Page 11 of 32
IM25.{8,12-14} | Geriatric Musculoskeletal Disorders — SDL Guide (Part 2)
Osteoporosis: Management and Fracture Prevention
Management of osteoporosis targets three goals: reducing bone resorption or stimulating bone formation (pharmacological), ensuring adequate substrate (calcium and vitamin D), and preventing falls (the mechanical trigger for most fractures). The principle of fracture liaison services (FLS) — a systematic approach to identifying all patients who present with fragility fracture and ensuring they receive appropriate investigation and treatment — is the evidence-based framework for reducing secondary fractures; up to 50% of patients with hip fracture have had a prior fragility fracture that was not investigated or treated.
Non-pharmacological management: Weight-bearing exercise (walking, resistance training) stimulates bone formation through mechanical loading. Fall prevention (see separate section). Smoking cessation (smoking is an independent risk factor for osteoporosis — increases osteoclast activity and reduces oestrogen levels). Alcohol reduction (>3 units/day increases fracture risk). Calcium and vitamin D supplementation should be provided to all patients receiving pharmacological therapy for osteoporosis: calcium 1000–1200 mg/day (from dietary sources first — dairy, fortified foods; supplement the gap); vitamin D 800–1000 IU/day (cholecalciferol). In the Indian context, vitamin D deficiency is highly prevalent even in sun-rich regions due to skin pigmentation, covered clothing, and limited outdoor activity in the elderly.
Pharmacological treatment:
- Bisphosphonates are the first-line treatment: alendronate (70 mg weekly oral — first-line for most patients), risedronate (35 mg weekly oral), zoledronic acid (5 mg IV infusion once yearly — preferred when oral not tolerated or absorbed, after hip fracture to reduce re-fracture risk). Mechanism: bisphosphonates are incorporated into bone matrix and ingested by osteoclasts during resorption, inhibiting farnesyl pyrophosphate synthase (mevalonate pathway) → osteoclast apoptosis → reduced bone resorption. Oral bisphosphonates must be taken on an empty stomach with a full glass of water and the patient must remain upright for 30 minutes (to prevent oesophageal erosion). Contraindicated in CKD with eGFR <30–35 mL/min. Duration: typically 3–5 years for alendronate/risedronate (drug holiday after 5 years in low-risk patients); zoledronic acid 3 injections then reassess. Atypical femoral fractures (rare, transverse subtrochanteric fractures after long-term bisphosphonate use) and osteonecrosis of the jaw (rare, associated with high-dose IV bisphosphonates for malignancy) are rare but recognised adverse effects — inform patients.
- Denosumab (60 mg SC every 6 months) — a RANK ligand monoclonal antibody; inhibits osteoclastogenesis; suitable when bisphosphonates not tolerated or in CKD (can be used with eGFR <30, though hypocalcaemia risk — ensure calcium/vitamin D adequate first); no renal excretion. Critical point: do NOT stop denosumab abruptly — rapid bone loss and rebound vertebral fractures can occur; transition to bisphosphonate when stopping.
- Teriparatide (recombinant PTH 1-34, 20 mcg SC daily) — the primary bone-forming (anabolic) agent; indicated for severe osteoporosis (multiple fractures or very low BMD) or inadequate response to antiresorptive therapy; maximum duration 24 months; expensive and requires SC injection.
- Hormone replacement therapy (HRT) — oestrogen reduces postmenopausal bone loss and prevents vertebral and hip fracture, but its use is primarily guided by menopausal symptoms rather than osteoporosis alone; appropriate for women with premature menopause (before age 45) where it provides both skeletal and cardiovascular protection.
Fracture management — hip fracture: The Fix 48 principle: hip fracture surgery within 48 hours of admission reduces mortality, pain, delirium, and pressure ulcer incidence. Subcapital fractures in the elderly: hemiarthroplasty (femoral head replacement) or total hip replacement (better functional outcomes in active patients). Intertrochanteric fractures: dynamic hip screw (DHS) or intramedullary nail. Post-operatively: early mobilisation (weight-bearing day 1 with physiotherapy support), VTE prophylaxis, delirium prevention bundle, nutritional support.
