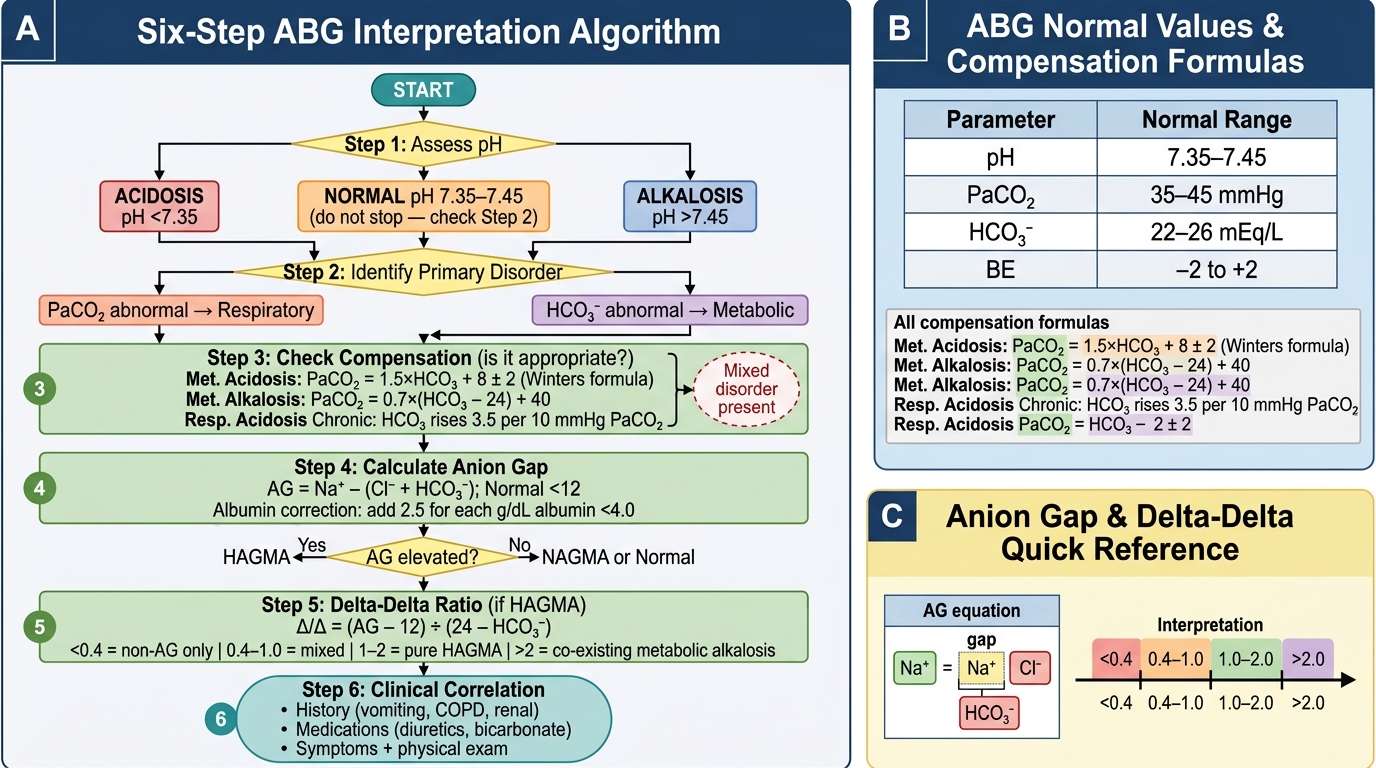
Six-Step Systematic ABG Interpretation Algorithm
SELF-CHECK
ABG: pH 7.38, PaCO₂ 60 mmHg, HCO₃⁻ 34 mmol/L. Serum Na 140, Cl 95, K 4.0. The patient is a 65-year-old man being treated for vomiting from gastric outlet obstruction. What is the CORRECT interpretation?
