Page 2 of 17
IM23.1-3 | Calcium and Parathyroid Disorders — SDL Guide (Part 2)
Primary Hyperparathyroidism: Clinical Manifestations and Diagnosis
Primary hyperparathyroidism (PHPT) is now predominantly a disease of incidental discovery. In the pre-biochemistry-panel era, patients presented with the classic tetrad of 'bones, stones, groans, and psychic moans' — severe osteitis fibrosa cystica, nephrolithiasis, abdominal symptoms, and psychiatric manifestations. Today, more than 80% of patients are diagnosed at a stage of mild asymptomatic hypercalcaemia found on routine blood testing. The clinical range extends from this silent presentation to rare cases with severe multi-organ involvement.
Epidemiology: PHPT affects approximately 1 in 1000 people, making it the third most common endocrine disorder after diabetes and thyroid disease. It is three times more common in women, with peak incidence in the sixth decade. The vast majority are sporadic; familial forms occur in the context of multiple endocrine neoplasia type 1 (MEN1) (parathyroid hyperplasia/adenoma + pituitary tumour + pancreatic NET), MEN2A (parathyroid hyperplasia + medullary thyroid carcinoma + phaeochromocytoma), and isolated familial hyperparathyroidism.
Clinical manifestations by organ system:
- Bone: persistent hypercalcaemia elevates osteoclast activity, causing bone resorption. In mild disease, only a reduction in bone mineral density (BMD) is seen — particularly at the distal one-third of the radius (cortical bone), which is preferentially affected in PHPT relative to the spine. In severe disease: osteitis fibrosa cystica — subperiosteal bone resorption (radial aspect of middle phalanges), brown tumours (tumour-like collections of fibroblasts and haemosiderin), and bone cysts. Pathological fractures may occur. DEXA scan shows reduced BMD, particularly at cortical sites.
- Kidney: hypercalciuria (calcium >400 mg/24 hours) occurs in up to 40% of PHPT patients. This predisposes to nephrolithiasis (calcium oxalate or calcium phosphate stones — the most common type overall in PHPT). Chronic hypercalcaemia also causes nephrocalcinosis (calcium deposition in renal parenchyma), which can lead to progressive renal impairment. Polyuria and polydipsia result from calcium-induced nephrogenic diabetes insipidus (calcium impairs aquaporin-2 function in the collecting duct).
- Gastrointestinal: constipation (hypercalcaemia reduces smooth muscle contractility), nausea, anorexia, dyspepsia. Peptic ulcer disease (calcium stimulates gastrin secretion). In MEN1, the coexistence of a gastrinoma (Zollinger-Ellison syndrome) amplifies this association.
- Neuromuscular and psychiatric: fatigue, proximal muscle weakness, depression, anxiety, poor concentration, and in severe cases — confusion and coma. The neuropsychiatric manifestations of mild PHPT (especially the 'vague' symptoms of fatigue, foggy thinking, depression) are the most common presenting complaint in the modern era, yet they are frequently attributed to other causes, delaying diagnosis as in the opening case.
- Cardiovascular: mild hypertension is more common in PHPT. Hypercalcaemia shortens the QT interval on ECG (a useful bedside clue).