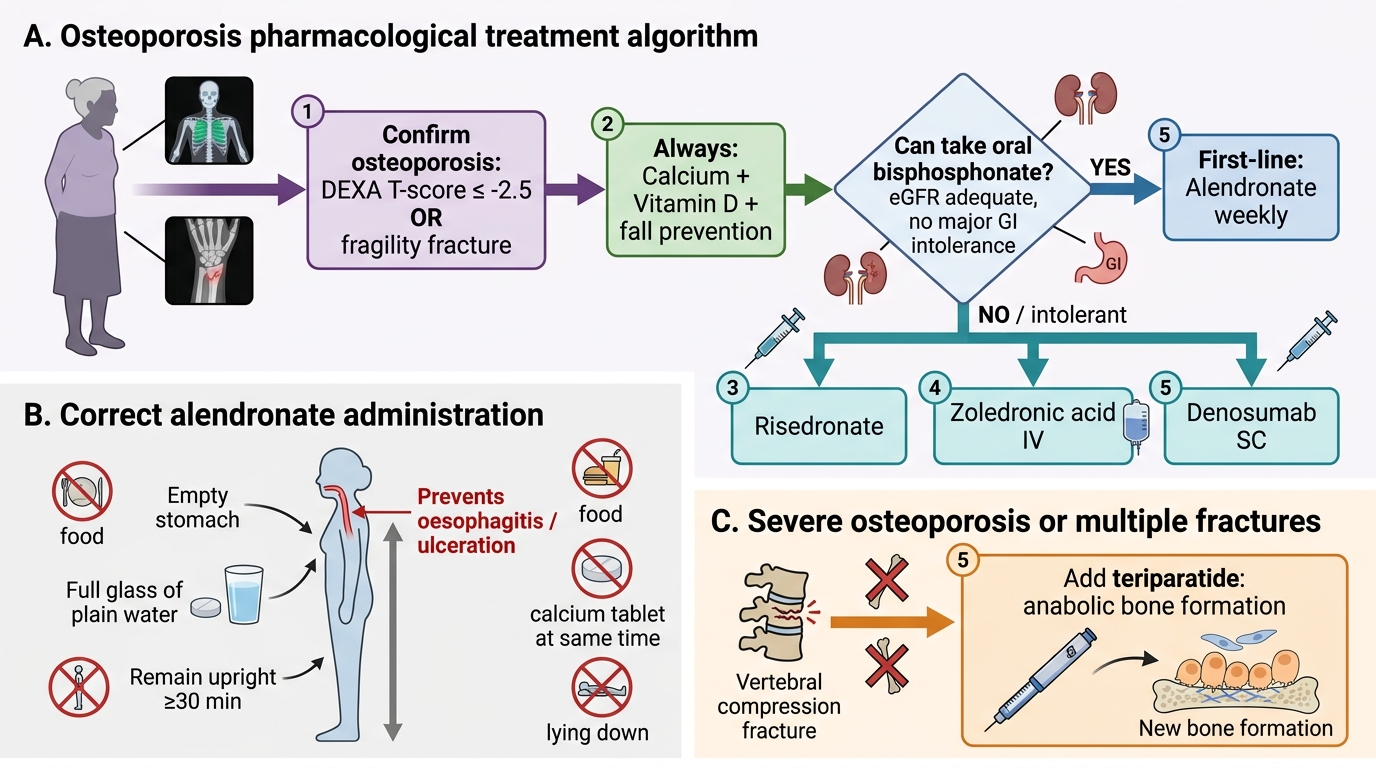
Osteoporosis Pharmacological Treatment Algorithm
SELF-CHECK
A 72-year-old woman with a recent Colles fracture and DEXA T-score of -2.8 at the lumbar spine is prescribed alendronate 70 mg weekly. Her eGFR is 55 mL/min. She asks about the correct way to take the medication. Which instruction is MOST important to prevent a serious adverse effect?
A. Take alendronate with food to improve absorption and reduce nausea
B. Take alendronate with a calcium supplement in the evening before bed
C. Take alendronate with a full glass of water on an empty stomach and remain upright for at least 30 minutes
D. Take alendronate twice daily to achieve optimal bone density improvement
Reveal Answer
Answer: C. Take alendronate with a full glass of water on an empty stomach and remain upright for at least 30 minutes
Oral bisphosphonates (alendronate, risedronate) must be taken fasting (empty stomach) with a full glass of plain water, and the patient must remain upright (seated or standing — not lying down) for at least 30 minutes after ingestion. This is to prevent the drug pooling in the oesophagus where it causes oesophageal erosion, oesophagitis, or ulceration — one of the main reasons for discontinuation. Food and calcium supplements reduce absorption (bisphosphonates should be taken 30 minutes before any food/other medications). Alendronate is weekly, not twice daily. Her eGFR of 55 is above the threshold for bisphosphonate use (avoid if <30–35 mL/min).
