Page 1 of 32
IM25.{1-2,18} | Geriatric Foundations and Assessment — SDL Guide
Learning Objectives
- Describe the epidemiology and demographic trends of ageing in India with reference to LASI data and projections
- Explain the concept of homeostenosis and the key pathophysiological changes of normal ageing across organ systems
- Identify the geriatric giants and explain why atypical presentation is characteristic of elderly patients
- Describe the five domains of the Comprehensive Geriatric Assessment and the validated tools used in each domain
- Apply STOPP/START criteria to identify potentially inappropriate medications in elderly patients
- Outline the five management principles of geriatric medicine including polypharmacy review, fall prevention, rehabilitation, advance care planning, and caregiver support
INSTRUCTIONS
Geriatric medicine is one of the fastest-growing fields in Indian internal medicine. This foundational module introduces the epidemiology of ageing in India, the pathophysiology that makes elderly patients different from younger adults, and the Comprehensive Geriatric Assessment — the structured tool that converts a complex clinical picture into a prioritised, interdisciplinary care plan. Master this framework before proceeding to the disease-specific geriatric modules.
References
- Harrison's Principles of Internal Medicine, 21st ed., Part 9 — Geriatric Medicine (textbook)
- API Textbook of Medicine, 11th ed., Chapter on Geriatrics (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 13 — Ageing and Disease (textbook)
- Longitudinal Ageing Study in India (LASI) Wave 1, 2017–18, IIPS Mumbai (guideline)
- American Geriatrics Society Beers Criteria 2023 Update (guideline)
- STOPP/START Criteria Version 2, O'Mahony et al., Age and Ageing 2015 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Krishnamurthy, an 80-year-old retired schoolteacher, arrives at the medicine outpatient department accompanied by his daughter. She reports that over the past six months he has been 'slowing down' — he shuffles when he walks, has fallen twice, forgets appointments, and refuses to eat properly. His medical record lists hypertension, type 2 diabetes, and osteoarthritis. He takes eight medications daily, some prescribed by different specialists. His daughter asks the most challenging question in geriatric medicine: 'Doctor, which of these problems should we treat first?' The answer, as you will discover, is not 'the one with the worst blood test' — it is the one that most threatens his ability to live independently, his dignity, and his quality of life. Geriatric medicine reframes this question by replacing a single-disease, single-organ lens with a multidimensional evaluation of the whole person. This module introduces the foundations of that approach — why the elderly present differently, how demographic change has made geriatric competency an urgent priority in India, and how the Comprehensive Geriatric Assessment transforms a list of diagnoses into an actionable care plan.
WHY THIS MATTERS
India is home to approximately 140 million people aged 60 years and above, a number projected to exceed 300 million by 2050. This demographic transition means that every medical graduate will care for elderly patients across every specialty, not only geriatrics. The elderly are disproportionate consumers of inpatient care, account for a higher burden of polypharmacy-related adverse events, and have longer hospital stays than younger adults with equivalent diagnoses. The unique challenge — atypical disease presentation, multiple concurrent chronic conditions, and functional decline as the common final pathway — demands a clinical framework that transcends single-disease management. NMC competency IM25.1, 25.2, and 25.18 address this foundation: epidemiology and disease course in the elderly, multidimensional geriatric assessment, and the demographic imperative. Mastering this material prepares you to provide holistic, safe, and effective care to India's rapidly growing elderly population.
RECALL
Before engaging with geriatric medicine, activate what you already know. The ageing process involves predictable physiological changes across organ systems: declining glomerular filtration rate (normal drop approximately 1 mL/min/year after age 40), reduced hepatic blood flow and cytochrome P450 activity affecting drug metabolism, reduced lung compliance and forced vital capacity, decreased bone mineral density, reduced muscle mass (sarcopenia), and declining homeostatic reserve (the ability to respond to physiological stress). You have also studied pharmacokinetics — how ageing alters drug absorption, distribution, metabolism, and excretion. Recall that protein binding is reduced in malnutrition (common in the elderly), increasing the free fraction of protein-bound drugs. Recall the difference between disease prevalence and incidence, and how the epidemiological transition describes the shift from communicable to non-communicable disease burden. These foundations underpin the geriatric framework you are about to build.