Diagnosis:
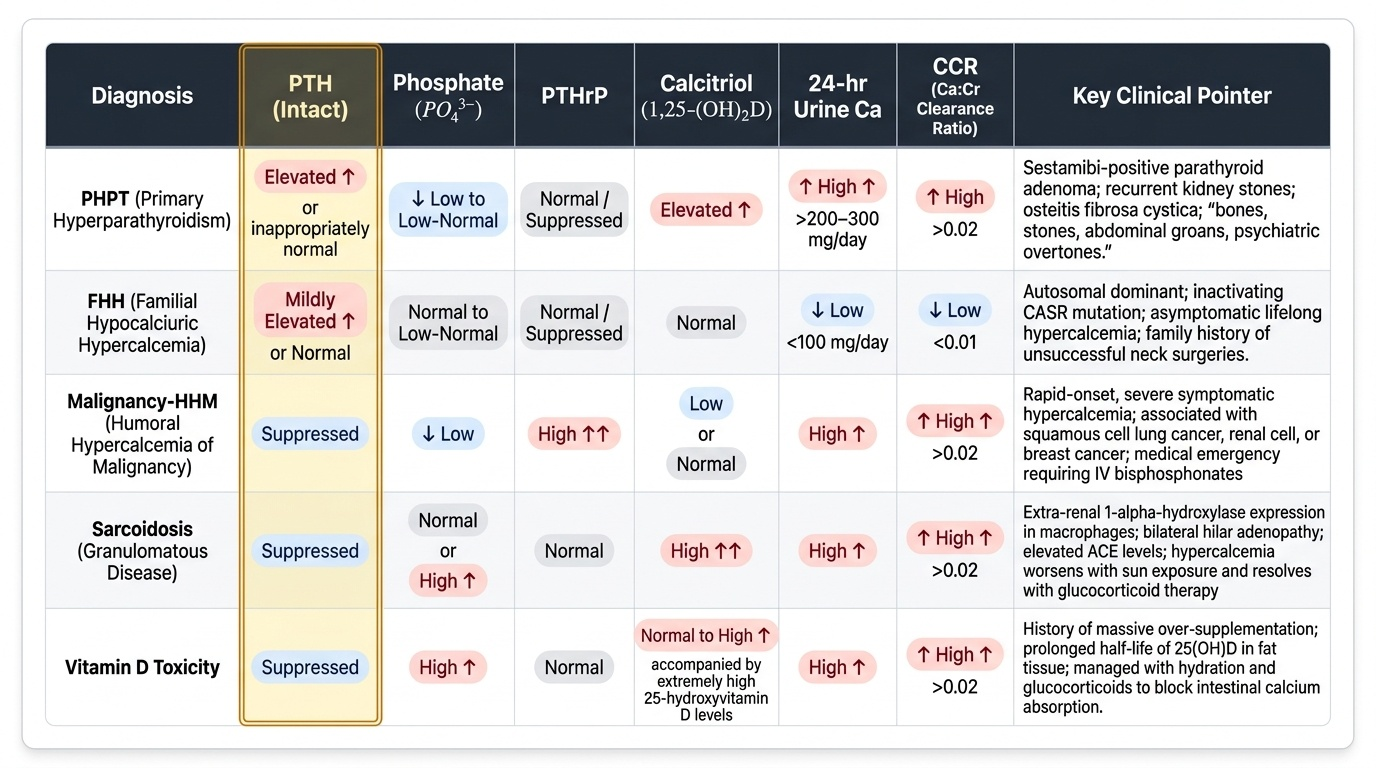
The biochemical diagnosis of PHPT rests on finding simultaneously elevated calcium and elevated (or inappropriately non-suppressed) intact PTH. The steps are:
- Confirm hypercalcaemia on two fasting measurements. Correct for albumin if hypoalbuminaemia is present.
- Measure intact PTH (two-site immunometric assay, normal 10–65 pg/mL). In PHPT: PTH is elevated, or is 'high-normal' despite hypercalcaemia (which is biochemically inappropriate — a normal PTH in the face of hypercalcaemia is never truly normal).
- Measure serum phosphate: low or low-normal (PTH-mediated phosphaturia).
- Measure 24-hour urinary calcium: elevated in PHPT; LOW in FHH (critical differentiation). Calculate calcium-creatinine clearance ratio (CCR) = (urine Ca × plasma Cr) / (plasma Ca × urine Cr); CCR <0.01 = FHH.
- Measure serum calcitriol (1,25-dihydroxyvitamin D): normal or slightly elevated in PHPT.
- Measure serum PTHrP: undetectable in PHPT, elevated in malignancy-HHM.
- Localisation studies (required before surgery, NOT for diagnosis): Tc-99m sestamibi parathyroid scintigraphy (most sensitive for single adenoma; identifies aberrant/ectopic glands); neck ultrasound (identifies location and size, guides intraoperative approach); 4D CT or MRI for complex anatomy or re-operative cases.