Falls Prevention and Common Fractures in the Elderly
Falls prevention is most effective when it is multifactorial — addressing multiple risk domains simultaneously in a coordinated intervention. The evidence for single-component interventions (exercise alone, home modification alone) shows modest benefit; multi-component programmes reduce fall incidence by 24% (Cochrane review 2019, Sherrington et al.). The components of an evidence-based falls prevention programme are:
1. Exercise interventions: Balance and gait training is the most effective single component (reduces falls by 23%). Programmes with the highest evidence: Otago Exercise Programme (individually prescribed home exercise programme of leg strengthening and balance retraining — 35% reduction in falls, 35% reduction in injury rates, originally validated in New Zealand but applicable in India); Tai Chi (group balance training — 19% reduction in falls in community-dwelling elderly); strength and balance classes (Falls Management Exercise, FaME). Exercise prescription must be tailored to the individual's baseline capability and monitored for progression.
2. Medication review: Reducing the number of medications (polypharmacy reduction) and specifically targeting high-risk medications for falls: benzodiazepines (gradual taper and stop — withdrawal symptoms require slow titration over weeks to months); first-generation antihistamines (replace with non-sedating antihistamines); TCAs (replace with SSRI if antidepressant needed); antihypertensives (review BP targets — evidence that tight BP control in the very frail elderly may cause more harm from falls than the cardiovascular benefit justifies); antipsychotics (reduce dose or discontinue where possible).
3. Vision correction: Uncorrected visual impairment doubles falls risk. Annual ophthalmology review; expedite cataract surgery where indicated (cataract is the most common surgically correctable cause of visual impairment in Indian elderly); appropriate spectacle correction.
4. Vitamin D supplementation: Vitamin D deficiency impairs muscle strength and neuromuscular coordination in addition to causing osteomalacia; supplementation with 800–1000 IU/day reduces falls risk in vitamin D-deficient elderly (NNT approximately 15 to prevent one fall).
5. Home hazard modification: Occupational therapy home assessment targeting: removal of loose rugs and electrical cords; installation of grab bars in bathroom and toilet; non-slip flooring; adequate lighting in hallways and stairways; raised toilet seats; bed rails; removal of clutter from walking paths.
6. Management of orthostatic hypotension: Identify and modify causative medications (antihypertensives — review target BP; diuretics — review necessity); non-pharmacological: compression stockings, adequate hydration, head-of-bed elevation (reduces overnight pressure natriuresis); midodrine or fludrocortisone for severe symptomatic cases.
Common fractures in the elderly:
- Hip fracture (neck of femur + intertrochanteric + subtrochanteric): most serious — 20–25% one-year mortality, 50% permanent disability. The vast majority are preceded by falls. Subcapital fractures: Garden classification I–IV (determines blood supply viability); Garden I–II (incomplete, impacted) may be treated with internal fixation; Garden III–IV (displaced — higher risk of avascular necrosis of femoral head) require hemiarthroplasty or THR in elderly. Intertrochanteric: DHS or intramedullary nail. Key geriatric principle: operate within 48 hours (FIX 48). Post-op: start IV or SC zoledronate before discharge (IV zoledronic acid after hip fracture reduces subsequent fracture risk by 35% — evidence from HORIZON Recurrent Fracture Trial).
- Vertebral compression fracture: most common osteoporotic fracture; may be asymptomatic or present with acute back pain, kyphosis, height loss. Diagnosis: lateral X-ray spine; MRI for acute vs chronic. Management: analgesia (paracetamol, weak opioids in elderly — avoid NSAIDs and strong opioids if possible), back bracing for acute phase, vertebroplasty/kyphoplasty for persistent pain unresponsive to 4–6 weeks conservative management. Start antiresorptive therapy (bisphosphonate/denosumab) regardless of prior treatment status.
- Colles fracture (distal radius): most common upper limb fragility fracture; treat with closed reduction and cast in elderly if not significantly displaced; K-wire fixation or ORIF for displaced fractures. Investigate and treat underlying osteoporosis.
- Pelvic/pubic ramus fractures: common in frail elderly following minimal trauma; often managed conservatively with analgesia and early mobilisation; VTE prophylaxis essential.