A. Chronic respiratory acidosis with appropriate metabolic compensation
B. Metabolic alkalosis with appropriate respiratory compensation
C. Mixed metabolic alkalosis and chronic respiratory acidosis
D. Normal ABG — pH is within the normal range
Reveal Answer
Answer: C. Mixed metabolic alkalosis and chronic respiratory acidosis
Step 1: pH 7.38 — normal, but do not stop here. Step 2: Both PaCO₂ (60, high — would cause acidosis) and HCO₃⁻ (34, high — would cause alkalosis) are abnormal in OPPOSITE directions. A normal pH with opposing abnormalities always means a mixed disorder. Step 3: For metabolic alkalosis, expected PaCO₂ = 24 + 0.7 × (34 − 24) = 24 + 7 = 31 mmHg. Measured PaCO₂ = 60 — far above expected. This confirms respiratory acidosis is also present (not just compensation). Step 4: AG = 140 − (95 + 34) = 11 — normal, no HAGMA. Conclusion: mixed metabolic alkalosis (from vomiting/gastric suction) + chronic respiratory acidosis (likely COPD). Each disorder partially masks the pH effect of the other — hence the near-normal pH. The student who sees pH 7.38 and stops has missed both disorders entirely.
SELF-CHECK
In a patient with diabetic ketoacidosis, HCO₃⁻ is 10 mmol/L and Na⁺ is 136, Cl⁻ is 96. Anion gap = 136 − (96 + 10) = 30 mEq/L. The delta-delta ratio = (30 − 12) / (24 − 10) = 18/14 = 1.29. PaCO₂ is 22 mmHg. Using Winter's formula, what is the expected PaCO₂ and what does the measured value indicate?
A. Expected PaCO₂ 23 ± 2; measured 22 mmHg is within range — pure HAGMA with appropriate compensation
B. Expected PaCO₂ 20 ± 2; measured 22 is too high — concurrent respiratory acidosis
C. Expected PaCO₂ 27 ± 2; measured 22 is too low — concurrent respiratory alkalosis
D. Winter's formula does not apply because the anion gap is elevated
Reveal Answer
Answer: A. Expected PaCO₂ 23 ± 2; measured 22 mmHg is within range — pure HAGMA with appropriate compensation
Winter's formula: expected PaCO₂ = 1.5 × HCO₃⁻ + 8 ± 2 = 1.5 × 10 + 8 = 23 ± 2 (i.e., 21–25 mmHg). Measured PaCO₂ = 22, which falls within the expected range. Conclusion: appropriate respiratory compensation — no concurrent respiratory disorder. The DDR of 1.29 also falls within 1.0–2.0, confirming this is a pure high-AG metabolic acidosis without a concurrent NAGMA or metabolic alkalosis. Winter's formula applies to all metabolic acidoses regardless of the AG.
CLINICAL PEARL
Two ABG pearls that save lives in practice:
First: Winter's formula must become automatic for metabolic acidosis. Calculated in seconds, it tells you whether the patient is ventilating appropriately or is also in respiratory failure. A DKA patient with pH 7.20 and HCO₃⁻ 10 should have a PaCO₂ around 23 mmHg. If their PaCO₂ is 38 — 'normal' by the printed reference range — they are in impending respiratory failure: their respiratory muscles cannot sustain the Kussmaul drive that was keeping them alive, and mechanical ventilation may be needed within the hour. Without Winter's formula, this is invisible.
Second: a normal pH does not mean a normal blood gas. In any patient with a clinical reason to suspect acid-base disorder, look at HCO₃⁻ and PaCO₂ independently. If both are abnormal and in opposite directions (one high, one high; one low, one low) — you have a mixed disorder. If both are abnormal in opposite directions with near-normal pH — two disorders are cancelling each other. Treat both, because each one carries its own morbidity.