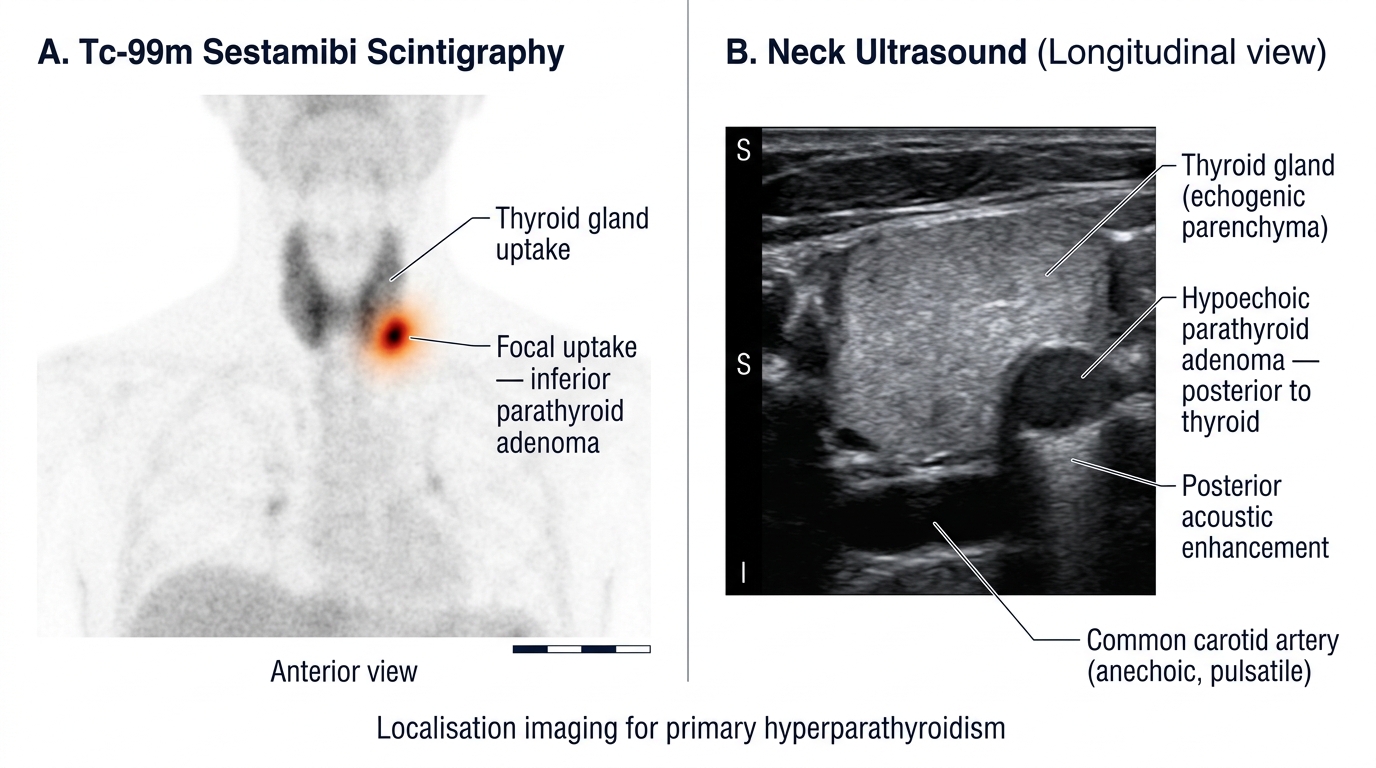
Localisation Imaging in Primary Hyperparathyroidism: Sestamibi Scan vs Neck Ultrasound
Management of Hypercalcaemia and Primary Hyperparathyroidism
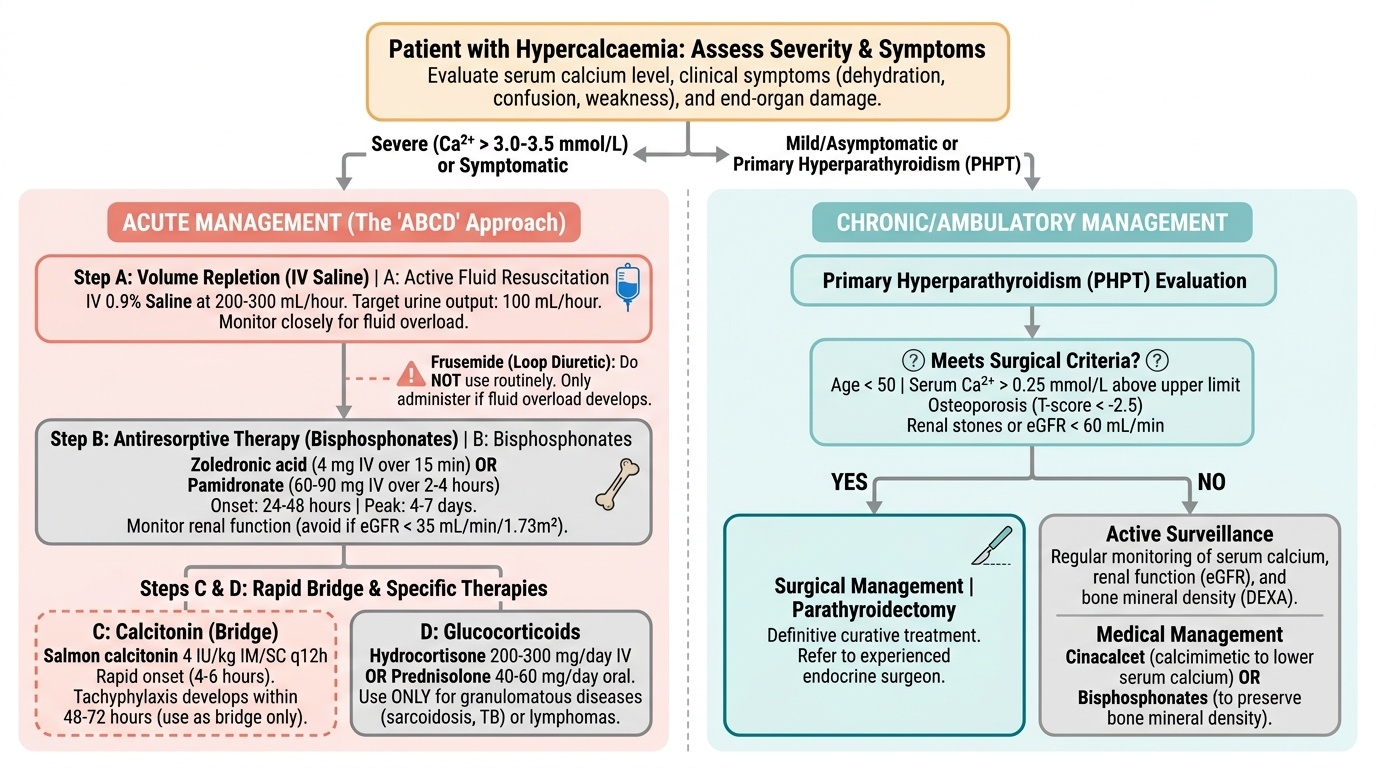
The management of hypercalcaemia depends on the underlying aetiology, the severity of the calcium elevation, and the presence of symptoms or end-organ damage. Two distinct treatment contexts exist: (1) acute management of symptomatic or severe hypercalcaemia (calcium >3.0–3.5 mmol/L or symptoms present), and (2) chronic management of conditions such as primary hyperparathyroidism in the ambulatory setting.
Provided image
Acute management of hypercalcaemia (the ABCD of hypercalcaemia management):
The cornerstone is volume repletion with intravenous 0.9% saline. Hypercalcaemia causes nephrogenic diabetes insipidus, dehydration, and further calcium concentration. Saline administration restores volume, increases glomerular filtration, and promotes calciuresis (calcium follows sodium in the proximal tubule). Typical initial rate: 200–300 mL/hour, targeting urine output of 100–150 mL/hour. Monitor for fluid overload, especially in patients with cardiac or renal compromise. Loop diuretics (frusemide) are NOT administered routinely to 'force calciuresis' — they exacerbate dehydration and hypokalaemia. Frusemide is used ONLY if fluid overload develops.
Bisphosphonates are the second agent for moderate-severe or malignancy-related hypercalcaemia. Zoledronic acid 4 mg IV over 15 minutes (or pamidronate 60–90 mg IV over 2–4 hours) inhibit osteoclast activity, reducing calcium release from bone. Effect is seen in 24–48 hours; maximum effect at 4–7 days. Duration of action: 2–4 weeks (zoledronate) or 1–2 weeks (pamidronate). Monitor renal function before each dose (avoid if eGFR <35 mL/min/1.73m² for standard doses). Adjust dose or choose pamidronate over zoledronate in renal impairment.
Calcitonin (salmon calcitonin 4 IU/kg IM/SC every 12 hours) acts rapidly (within 4–6 hours) by inhibiting osteoclasts and increasing renal calcium excretion, but tachyphylaxis develops within 48–72 hours due to receptor downregulation. Used as a bridge while awaiting bisphosphonate effect. Not appropriate as sole agent.
Glucocorticoids (hydrocortisone 200–300 mg/day IV or prednisolone 40–60 mg/day oral) are specifically effective in granulomatous diseases (sarcoidosis, TB) and some lymphomas because they inhibit macrophage 1α-hydroxylase, reducing calcitriol production. They are NOT effective for PHPT or malignancy-HHM.
