Page 7 of 17
IM24.1-5 | Nutrition Assessment and Support — SDL Guide
Learning Objectives
- Describe the methods of nutritional assessment in hospitalised patients including anthropometric, biochemical, clinical, and dietary components
- Discuss the causes and consequences of protein-calorie malnutrition in the hospital setting
- Describe the aetiology, clinical manifestations, complications, diagnosis, and management of common vitamin deficiencies
- Enumerate the indications for enteral and parenteral nutrition in critically ill patients
- Counsel patients on an appropriate balanced diet in a simulated environment
INSTRUCTIONS
Malnutrition is the most under-recognised and undertreated condition in hospitals worldwide. In India, where both under-nutrition and the emerging burden of obesity-related micronutrient deficiency coexist, nutritional medicine is a daily clinical skill. This module builds from the physiology of normal nutrition through the assessment of malnutrition, to specific vitamin deficiencies, and culminates in the clinical decision-making framework for enteral and parenteral nutrition support.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 326–328 — Nutritional Requirements, Nutritional Assessment, and Enteral/Parenteral Nutrition (textbook)
- API Textbook of Medicine, 10th ed. — Nutrition and Nutritional Disorders (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 20 — Nutrition (textbook)
- ESPEN Guidelines on Clinical Nutrition in the ICU, 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old farmer is admitted to the medical ward with a 3-month history of progressive weakness and weight loss. He is thin, with visible temporal wasting, oedematous ankles, and flaky skin. He has had chronic diarrhoea for six months and now cannot walk unassisted. His serum albumin is 2.1 g/dL; haemoglobin is 8.4 g/dL with a mixed picture (macrocytes and microcytes on smear); random blood glucose is normal; HIV test is negative.
His diet history reveals near-total dependence on maize for the past year, with minimal animal protein, fruit, or vegetables.
This patient has at least three simultaneous nutritional deficiencies — protein-calorie malnutrition, pellagra (niacin deficiency from maize-dominant diet), and likely a deficiency of thiamine, folate, and vitamin B12 — but the clinical picture is a tangle of overlapping symptoms. Understanding how to assess nutritional status systematically and recognise specific deficiency syndromes is the only way to untangle it.
WHY THIS MATTERS
Hospital malnutrition is not a problem of resource-poor settings alone — studies across India show that 20–50% of hospitalised patients are malnourished on admission, and a further 10–15% deteriorate nutritionally during their stay. Malnutrition independently increases the risk of infections (impaired immunity), poor wound healing, pressure ulcers, longer hospital stay, higher costs, and mortality. Vitamin deficiencies are highly prevalent in India: vitamin D deficiency is almost universal (>80% in some population studies), vitamin B12 deficiency is common in vegetarians, thiamine deficiency is endemic in populations dependent on polished rice, and iron deficiency is the most common cause of anaemia worldwide. For NMC competencies IM24.1–24.5, you must be able to assess nutritional status, identify specific deficiency syndromes, and make decisions about enteral versus parenteral nutrition in the sick patient.
RECALL
Recall the fundamentals of macronutrient metabolism from biochemistry. The three macronutrients are carbohydrates, proteins, and fats. Carbohydrates provide 4 kcal/g; the minimum intake to prevent gluconeogenesis from protein is approximately 100–150 g/day. Proteins provide 4 kcal/g; the minimum daily requirement is approximately 0.8 g/kg/day in adults (higher in illness, injury, and pregnancy — up to 1.5–2.0 g/kg/day in the critically ill). The essential amino acids (cannot be synthesised by the body) are: isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, valine (and histidine in infants). Fats provide 9 kcal/g; essential fatty acids (linoleic and alpha-linolenic acid) must come from the diet. The total daily energy requirement for a 70 kg adult at rest (basal metabolic rate, BMR) is approximately 1400–1800 kcal/day; this rises by 20–50% in stress states (sepsis, trauma, major surgery). The fat-soluble vitamins (ADEK) require dietary fat for absorption and are stored in the body; the water-soluble vitamins (B-complex and C) are not stored and must be supplied daily. Micronutrients — vitamins and minerals — participate in enzymatic reactions; their deficiency therefore impairs multiple metabolic pathways simultaneously, producing multi-system deficiency syndromes.