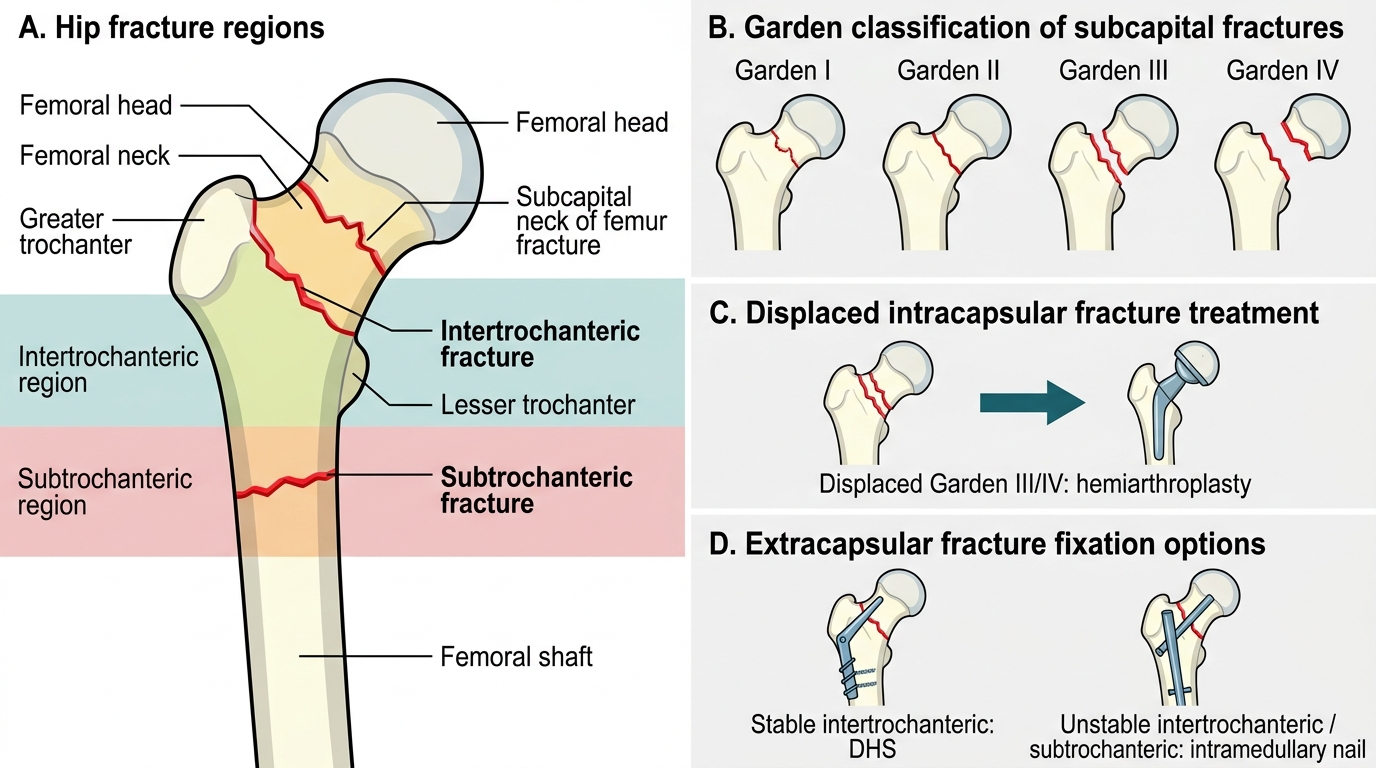
Hip Fracture Classification and Surgical Management
SELF-CHECK
A 77-year-old man undergoes right hip hemiarthroplasty for a displaced subcapital neck of femur fracture. He has a DEXA T-score of -2.9 and has not previously been treated for osteoporosis. What is the MOST EVIDENCE-BASED pharmacological intervention to reduce his risk of further osteoporotic fracture before hospital discharge?
A. Start oral alendronate 70 mg weekly — the most convenient oral option
B. Prescribe calcium and vitamin D supplementation alone — sufficient for fracture prevention post-surgery
C. Administer intravenous zoledronic acid 5 mg as a single annual infusion — the HORIZON Recurrent Fracture Trial demonstrates 35% reduction in subsequent fractures after hip fracture
D. Start denosumab 60 mg SC — preferred over bisphosphonates after major fracture
Reveal Answer
Answer: C. Administer intravenous zoledronic acid 5 mg as a single annual infusion — the HORIZON Recurrent Fracture Trial demonstrates 35% reduction in subsequent fractures after hip fracture
The HORIZON Recurrent Fracture Trial specifically demonstrated that a single annual IV infusion of zoledronic acid 5 mg, initiated 2 or more weeks after hip fracture surgery, reduces subsequent non-vertebral fractures by 35% and all-cause mortality by 28%. This is the highest-level evidence for fracture prevention specifically after hip fracture. IV zoledronate is particularly appropriate here because: oral bisphosphonates may not be tolerated post-operatively when the patient is not yet reliably taking food; IV administration bypasses gastrointestinal absorption issues; and the once-yearly regimen improves adherence. Calcium and vitamin D alone are insufficient for fracture prevention in confirmed osteoporosis.