Epidemiology and Demography of Ageing in India
Geriatric medicine is the branch of internal medicine concerned with the health care of elderly persons, defined by the World Health Organization as individuals aged 60 years and above in developing countries (including India) and 65 years and above in developed countries. The distinction matters because India's elderly experience age-related physiological decline and disease burden at younger chronological ages than Western counterparts, likely reflecting a cumulative lifetime burden of nutrition, infection, occupational hazard, and healthcare access. Understanding the demographic and epidemiological context is not merely academic — it defines the clinical scale of the challenge every Indian physician will face.
Provided image
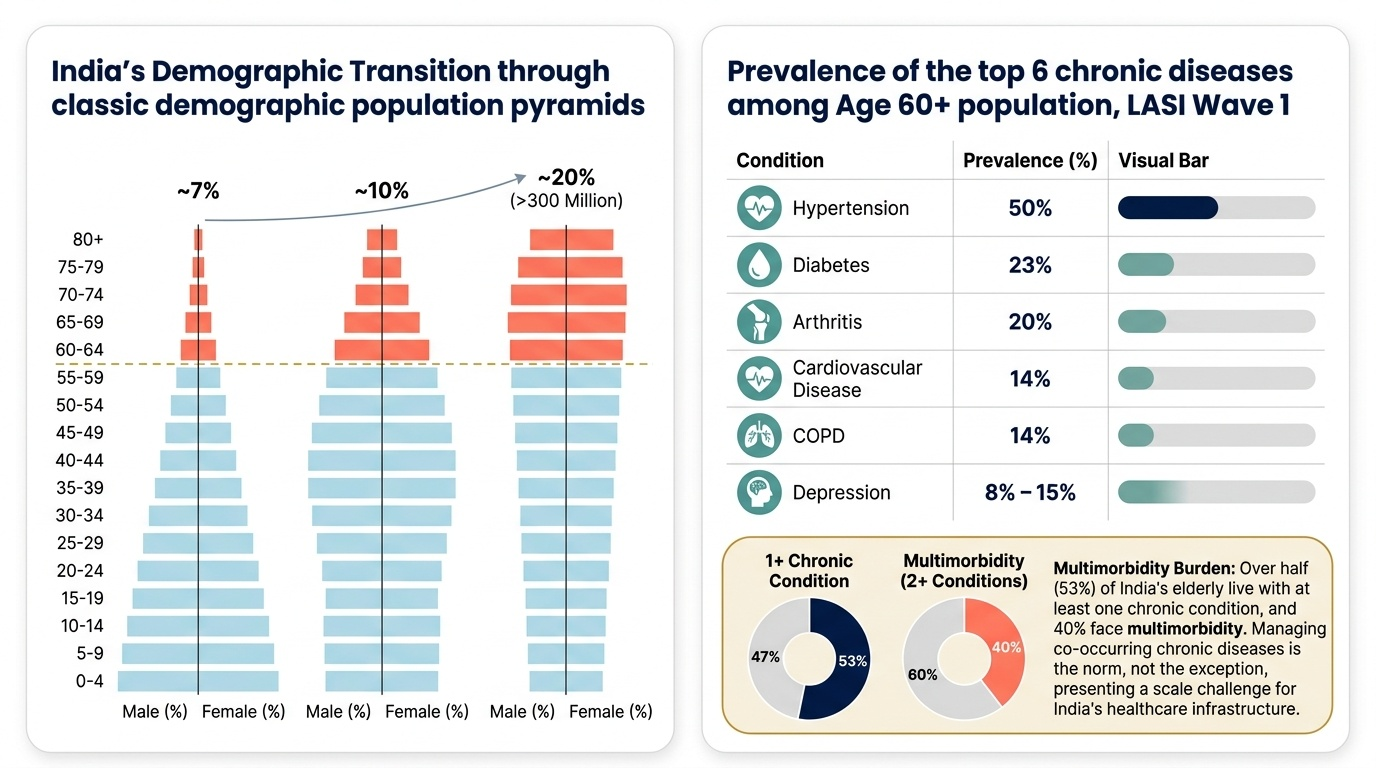
Demographic transition in India: According to the Longitudinal Ageing Study in India (LASI) Wave 1 (2017–18), India had approximately 103 million people aged 60 and above, representing 8.6% of the total population. By 2050, this number is projected to exceed 300 million (approximately 20% of the projected population). The old-age dependency ratio — the number of persons aged 60+ per 100 working-age persons — is rising steeply. Simultaneously, the total fertility rate has declined to near-replacement level, meaning the working-age population will not grow proportionally. The combination of increasing longevity and declining fertility is the double driver of population ageing. India is ageing rapidly but remains a lower-middle-income country, meaning this demographic shift occurs in a context of relatively limited healthcare infrastructure, sparse geriatric specialist training, and weak social safety nets — creating the 'demographic dividend becoming a demographic burden' scenario if not anticipated.