Denosumab (RANK-L inhibitor, 60–120 mg SC) is an alternative for bisphosphonate-refractory or renal-failure cases, especially in malignancy-associated hypercalcaemia.
Haemodialysis with low-calcium dialysate is the most rapid and reliable treatment for life-threatening hypercalcaemia (calcium >4 mmol/L with neurological compromise), especially when saline and bisphosphonates are contraindicated (renal failure).
Chronic management — primary hyperparathyroidism:
Surgery (parathyroidectomy) is the only definitive curative treatment for PHPT. The Fourth International Workshop guidelines (2014) recommend surgery for ALL symptomatic PHPT and for asymptomatic PHPT meeting ANY of the following criteria:
| Criterion | Threshold for Surgery |
|---|---|
| Age | <50 years |
| Serum calcium | >1 mg/dL (0.25 mmol/L) above upper normal |
| Bone mineral density | T-score < −2.5 at any site; or previous fragility fracture |
| Renal | eGFR <60 mL/min/1.73m²; or nephrolithiasis on imaging; or 24-hr urine Ca >400 mg/day |
| Vertebral fracture | on imaging (plain X-ray, CT, or VFA on DEXA) |
Minimally invasive parathyroidectomy (MIP) guided by preoperative sestamibi and intraoperative PTH monitoring (rapid PTH assay: >50% fall within 10 minutes of adenoma removal = cure criterion) is now the preferred approach for sporadic single adenoma. Cure rates exceed 95%.
Cinacalcet is a calcimimetic (positive allosteric modulator of the CaSR) that sensitises the CaSR to calcium, lowering PTH secretion and serum calcium. It is used in patients who are not surgical candidates (frailty, comorbidity) or who decline surgery, in tertiary hyperparathyroidism post-transplant, and in parathyroid carcinoma. It does not improve BMD.
Surveillance for asymptomatic PHPT not meeting surgical criteria: annual serum calcium, annual renal function, DEXA every 1–2 years.
SELF-CHECK
A 70-year-old woman with disseminated breast cancer presents with confusion, nausea, and polyuria. Serum calcium is 3.6 mmol/L (14.4 mg/dL). PTH is <5 pg/mL. She is haemodynamically stable. What is the FIRST step in acute management?
A. IV frusemide 80 mg to promote calciuresis
B. Immediate subcutaneous calcitonin 4 IU/kg
C. Intravenous 0.9% saline infusion at 200–300 mL/hour
D. Prednisolone 60 mg oral for anti-inflammatory effect
Reveal Answer
Answer: C. Intravenous 0.9% saline infusion at 200–300 mL/hour
The cornerstone of acute hypercalcaemia management is IV volume repletion with 0.9% normal saline. Hypercalcaemia causes nephrogenic DI and dehydration, concentrating calcium further. Saline restores GFR and promotes calciuresis. Frusemide is NOT a first-line agent (it exacerbates dehydration — only use if fluid overload develops). Calcitonin can be added as a bridge therapy for rapid effect, but saline takes precedence. Prednisolone is for granulomatous diseases; it has no role in malignancy-HHM. After adequate hydration, IV zoledronic acid is added to inhibit osteoclast-mediated calcium release.
SELF-CHECK
Which investigation is MOST important to differentiate primary hyperparathyroidism from familial hypocalciuric hypercalcaemia before recommending parathyroidectomy?
A. Serum PTHrP level
B. Tc-99m sestamibi parathyroid scintigraphy
C. 24-hour urine calcium and calcium-creatinine clearance ratio
D. Serum 25-hydroxyvitamin D
Reveal Answer
Answer: C. 24-hour urine calcium and calcium-creatinine clearance ratio
FHH and PHPT both present with elevated calcium and elevated PTH. The critical distinguishing test is the 24-hour urine calcium and calculation of the calcium-creatinine clearance ratio (CCR). In PHPT, urinary calcium is elevated (>400 mg/24hr) and CCR >0.02. In FHH, renal calcium reabsorption is pathologically increased due to the mutated CaSR, producing low urinary calcium and CCR <0.01. Parathyroidectomy is ineffective in FHH (the glands are normal in their function relative to the shifted set-point) — performing surgery based on PTH alone without excluding FHH is a dangerous error. Sestamibi is a localisation study used only after the biochemical diagnosis is confirmed, not to differentiate FHH from PHPT.