Self-Assessment: Musculoskeletal Case Integration
The following scenarios integrate all four topics — osteoporosis, osteoarthritis, falls, and fractures — as they coexist in real elderly patients. Test your ability to prioritise management across these domains simultaneously.
Scenario A: Mrs Padmavathi, 73 years old, presents with acute onset back pain after bending to pick up a bag of rice. She reports three episodes of similar back pain in the past two years, each resolving within 4–6 weeks. She has been on prednisolone 10 mg daily for 4 years for rheumatoid arthritis. She has not had a DEXA scan. Lateral spine X-ray shows 30–40% height loss of L2 and L3 vertebral bodies. What is the diagnosis and immediate management priority?
Analysis: Acute vertebral compression fractures (L2–L3) on a background of glucocorticoid-induced osteoporosis. Prednisolone ≥5 mg/day for ≥3 months is an indication for bone protection therapy regardless of DEXA score — this was not provided (a prescribing error). Immediate management: (1) DEXA scan to characterise BMD (though fractures are definitive evidence of severe disease — T-score ≤−2.5 almost certain); (2) start antiresorptive therapy immediately — alendronate 70 mg weekly or, in view of the severity, zoledronic acid 5 mg IV annually with calcium 1000 mg/day and vitamin D 1000 IU/day; (3) analgesia (paracetamol ± short-term weak opioid — avoid NSAIDs in RA on steroids — double GI/renal hazard); (4) physiotherapy for spinal muscles and fall risk reduction. Vertebroplasty: not indicated for this acute presentation (conservative management first 4–6 weeks).
Scenario B: Mr Mohan, 80 years old, has bilateral knee pain limiting stair-climbing (IADL impaired). He rates his pain 7/10. X-ray shows severe joint space narrowing, osteophytes, and subchondral sclerosis bilaterally. His BMI is 34 (obese). He is currently on ibuprofen 400 mg TDS (three daily) plus omeprazole, prescribed for 'years'. eGFR is 48 mL/min. CRP and ESR are normal. What modifications to his management are required?
Analysis: Severe bilateral knee OA on a background of obesity, with chronic NSAID use that is hazardous given eGFR 48 (NSAIDs further impair renal perfusion in CKD — a STOPP criterion). Management changes: (1) stop ibuprofen — NSAID contraindicated in CKD (eGFR <50); (2) switch to topical diclofenac gel (local effect, minimal systemic absorption) plus paracetamol 1 g TDS; (3) consider intra-articular methylprednisolone for short-term relief; (4) intensive weight management — 5% weight loss will provide clinically meaningful pain reduction (the most effective OA intervention in the obese patient); (5) physiotherapy referral for quadriceps strengthening; (6) refer for orthopaedic assessment for total knee replacement given severe bilateral disease and functional impairment despite conservative management. Do not delay TKR on the basis of age alone.
Scenario C: Mrs Sulochana, 82 years old, is admitted after her third fall in 6 months. She lives alone in a single-room apartment. She uses a walking stick. Her TUG test is 18 seconds. Her medications: metoprolol, amlodipine, lorazepam (benzodiazepine) nightly, mirtazapine (alpha-2 antagonist antidepressant). MMSE 24. BP lying 148/86, standing 128/72. What is the priority falls prevention plan?
Analysis: Multiple modifiable risk factors identified: (1) Lorazepam — the highest priority: a benzodiazepine that causes next-morning sedation, balance impairment, and falls; gradual taper and stop (not abrupt cessation — withdrawal risk); (2) Orthostatic hypotension — present (20 mmHg systolic drop on standing); review antihypertensives (reduce amlodipine if tolerated); (3) TUG 18 sec — significant fall risk; refer to physiotherapy for balance and gait training (Otago programme); (4) Vision assessment — check for uncorrected visual impairment; (5) Home occupational therapy assessment — grab bars in bathroom, non-slip mat, improved lighting; (6) Vitamin D level — supplement if deficient; (7) Social isolation — consider day programme and social support referral. Note: mirtazapine should be reviewed as sedating antidepressant (less falls risk than TCA or benzodiazepine but still sedating at higher doses).