Orientation: The Scope and Burden of Malnutrition
Nutrition is foundational to recovery from illness. The physiological stress of acute disease — infection, surgery, trauma, organ failure — triggers a catabolic state driven by cortisol, catecholamines, and pro-inflammatory cytokines. In this state, the body preferentially breaks down muscle protein to provide gluconeogenic substrates, nitrogen balance becomes negative, and micronutrient stores are rapidly depleted. A patient who was borderline malnourished at admission can become severely malnourished within days without adequate nutritional support. This phenomenon — hospital-acquired malnutrition — is preventable but requires active recognition and intervention.
Two distinct nutritional disease burdens coexist in India and must be understood in context. The first is under-nutrition: protein-energy malnutrition (PEM), micronutrient deficiencies (iron, iodine, folate, vitamins A, D, B12), and growth stunting — these remain major public health problems, particularly among the poor, elderly, and chronically ill. The second, rapidly growing burden is over-nutrition with micronutrient deficiency: urban populations with high-calorie but nutritionally poor diets show vitamin D deficiency from sun avoidance, B12 deficiency from vegetarian diets, and zinc deficiency despite adequate caloric intake. Understanding this double burden is essential for taking a nutritional history that covers both dimensions — not simply asking 'how much do you eat' but 'what do you eat and what are you missing.'
The consequences of hospital malnutrition span every organ system. Immune function is impaired — both cell-mediated immunity (T-lymphocyte function, critical for fighting intracellular pathogens like TB and fungi) and humoral immunity (reduced antibody production). Wound healing is delayed — collagen synthesis requires vitamin C, zinc, and protein. Respiratory muscle mass decreases, prolonging ventilator dependency. Gut mucosal integrity deteriorates, increasing bacterial translocation and the risk of septicaemia. Cardiac muscle is not spared — severe PEM causes reduced cardiac output and increased susceptibility to arrhythmias.
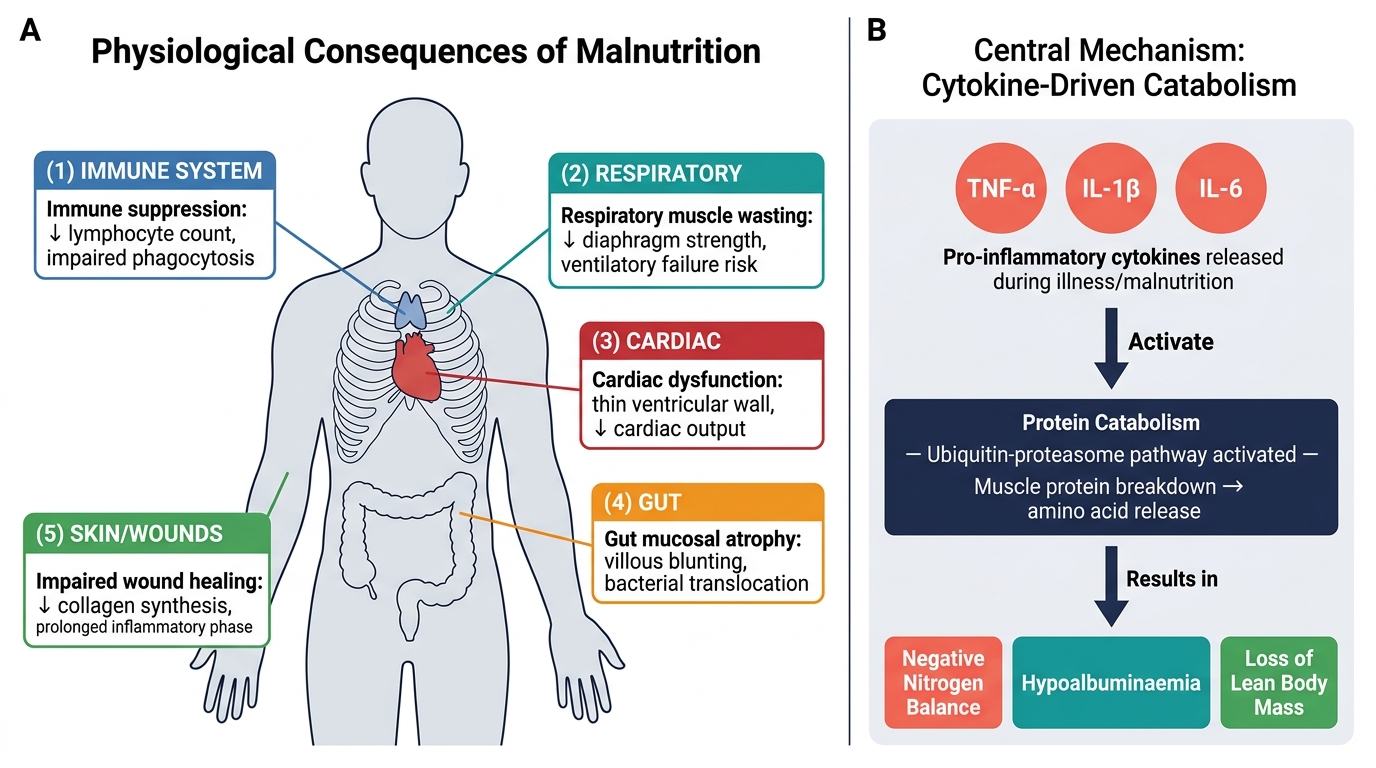
Multi-Organ Consequences of Malnutrition and the Cytokine-Driven Catabolic Mechanism
Nutritional Assessment: ABCD Framework
Nutritional assessment in hospitalised patients uses the ABCD framework: Anthropometric measurements, Biochemical markers, Clinical examination, and Dietary history. No single parameter is sufficient in isolation; the complete picture integrates all four domains. The purpose of assessment is twofold: to identify patients who are already malnourished (and require immediate support) and to identify those at risk of malnutrition during their hospital stay (and require preventive intervention).