Morbidity and burden of disease in the elderly: Elderly Indians carry a disproportionate burden of non-communicable diseases (NCDs): the LASI survey documented that approximately 53% of those aged 60+ have at least one chronic condition, and approximately 40% have two or more. The leading conditions are hypertension (50%), diabetes (23%), cardiovascular disease (14%), chronic obstructive pulmonary disease (14%), arthritis (20%), and depression (8–15% depending on instrument). Importantly, multimorbidity — the co-occurrence of two or more chronic conditions — is the norm, not the exception. Managing multimorbidity with a single-disease guideline approach risks polypharmacy, drug-drug interactions, and competing treatment targets.
Atypical disease presentation: One of the cardinal principles of geriatric medicine is that diseases often present atypically in older patients. Common examples include: myocardial infarction presenting without chest pain (silent MI — more common in elderly diabetics); pneumonia presenting with confusion rather than fever and productive cough; urinary tract infection presenting with acute confusion (delirium) rather than dysuria; hyperthyroidism presenting as weight loss and atrial fibrillation without heat intolerance or tremor (apathetic thyrotoxicosis); and appendicitis presenting with minimal peritonism due to blunted pain perception and reduced abdominal wall rigidity. The common pathways — delirium, falls, incontinence, immobility — are called the geriatric giants (described by Bernard Isaacs, 1965), representing the four great clinical syndromes through which most serious illness manifests in the elderly, regardless of the underlying diagnosis.
Frailty is a distinct geriatric syndrome characterised by a state of decreased reserve and resistance to stressors, resulting from cumulative decline across physiological systems. The Fried phenotype (2001) defines frailty by five criteria: unintentional weight loss >4.5 kg in the past year, self-reported exhaustion, weak grip strength (below gender- and BMI-specific thresholds), slow gait speed (<0.8 m/s), and low physical activity. Meeting 3 or more criteria = frail; 1–2 = pre-frail; 0 = robust. Frailty is distinct from, but overlaps with, disability (loss of the ability to perform activities of daily living) and multimorbidity (multiple diagnoses). A frail patient has greatly increased risk of falls, hospitalisation, functional decline after acute illness, and death. Recognising frailty before an acute stressor allows preventive and rehabilitative interventions.
The epidemiology of specific diseases in the elderly differs quantitatively and qualitatively from the general population: stroke incidence doubles with each decade after age 55, making it the leading cause of acquired disability in the elderly; hip fracture (the most dangerous complication of osteoporosis and falls) carries a 20–25% one-year mortality in the elderly; dementia prevalence doubles every five years after age 65, reaching approximately 33% by age 85; and polypharmacy (defined as ≥5 concurrent medications) is present in over 40% of elderly Indian patients, creating cumulative adverse-event burden.
Pathophysiology of Ageing and Age-Related Disease
The pathophysiological basis of geriatric medicine lies in understanding what distinguishes 'normal ageing' from 'disease', and how the reserve depletion of normal ageing amplifies the impact of any superimposed disease. The key conceptual framework is homeostenosis — the progressive narrowing of homeostatic reserve across physiological systems with advancing age. Under normal resting conditions, the elderly person may appear clinically indistinguishable from a younger adult. However, when stressed — by infection, surgery, dehydration, drugs, or injury — the elderly individual has less reserve to call upon and therefore decompensates more readily, more severely, and across multiple organ systems simultaneously. This explains why a urinary tract infection can produce florid delirium in an 85-year-old but only dysuria in a 30-year-old.
Cellular and molecular mechanisms of ageing: Ageing is driven by several interrelated cellular processes. Telomere shortening — the progressive erosion of chromosomal end-sequences with each cell division — triggers replicative senescence when the critically short telomere activates the p53-mediated DNA damage response, preventing further cell division. Mitochondrial dysfunction leads to increased production of reactive oxygen species (ROS), causing oxidative damage to proteins, lipids, and DNA; mitochondrial biogenesis declines with age. Cellular senescence — a stable cell cycle arrest in response to stressors — promotes tissue inflammation through the senescence-associated secretory phenotype (SASP), where senescent cells secrete pro-inflammatory cytokines (IL-6, IL-8, TNF-α), matrix metalloproteinases, and growth factors. Accumulation of senescent cells drives inflammaging — the chronic, low-grade sterile inflammatory state that underlies many age-related diseases including atherosclerosis, Alzheimer disease, type 2 diabetes, and sarcopenia. Autophagy — the cellular housekeeping system that degrades damaged proteins and organelles — declines with age, allowing accumulation of protein aggregates (amyloid-β in Alzheimer, α-synuclein in Parkinson).