Self-Assessment: ABG Interpretation Worked Cases
Apply the six-step framework to the following cases before reading the analysis. These represent the most commonly tested clinical scenarios in NMC examinations and in clinical practice. For each case, work through the six steps in sequence — pH direction, primary disorder identification, compensation formula, anion gap, delta-delta if applicable, and clinical correlation — before reading the analysis provided. The purpose of this exercise is not only to arrive at the correct final answer but to build the habit of sequential reasoning that prevents common errors: labelling a pH of 7.38 as 'normal' without examining the PaCO₂ and HCO₃⁻ independently, or missing a concurrent NAGMA in a patient with DKA who also has diarrhoea. Pay particular attention to Winter's formula in every metabolic acidosis case (the most commonly tested compensation formula in the NMC and API exams) and to the delta-delta in cases with a markedly elevated anion gap. These two calculations together — taking under 30 seconds each — convert a basic ABG reading into a complete acid-base analysis that can identify three simultaneous disorders from a single blood sample. The cases below span the full clinical spectrum you will encounter on call: DKA, vomiting, COPD exacerbation, lactic acidosis, and mixed salicylate poisoning.
Provided image
Case 1: Admitted 19-year-old with 3 days of vomiting and coffee-ground haematemesis. pH 7.52, PaCO₂ 48, HCO₃⁻ 38, Na 138, Cl 85, K 2.9.
Analysis: Step 1: pH 7.52 = alkalaemia. Step 2: HCO₃⁻ 38 (high) explains the alkalosis → primary metabolic alkalosis. PaCO₂ 48 (high) is compensatory. Step 3: expected PaCO₂ = 24 + 0.7 × (38−24) = 24 + 9.8 = 33.8 mmHg. Measured 48 — far above expected. Concurrent respiratory acidosis. Step 4: AG = 138 − (85+38) = 15. Mildly elevated; may reflect mild haemoconcentration. Step 5: AG not markedly elevated; delta-delta not critical here. Step 6: Clinical — vomiting → metabolic alkalosis (loss of HCl); haematemesis → likely UGIB causing pain, shallow breathing → concurrent respiratory acidosis; hypokalaemia (K 2.9) perpetuates alkalosis. Management: IV 0.9% saline + KCl; identify and treat the bleeding source.
Case 2: 60-year-old with known COPD, now with drowsiness and cyanosis. pH 7.24, PaCO₂ 78, HCO₃⁻ 32, Na 139, Cl 100, K 4.2.
Analysis: Step 1: pH 7.24 = acidaemia. Step 2: PaCO₂ 78 (high) explains acidosis → primary respiratory acidosis. Step 3: HCO₃⁻ 32. Chronic compensation expected: 24 + 3.5×(78−40)/10 = 24 + 3.5×3.8 = 24 + 13.3 = 37.3. Measured 32 — BELOW expected. This means less renal compensation than expected for a purely chronic disorder → acute-on-chronic respiratory acidosis. Step 4: AG = 139−(100+32) = 7 — normal. No HAGMA. Step 6: Acute decompensated COPD. Management: NIV (BiPAP), controlled O₂ (SpO₂ 88–92%), bronchodilators, systemic steroids, antibiotics if infective exacerbation.
Case 3: 25-year-old runner brought in after collapsing in a marathon. pH 7.22, PaCO₂ 26, HCO₃⁻ 10, Na 141, Cl 103, K 4.1. Lactate 8.2 mmol/L.
Analysis: Step 1: acidaemia. Step 2: HCO₃⁻ 10 → primary metabolic acidosis. Step 3: Winter's: 1.5×10+8 = 23±2 (21–25). Measured PaCO₂ = 26 → slightly above upper expected range. Borderline concurrent respiratory acidosis — suggests respiratory muscles fatiguing. Step 4: AG = 141−(103+10) = 28. High AG. Corrected for normal albumin = 28. Step 5: DDR = (28−12)/(24−10) = 16/14 = 1.14 — pure HAGMA, no concurrent NAGMA. Step 6: High lactate 8.2 confirms lactic acidosis type A (tissue hypoperfusion from exertion and possible rhabdomyolysis). Management: IV fluid resuscitation, rest, monitor renal function, creatine kinase for rhabdomyolysis.