A validated screening tool should be used on every hospital admission. The Malnutrition Universal Screening Tool (MUST) is widely validated and uses three parameters: BMI, unintentional weight loss percentage, and acute disease effect (absence of nutrition for >5 days). Scores of 0 = low risk (routine care), 1 = medium risk (monitor), ≥2 = high risk (nutritional support). The Nutritional Risk Screening 2002 (NRS-2002) is preferred in hospitalised patients (validated specifically in the inpatient setting) and adds a disease severity score to the patient's nutritional status score; total score ≥3 indicates nutritional risk and warrants dietitian referral and active support.
The detailed assessment covers each domain:
Anthropometric measurements provide objective physical data that are compared to reference standards. Body mass index (BMI) = weight (kg) / height (m²); graded as: <18.5 = underweight, 18.5–24.9 = normal, 25–29.9 = overweight, ≥30 = obese; ≤16 = severe thinness. Note that BMI does not distinguish fat from muscle mass — a sarcopenic obese patient may have normal BMI with severely depleted muscle. Mid-upper arm circumference (MUAC) is particularly useful in community settings, elderly patients, and when weighing is impractical (oedema, immobility); MUAC <22 cm in adults indicates severe undernutrition. Skinfold thickness (triceps, subscapular, biceps, suprailiac) estimates subcutaneous fat using Harpenden callipers; the sum of four skinfolds correlates with total body fat percentage using Durnin-Womersley equations. Waist circumference and waist-hip ratio assess central adiposity and metabolic risk. Handgrip strength (dynamometry) is a validated marker of muscle function (not just mass) and is independently predictive of clinical outcomes — weak grip in a hospitalised patient predicts complications, longer stay, and mortality independent of BMI.
Biochemical markers reflect specific nutritional deficiencies. Serum albumin (normal 35–50 g/L) — a marker of chronic nutritional status and protein synthesis capacity, but importantly also an acute-phase reactant (falls in inflammation independent of nutrition — thus a poor marker of acute nutritional change). Serum prealbumin (transthyretin) — shorter half-life (2–3 days) than albumin (21 days), making it a more sensitive index of recent nutritional change; normal >20 mg/dL. C-reactive protein (CRP) should be measured alongside prealbumin — if CRP is elevated, the fall in prealbumin reflects inflammation rather than malnutrition. Nitrogen balance = protein intake (g/day) / 6.25 − (urinary urea nitrogen + 4 g insensible losses); positive balance = anabolism; negative balance = catabolism. Transferrin, retinol-binding protein, haemoglobin, iron studies, vitamin levels (B12, folate, 25-OH vitamin D, vitamin B1), zinc, and selenium as indicated by the clinical picture.