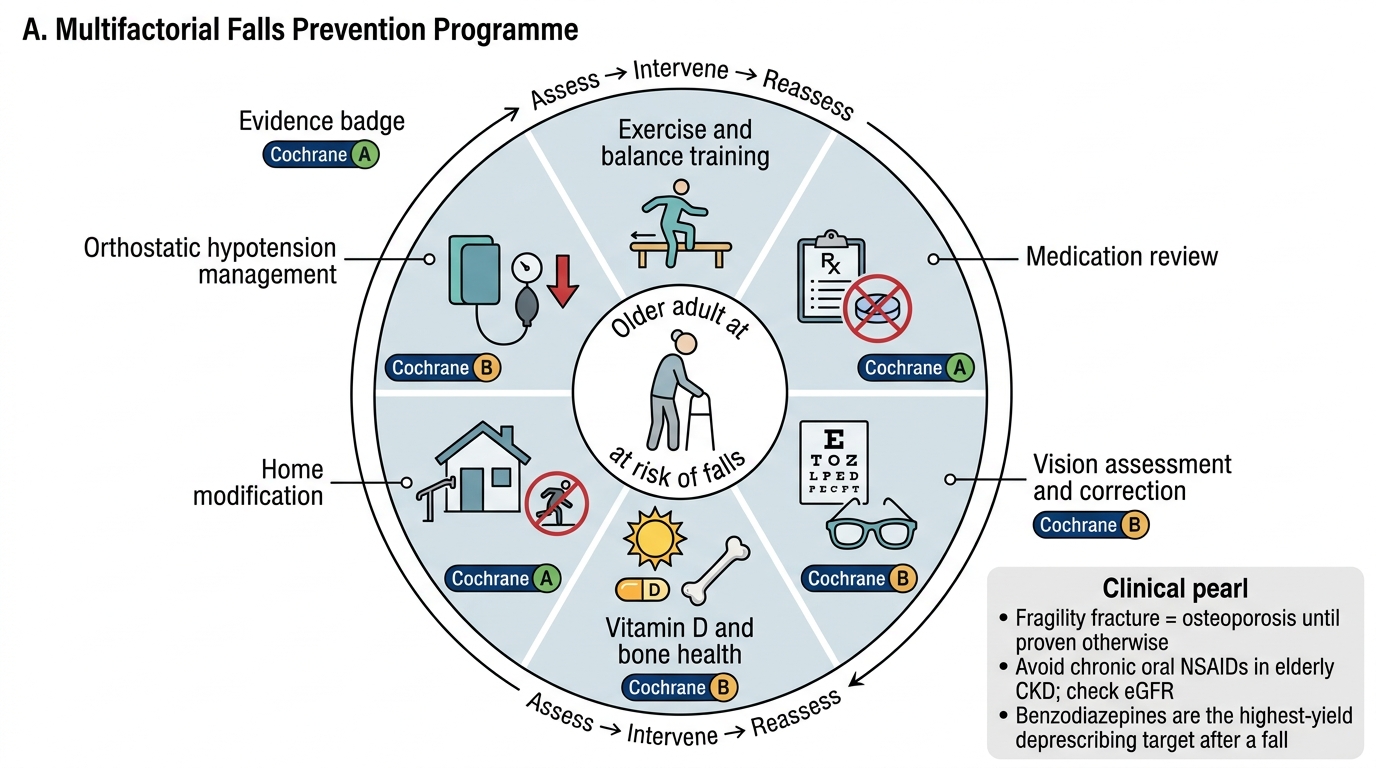
Multifactorial Falls Prevention Programme
CLINICAL PEARL
Three high-yield clinical rules for musculoskeletal geriatrics: (1) A fragility fracture — any fracture from a fall from standing height or less — is osteoporosis until proven otherwise, and requires bone-protective treatment regardless of prior DEXA. Do not wait for a second hip fracture before prescribing bisphosphonates. (2) Chronic NSAID use in elderly patients with CKD is a STOPP criterion — it is not safe, and topical NSAIDs achieve local anti-inflammatory effect with negligible systemic absorption. In any elderly patient with chronic pain on oral NSAIDs, check eGFR and consider switching. (3) Benzodiazepines are the highest-risk single medication class for falls in the elderly. When reviewing the medication list of a patient who has fallen, reach for the benzodiazepine first — it is the highest-yield deprescribing target.