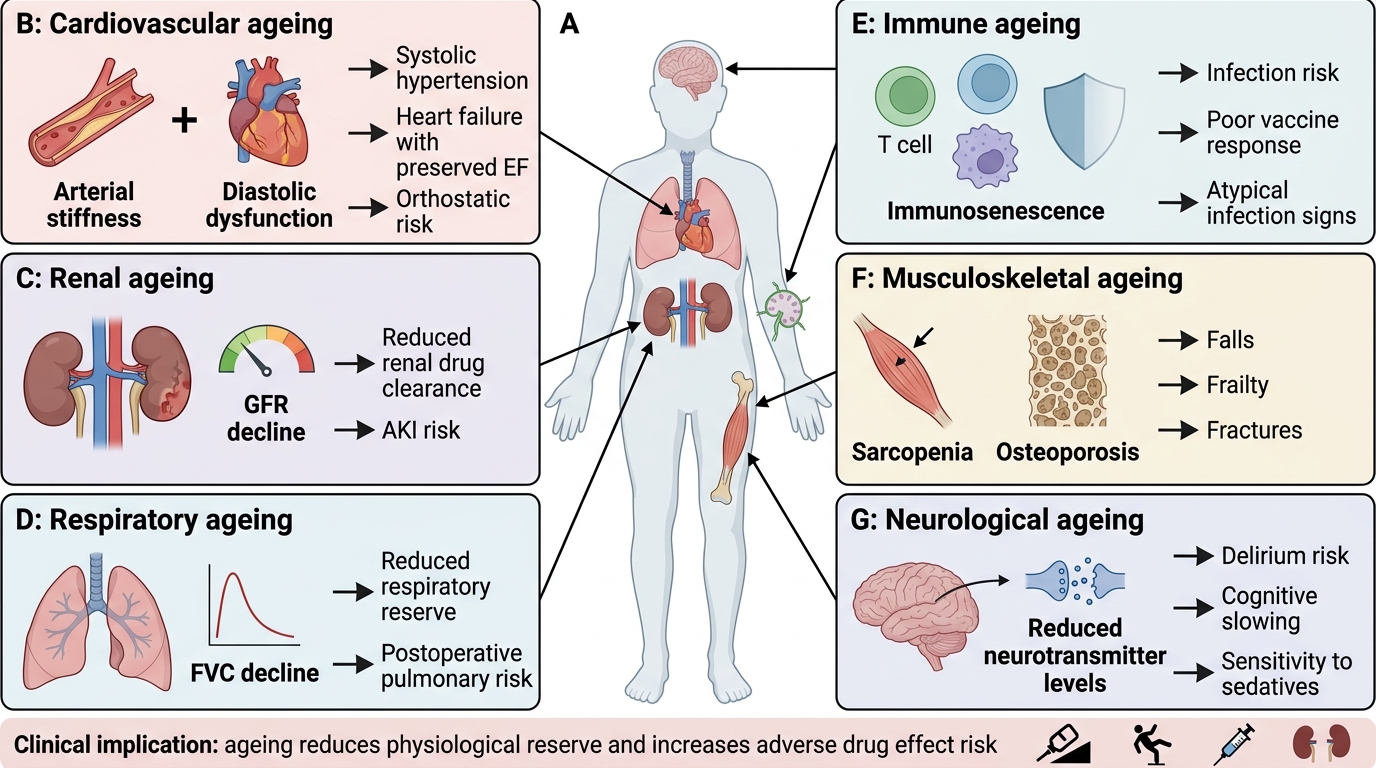
Organ-specific age-related changes: The cardiovascular system shows arterial stiffening (reduced aortic compliance → increased systolic blood pressure and pulse wave velocity, widened pulse pressure), myocardial hypertrophy (concentric), reduced maximum heart rate (220 − age formula), and diastolic dysfunction (prolonged isovolumetric relaxation time). The renal system shows declining nephron number (approximately 30% loss by age 75), reduced tubular secretion, and consequently reduced GFR — estimated by the CKD-EPI or MDRD equation, both validated in older adults — though serum creatinine may remain normal because muscle mass (creatinine source) also declines. Drug dosing in the elderly must be GFR-based, not creatinine-based. The respiratory system shows decreased lung elasticity, reduced mucociliary clearance, and blunted hypoxic/hypercapnic ventilatory response. The immune system undergoes immunosenescence — thymic involution, reduction in naïve T-cell output, and shift toward memory T cells with reduced repertoire diversity, impairing response to new infections and reducing vaccine efficacy. Thermoregulation becomes impaired (risk of both hypothermia and heat stroke). Gastrointestinal changes include reduced gastric acid secretion (achlorhydria), delayed gastric emptying, and reduced intestinal motility.