Clinical examination signs of specific deficiencies are reviewed in detail in the next section. At the assessment stage, the key elements are: general appearance (temporal wasting, muscle wasting in the thenar eminences and interossei), skin (dermatitis, purpura, poor wound healing), hair (texture, loss), eyes (conjunctival pallor, Bitot spots for vitamin A), mouth (angular stomatitis, glossitis, cheilosis for B-complex), neurology (peripheral neuropathy, ataxia, cognitive impairment), and oedema distribution (hypoalbuminaemic oedema in kwashiorkor).
Dietary history focuses on: total caloric intake versus estimated requirements, protein intake, specific food groups (red meat, fish, dairy, fruit/vegetables, grains — and whether staple grain is refined/polished), duration and pattern of any restriction, alcohol intake, cultural or religious dietary practices, and recent changes in intake due to illness.
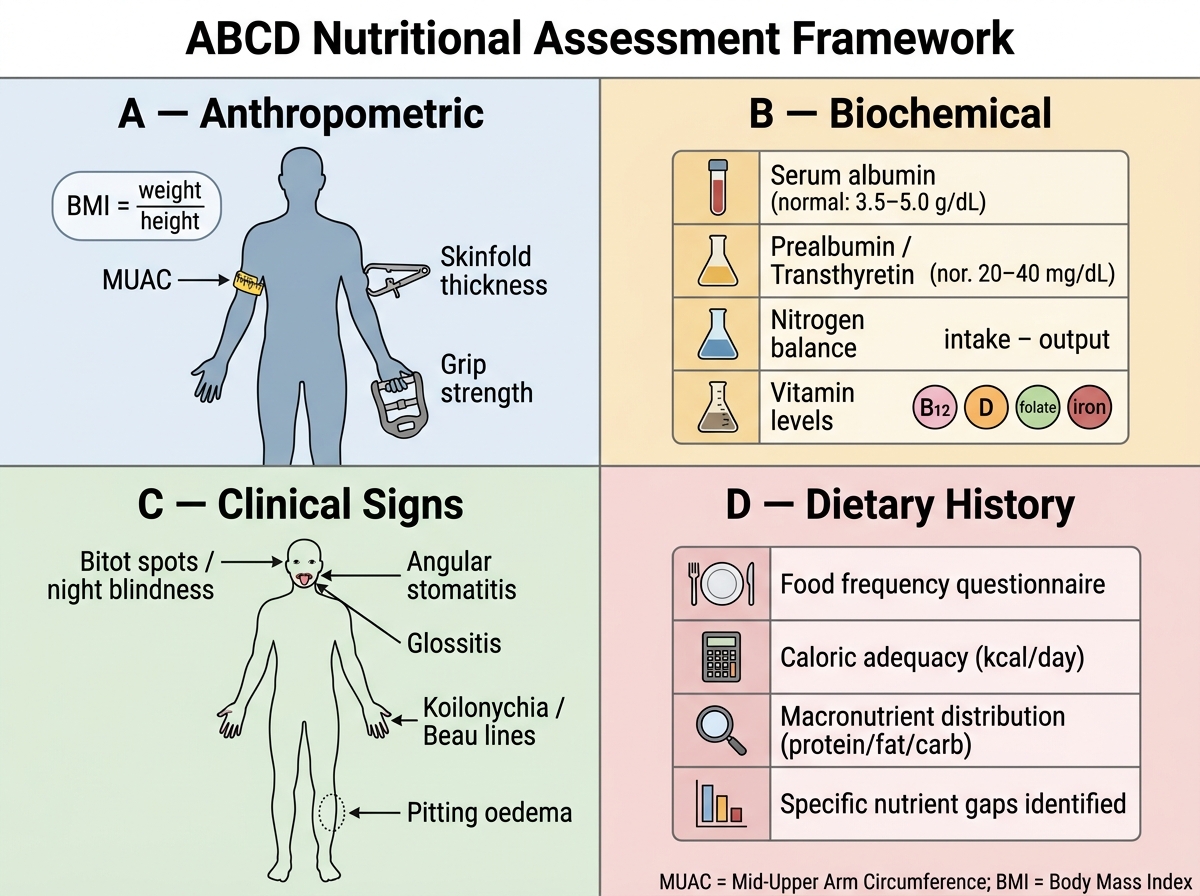
The ABCD Framework for Nutritional Assessment
Protein-Energy Malnutrition and Common Vitamin Deficiencies
Protein-energy malnutrition (PEM) encompasses a spectrum from mild undernutrition to the severe clinical syndromes of marasmus and kwashiorkor, which represent the extremes of adaptation to inadequate intake.