CLINICAL PEARL
The single most powerful bedside rule in hypercalcaemia is: always measure calcium and PTH together, and interpret the PTH relative to the calcium — not as an isolated value. A PTH of 50 pg/mL (within the normal 10–65 range) is NORMAL when calcium is normal, but INAPPROPRIATE when calcium is 3.0 mmol/L. At that level of hypercalcaemia, PTH should be undetectable (<5 pg/mL) because the parathyroids ought to be completely suppressed. A 'normal' PTH in the face of hypercalcaemia means the parathyroids are not responding normally to the calcium signal — this is primary hyperparathyroidism until proven otherwise.
A second pearl: never forget to check the calcium-creatinine clearance ratio (CCR) before sending a patient to a parathyroid surgeon. Familial hypocalciuric hypercalcaemia (FHH) mimics PHPT perfectly on routine biochemistry and will show an adenoma on sestamibi in a proportion of cases because some FHH patients develop a genuine adenoma later in life. The CCR remains the definitive functional test: CCR <0.01 = FHH; parathyroidectomy will fail to normalise calcium and may render the patient permanently hypoparathyroid.
Self-Assessment: Integrating Calcium and Parathyroid Disorders
You have now covered normal calcium homeostasis, the PTH versus non-PTH classification of hypercalcaemia, the clinical features and diagnosis of primary hyperparathyroidism, and the acute and chronic management principles. The scenarios below are designed to test your ability to apply this framework systematically — choosing the right diagnostic path based on the simultaneous interpretation of serum calcium, intact PTH, phosphate, PTHrP, calcitriol, and urinary calcium. The skill being tested is not simple recall but pattern recognition: given a biochemical set, can you identify the mechanism, name the diagnosis, and sequence the management correctly? Work through each scenario before reading the analysis. Note that the same calcium value can arise from completely different mechanisms with different urgencies and treatments — the PTH level is the critical pivot point that distinguishes a benign outpatient condition from a malignancy-driven emergency requiring hospitalisation and IV bisphosphonates within hours.
Provided image
Scenario A: A 45-year-old woman has calcium 2.85 mmol/L on two consecutive fasting samples. Intact PTH is 72 pg/mL. Phosphate is 0.72 mmol/L. 24-hour urinary calcium is 380 mg. CCR is 0.025. Sestamibi scan shows focal uptake in the left inferior neck. She is otherwise well and declines any surgery at present. What is the diagnosis and management approach?
Analysis: PTH-mediated hypercalcaemia (elevated PTH + low phosphate + elevated urinary calcium + CCR >0.02) = PHPT with single adenoma on sestamibi. Since she is asymptomatic, apply the Fourth International Workshop surgical criteria: age 45 (meets the <50 criterion). Therefore, surgery is recommended. However, if she declines, offer surveillance (annual calcium, renal function, DEXA every 1–2 years) and consider cinacalcet for ongoing symptom management.
Scenario B: A 68-year-old man with known small cell lung cancer presents with calcium 3.5 mmol/L. PTH is undetectable at <5 pg/mL. PTHrP is markedly elevated. Phosphate is 0.65 mmol/L. What is the primary mechanism and the most appropriate management sequence?
Analysis: Humoral hypercalcaemia of malignancy (HHM) from PTHrP secretion — typical of small cell carcinoma (though more classic for squamous cell; accept the vignette as stated). Management: IV 0.9% saline volume resuscitation first → IV zoledronic acid 4 mg once rehydrated (check eGFR first) → calcitonin as bridging agent. Glucocorticoids are NOT effective here. Treat the underlying malignancy for long-term control.
Scenario C: A 35-year-old man with known sarcoidosis presents with mild hypercalcaemia (2.75 mmol/L), polyuria, and constipation. PTH is 8 pg/mL (suppressed). Phosphate is normal. Calcitriol is elevated at 190 pmol/L (normal 60–108). Which treatment is most appropriate?
Analysis: Granulomatous hypercalcaemia (sarcoidosis-associated macrophage 1α-hydroxylase → excess calcitriol). Management: oral prednisolone 40 mg/day — glucocorticoids specifically block macrophage 1α-hydroxylase. Advise sun avoidance and avoid high dietary calcium. Bisphosphonates and IV saline are appropriate for severe or symptomatic cases; for this mild presentation, steroid therapy alone is the correct first-line.