Age-Related Physiological Changes and Clinical Implications
Pharmacological implications of ageing: Age-related pharmacokinetic changes create predictable hazards. Absorption is relatively preserved. Distribution changes because body fat increases and lean body mass and total body water decrease — lipophilic drugs (e.g., benzodiazepines, tricyclic antidepressants) have a larger volume of distribution and longer half-life; hydrophilic drugs (e.g., digoxin, aminoglycosides, lithium) have a smaller volume of distribution and higher peak concentrations at standard doses. Protein binding may be reduced in hypoalbuminaemia (malnutrition, liver disease) — increasing free fraction of protein-bound drugs (phenytoin, warfarin). Hepatic metabolism declines (reduced hepatic blood flow and CYP450 activity). Renal excretion declines with GFR. Pharmacodynamically, the elderly central nervous system is more sensitive to sedatives, opioids, and anticholinergic drugs, and the cardiovascular system is more sensitive to antihypertensives (orthostatic hypotension risk). These changes form the basis of Beers Criteria and STOPP/START criteria (detailed in the Geriatric Foundations module).
SELF-CHECK
An 80-year-old man with stable type 2 diabetes and hypertension is prescribed a new medication. His serum creatinine is 1.1 mg/dL (within normal limits). His calculated eGFR (CKD-EPI) is 42 mL/min/1.73 m². Which principle BEST explains why dose adjustment is required despite 'normal' creatinine?
A. Creatinine production increases with age, making serum creatinine an unreliable marker
B. Renal tubular secretion is enhanced in the elderly, increasing drug clearance
C. Muscle mass declines with age, so creatinine generation decreases; serum creatinine underestimates the degree of GFR reduction
D. Protein binding of the drug increases in old age, raising the free fraction
Reveal Answer
Answer: C. Muscle mass declines with age, so creatinine generation decreases; serum creatinine underestimates the degree of GFR reduction
In elderly patients, age-related sarcopenia (muscle mass loss) reduces creatinine production. Therefore, serum creatinine may remain in the 'normal' range even when GFR is substantially reduced, because less creatinine is being generated. Drug dosing must be based on calculated eGFR (CKD-EPI or MDRD), not on serum creatinine alone — this is a fundamental geriatric pharmacology principle. Enhanced tubular secretion is incorrect (tubular function declines). Protein binding reduction (not increase) is relevant to some drugs but does not explain this scenario.
Comprehensive Geriatric Assessment: Principles and Domains
The Comprehensive Geriatric Assessment (CGA) is the cornerstone of geriatric clinical practice. It is a multidimensional, interdisciplinary diagnostic process designed to identify and address the medical, psychological, functional, and social needs of elderly patients, with the ultimate aim of developing a coordinated, integrated plan for treatment and long-term follow-up. The evidence for CGA is strong: systematic reviews demonstrate that CGA reduces mortality (relative risk approximately 0.75), reduces rates of admission to long-term care (nursing homes), improves functional status at follow-up, and is cost-effective in hospitalised elderly patients. Critically, CGA identifies problems that standard medical assessment misses — approximately one-third of CGA-identified problems are not detected by routine assessment.