Marasmus is the result of long-standing, severe deprivation of both calories and protein. The body adapts by catabolising its own fat and muscle reserves while maintaining serum protein levels through conservation mechanisms. The clinical picture is extreme wasting: the child or adult appears emaciated with loss of all subcutaneous fat (the face has an 'old man' appearance with prominent cheekbones), severe muscle wasting (thenar, temporal, interossei), the skin is loose and wrinkled over prominent bony prominences, and hair may be thin. Crucially, serum albumin is often normal or only mildly reduced because protein synthesis is partially preserved by the conservation mechanism. There is no oedema. BMI is severely reduced; MUAC is <11.5 cm in children <5 years.
Kwashiorkor results from severe protein deficiency with relatively preserved caloric intake. The hallmark is hypoalbuminaemia — because without protein, hepatic albumin synthesis fails. Low serum albumin reduces plasma oncotic pressure, causing protein-deficiency oedema, which may mask the underlying wasting and give the child a deceptively 'plump' appearance. Additional features: depigmented, patchy skin with a 'flaky paint' or 'crazy paving' dermatosis, flag sign in hair (alternating light and dark bands corresponding to periods of protein deficiency and adequate intake), hepatomegaly from fatty infiltration (protein is required for VLDL synthesis; without it, fat accumulates in the liver), misery and irritability, immunosuppression, and recurrent infections. Serum albumin is severely low (<2.0 g/dL), in contrast to marasmus.
Marasmic kwashiorkor is a mixed picture, the most severely ill form, with both severe wasting and oedema/hypoalbuminaemia.
Consequences of PEM in hospitalised adults: the most clinically important consequences are impaired immunity (increased susceptibility to nosocomial infections, bacterial translocation from the gut, reactivation of latent TB), poor wound healing, prolonged ventilation dependency, decubitus ulcers, and increased mortality.
Vitamin deficiency syndromes — the key clinical presentations:
Vitamin A deficiency: most common cause of preventable childhood blindness. Night blindness (nyctalopia) is the earliest symptom. Bitot spots — greyish white, foamy, triangular xerotic plaques on the bulbar conjunctiva — are pathognomonic. Corneal xerosis progresses to keratomalacia (corneal softening) and blindness. Systemic: impaired epithelial integrity, increased susceptibility to respiratory and GI infections. Treatment: high-dose oral vitamin A supplementation.
Thiamine (B1) deficiency: most commonly seen in populations dependent on polished rice (thiamine is in the bran — removed by polishing) and in chronic alcoholism (poor intake + impaired absorption). Two syndromes: Dry beriberi — peripheral neuropathy (symmetrical, ascending, sensorimotor; burning feet, wasting of distal muscles, foot drop in severe cases). Wet beriberi — high-output cardiac failure (thiamine deficiency impairs oxidative metabolism → anaerobic glycolysis → lactic acidosis → compensatory vasodilation and increased cardiac output → ultimately biventricular failure). The cardiomegaly is biventricular; oedema is present. Wernicke-Korsakoff syndrome in alcoholics: Wernicke encephalopathy (acute — confusion, ophthalmoplegia, ataxia — the classic triad); Korsakoff psychosis (chronic — anterograde amnesia, confabulation). Treatment: thiamine IV/IM before glucose (administering glucose to a thiamine-deficient patient can precipitate acute Wernicke encephalopathy).