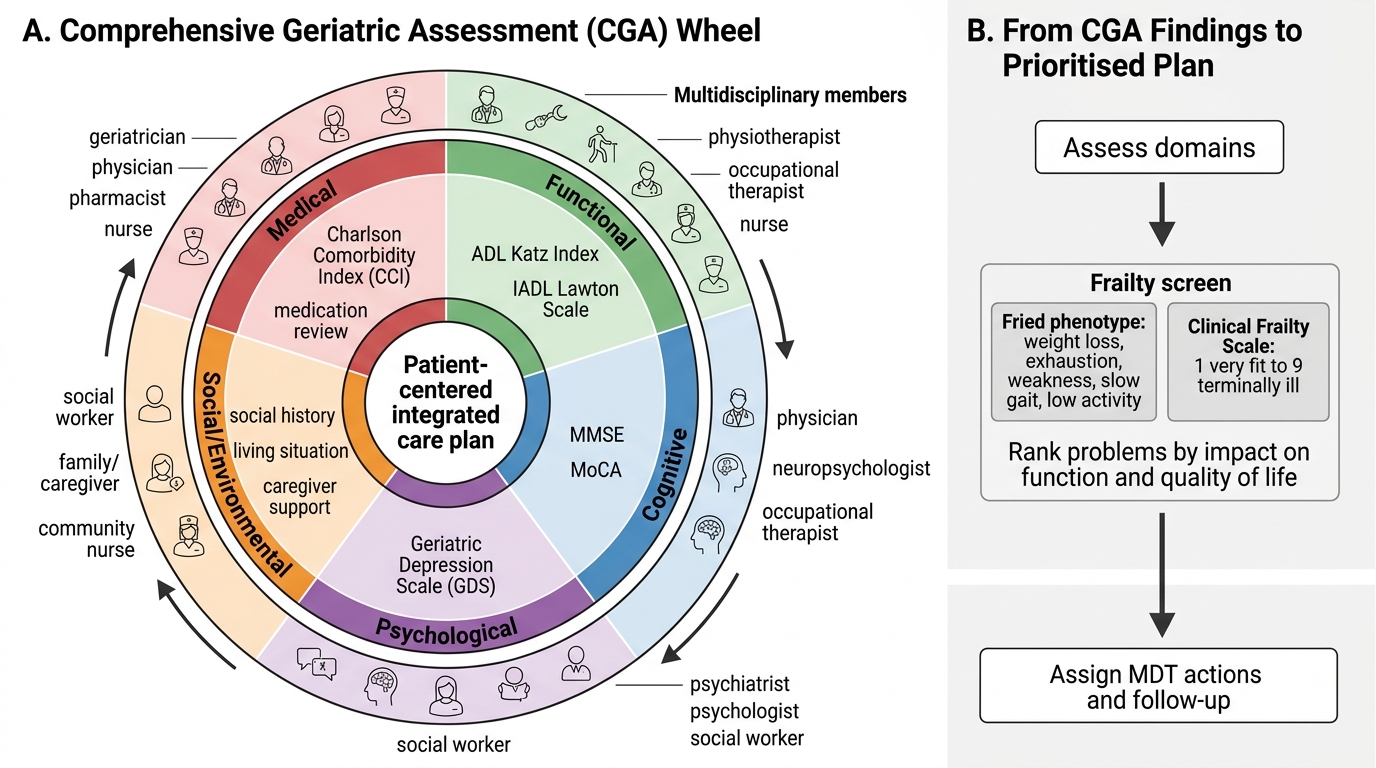
CGA is not a single test — it is a structured process conducted by a multidisciplinary team typically comprising a geriatrician, geriatric nurse, social worker, physiotherapist, occupational therapist, and, where available, dietitian, neuropsychologist, and pharmacist. In the Indian public health context, CGA may be conducted at varying levels of completeness depending on resource availability, but the core domains must be addressed even in resource-limited settings.
Domain 1 — Medical assessment: Comprehensive review of all current diagnoses; assessment of symptom burden; medication reconciliation (listing all medications including over-the-counter drugs, herbal preparations, and those prescribed by multiple physicians — essential for polypharmacy detection); assessment of comorbidity burden using validated tools such as the Charlson Comorbidity Index (CCI), which assigns weights to 17 conditions and generates a score predictive of 10-year mortality; nutritional screening (covered in the nutrition module); assessment for geriatric syndromes (falls, delirium, pressure ulcers, urinary incontinence, polypharmacy).
Domain 2 — Functional assessment: Evaluation of the patient's ability to perform activities needed for daily living. Two validated hierarchical scales are standard:
- Activities of Daily Living (ADL) — Katz scale (1963): Six basic self-care tasks: bathing, dressing, toileting, transferring (getting from bed to chair), continence, and feeding. Scored 0–6; a score of 0 indicates complete dependence. ADL measures the most fundamental tier of function and detects moderate-to-severe disability.
- Instrumental Activities of Daily Living (IADL) — Lawton scale (1969): Eight higher-order tasks: using a telephone, shopping, food preparation, housekeeping, laundry, mode of transportation, responsibility for own medications, and ability to handle finances. IADLs are more sensitive for early cognitive or functional impairment, as these complex tasks are lost before basic ADLs in most conditions. Typically, ADL and IADL are used together to characterise the full functional spectrum.
Domain 3 — Cognitive assessment: Screening for dementia and delirium using validated instruments. The Mini-Mental State Examination (MMSE) — a 30-point questionnaire assessing orientation (time, place), registration, attention/calculation (serial 7s), recall, language, and visuospatial ability — remains the most widely used cognitive screening tool globally. Scores: 24–30 = normal; 18–23 = mild impairment; 0–17 = severe impairment. The Montreal Cognitive Assessment (MoCA) is more sensitive for mild cognitive impairment (MCI); it adds visuospatial (clock drawing, cube copy), executive function, and verbal fluency domains absent from the MMSE. A score <26/30 is the standard MCI cutoff.
Domain 4 — Psychological assessment: Screening for depression using the Geriatric Depression Scale (GDS) — validated for the elderly (avoids somatic items that overlap with physical illness); 15-item short version: score ≥5 = probable depression (sensitivity 92%, specificity 89%); 30-item long version: ≥11. Detection is critical because depression in the elderly is under-recognised, undertreated, and contributes substantially to functional decline, mortality, and quality of life impairment.
Domain 5 — Social and environmental assessment: Evaluation of living arrangements (alone vs with family), caregiver support and caregiver burden, financial resources, safety of the home environment (fall hazards: loose rugs, poor lighting, lack of grab bars), and social participation and isolation. In the Indian context, the traditional joint family structure provides inherent social support for many elderly, but urbanisation, migration, and nuclear family trends are eroding this. Social assessment also includes identifying elder abuse (physical, psychological, financial, neglect) — an underreported problem with an Indian prevalence estimated at 14–50% depending on definition and study population.
Comprehensive Geriatric Assessment Wheel and Care Planning
Domain 6 — Frailty assessment: Formal assessment using the Fried phenotype (five criteria: weight loss, exhaustion, weakness, slow gait speed, low activity) or the Clinical Frailty Scale (CFS) (Rockwood 2005) — a 9-point pictographic scale ranging from 1 (very fit) to 9 (terminally ill), widely used in acute settings for rapid frailty identification. Frailty status influences prognosis, surgical risk, and the appropriateness of aggressive intervention versus comfort-focused care.
The CGA output is not simply a list of problems — it is a prioritised, integrated care plan that sets realistic treatment goals, assigns responsibilities across the MDT, schedules follow-up, and addresses the patient's own preferences and values. The crucial skill is translating CGA findings into a hierarchy: which problem, if treated first, will most improve function and quality of life? In Krishnamurthy's case, the answer might be: address polypharmacy first (reducing fall risk), then rehabilitation for the falls, then depression screening.
SELF-CHECK
A 76-year-old woman living alone can bathe and dress independently (ADL intact) but has difficulty managing her medications, using public transport, and handling bank transactions. On the Lawton IADL scale, she scores 5/8. Which conclusion BEST describes her functional status?
A. She has severe disability requiring institutional care
B. She has preserved basic self-care (ADL intact) but compromised higher-order instrumental function (IADLs impaired), suggesting early to moderate cognitive or physical decline
C. Her ADL and IADL findings are inconsistent and require re-testing with MMSE
D. Lawton IADL is not validated for patients living alone and should be replaced with Katz ADL
Reveal Answer
Answer: B. She has preserved basic self-care (ADL intact) but compromised higher-order instrumental function (IADLs impaired), suggesting early to moderate cognitive or physical decline
ADL (Katz) measures basic self-care and is intact. IADL (Lawton) measures higher-order tasks and is partially impaired (5/8). This pattern — intact ADL with reduced IADLs — is the hallmark of early functional decline, typically driven by mild cognitive impairment or early dementia. IADLs are lost before ADLs in most progressive conditions. This finding should prompt cognitive screening (MMSE/MoCA) and review of social support. Institutional care would not be triggered solely by IADL impairment with intact ADL. Lawton IADL is validated regardless of living situation.