Niacin (B3 / nicotinic acid) deficiency — pellagra: the 4 Ds — Dermatitis (symmetrical, photosensitive — Casal necklace around the neck, glove-and-stocking distribution on sun-exposed areas), Diarrhoea, Dementia (cognitive decline, confusion), and untreated, Death. Classic in populations dependent on maize (maize contains niacin in bound form, unavailable unless treated with alkali — the traditional nixtamalisation process). Maize diets also lack tryptophan (a niacin precursor). Treatment: oral nicotinamide (preferred over nicotinic acid — avoids flushing).
Vitamin C (ascorbic acid) deficiency — scurvy: follicular hyperkeratosis (perifollicular haemorrhage — 'corkscrew' hairs), gingival swelling, bleeding, and ulceration (periodontal disease), haemarthroses, impaired wound healing, and anaemia (iron absorption depends on vitamin C — reduced ascorbic acid impairs non-haem iron absorption). The pathophysiology is defective collagen synthesis — ascorbic acid is required as a cofactor for prolyl and lysyl hydroxylase enzymes that hydroxylate proline and lysine residues in procollagen. Treatment: vitamin C 300–500 mg/day oral.
Vitamin D deficiency: the most prevalent nutritional deficiency in India. Caused by inadequate sun exposure (melanin pigment requires longer UV exposure for equivalent vitamin D synthesis) and inadequate dietary intake. Clinical effects: rickets in children (failure of bone mineralisation — bowing of legs, rachitic rosary, Harrison groove, craniotabes); osteomalacia in adults (painful proximal myopathy, aching bones, waddling gait, Looser zones / pseudofractures on X-ray). Biochemistry: low 25-OH vitamin D (<30 nmol/L), low/normal calcium, low phosphate (PTH-driven phosphaturia), elevated PTH, elevated alkaline phosphatase. Treatment: cholecalciferol (D3) supplementation — dosing depends on severity.
Vitamin B12 (cobalamin) and folate deficiency: both cause megaloblastic anaemia — the bone marrow produces enlarged, defective red cells (megaloblasts) from impaired DNA synthesis. Macrocytosis on blood film; hypersegmented neutrophils (≥5 lobes in >5% = pathognomonic). B12 deficiency additionally causes subacute combined degeneration of the spinal cord (SACD) — demyelination of the posterior and lateral columns causing peripheral neuropathy (glove-stocking), loss of vibration and position sense, and spastic paraplegia. This neurological complication is absent in pure folate deficiency — a critical distinguishing point. Causes of B12 deficiency: pernicious anaemia (autoimmune atrophic gastritis with intrinsic factor deficiency — most common cause in adults), strict vegetarian diet (B12 is absent from plant foods — a significant cause in India), gastrectomy, terminal ileal disease (Crohn's, ileal resection — site of B12-intrinsic factor complex absorption). Causes of folate deficiency: poor dietary intake (green leafy vegetables are the primary source), pregnancy and haemolytic anaemias (increased demand), malabsorption (coeliac disease, tropical sprue), methotrexate, trimethoprim, phenytoin (folate antagonists). Treatment: B12 — hydroxocobalamin IM injections (for pernicious anaemia or malabsorption); cyanocobalamin oral (for dietary deficiency). Folate — folic acid 5 mg/day oral; given as prophylaxis in pregnancy to prevent neural tube defects.
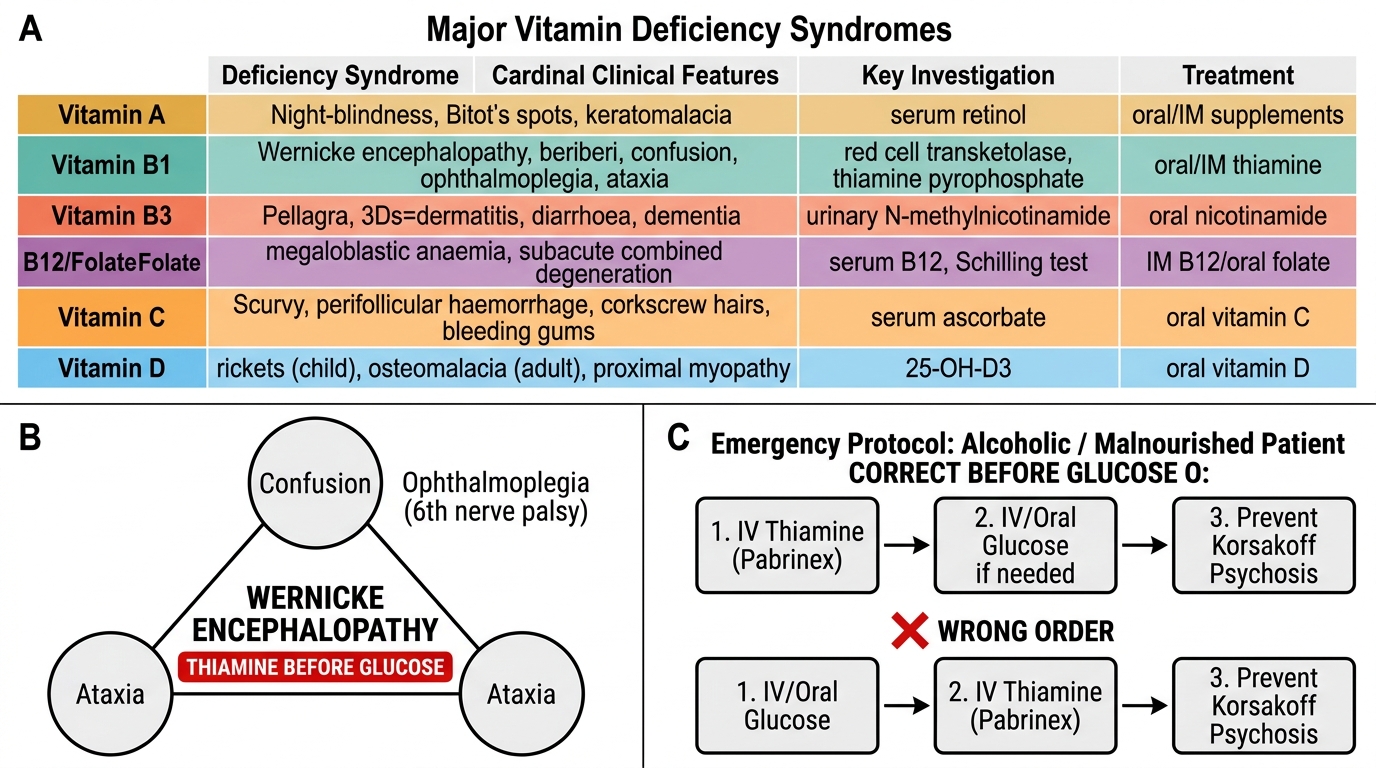
Major Vitamin Deficiency Syndromes: Clinical Reference Table with Wernicke Emergency Protocol
SELF-CHECK
A 45-year-old male chronic alcoholic presents with confusion, bilateral sixth nerve palsy (lateral gaze restriction), and unsteady gait. His blood glucose is 88 mg/dL (normal). What is the MOST IMPORTANT immediate treatment and why should it precede glucose administration?
A. Naloxone IV — to reverse opioid-induced confusion
B. Intravenous 50% dextrose immediately for presumed hypoglycaemia
C. Intravenous thiamine (pabrinex) before or with glucose
D. Oral nicotinamide for pellagra causing confusion
Reveal Answer
Answer: C. Intravenous thiamine (pabrinex) before or with glucose
The triad of confusion, ophthalmoplegia (sixth nerve palsy, or any abnormal eye movement), and ataxia is Wernicke encephalopathy — a thiamine (B1) deficiency emergency. Thiamine is an essential cofactor for pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase, and transketolase. In thiamine deficiency, these reactions are impaired. If glucose is administered first (providing more substrate for glycolysis), the limited thiamine stores are rapidly consumed, precipitating acute decompensation and potentially converting Wernicke encephalopathy to Korsakoff psychosis (which has a poor prognosis for recovery). The rule is thiamine BEFORE glucose in any alcoholic or malnourished patient with altered consciousness. Dose: pabrinex IV (500 mg thiamine component) three times daily for 3 days, then once daily for 5 more days.