Page 26 of 32
IM25.22 | Geriatric Nutritional Disorders — SDL Guide (Part 2)
Complications of Nutritional Disorders in the Elderly
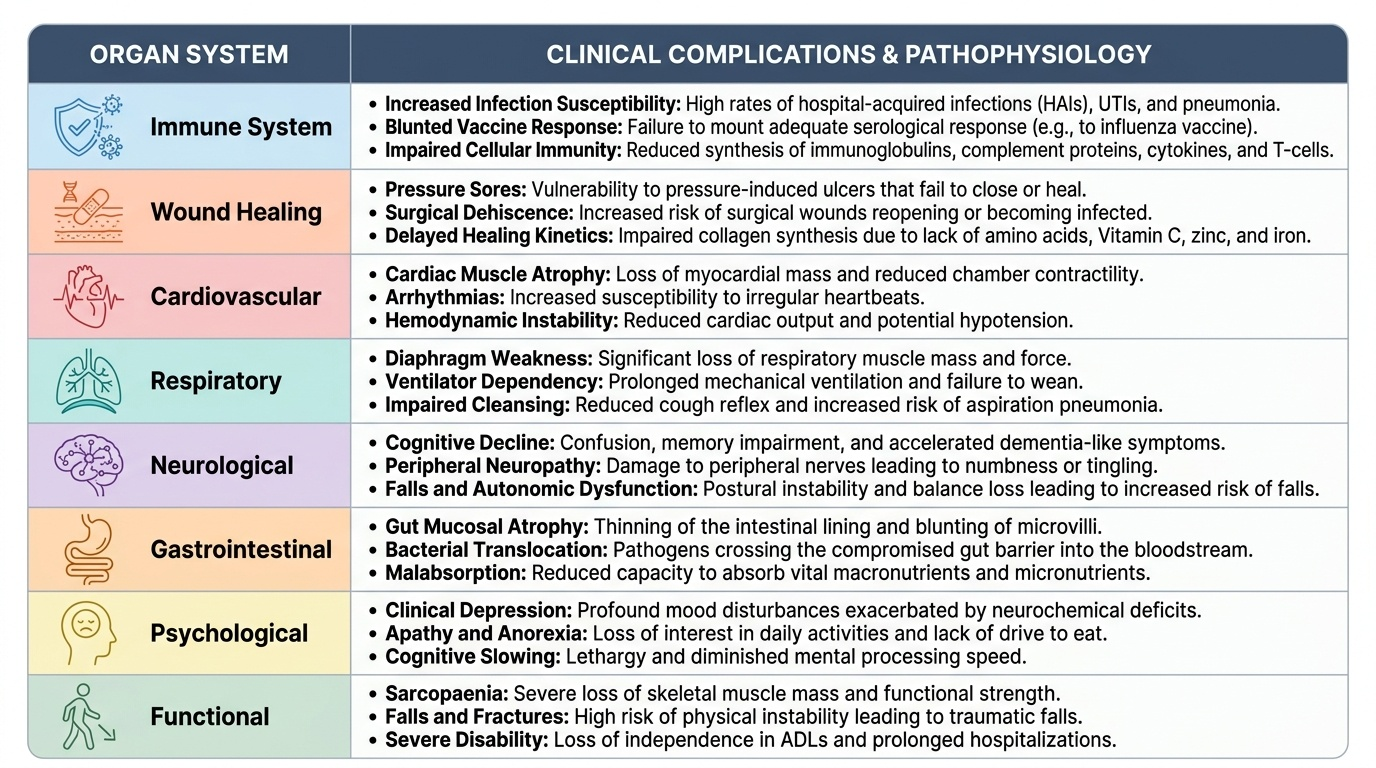
The complications of nutritional disorders in elderly patients span multiple organ systems and compound every concurrent illness. Understanding these complications is not merely a list-memorisation exercise — it provides the clinical rationale for proactive nutritional screening and intervention. Malnutrition is not a passive background state; it is an active pathophysiological process that worsens outcomes across every disease managed in a geriatric ward. The clinician who treats the pneumonia but ignores the malnutrition has addressed only part of the clinical problem.
Provided image
Impaired immune function is among the most clinically consequential complications. Protein deficiency impairs synthesis of immunoglobulins, complement proteins, cytokines, and lymphocytes — particularly T-cell mediated immunity. Malnourished elderly patients have higher rates of hospital-acquired infections, urinary tract infections, pneumonia, and surgical site infections. Vaccine responses are blunted — a malnourished elderly patient may fail to mount an adequate serological response to influenza vaccination. Micronutrient deficiencies compound this: zinc deficiency impairs neutrophil function and NK cell activity; vitamin A deficiency disrupts mucosal barrier integrity; vitamin C deficiency impairs neutrophil function and reduces bactericidal activity.
Poor wound healing directly reflects protein and micronutrient deficiency. Collagen synthesis requires adequate protein (amino acids, particularly proline and hydroxyproline), vitamin C (cofactor for prolyl hydroxylase — the enzyme that cross-links collagen), zinc (cofactor for metalloproteinases in tissue remodelling), and iron (oxygen delivery via haemoglobin to the wound). Malnourished elderly patients have pressure sores that fail to close, surgical wounds that dehisce or become infected, and fractures that are slow to unite. In the context of the opening case — Meenakshi awaiting knee replacement — her hypoalbuminaemia predicts a three-to-five-fold increased risk of surgical site infection and wound complications.
Cardiac and respiratory complications are underappreciated. The diaphragm and intercostal muscles are skeletal muscles and are subject to the same sarcopaenic wasting as limb muscles. Malnutrition-associated respiratory muscle weakness can precipitate respiratory failure in a patient with borderline lung function, or prolong mechanical ventilation in an ICU patient. Cardiac muscle atrophy (cardiac cachexia) reduces cardiac output reserve, increasing the risk of heart failure decompensation. Hypomagnesaemia and hypokalaemia from nutritional deficiency predispose to cardiac arrhythmias.
Falls and fractures are powerfully driven by nutritional factors. Vitamin D deficiency causes proximal myopathy (impairs muscle contraction) AND reduces bone mineral density — a dual mechanism that both increases fall risk and reduces the bone's ability to withstand impact. Protein deficiency drives sarcopaenic muscle weakness. The interaction is multiplicative: a malnourished elderly patient with vitamin D deficiency falls more often AND sustains worse fractures when they fall. Hip fractures in the context of malnutrition carry approximately 40% one-year mortality — nutrition is therefore a major determinant of post-fracture prognosis.
Cognitive impairment can be both a cause and a consequence of malnutrition. Vitamin B12 deficiency causes a reversible dementia-like syndrome; thiamine deficiency causes Wernicke's encephalopathy; folate deficiency raises homocysteine (a neurotoxin); protein-energy malnutrition reduces cerebral glucose metabolism. Conversely, dementia impairs the ability to self-feed, request food, and communicate hunger — creating a bidirectional relationship in which malnutrition and cognitive decline accelerate each other.
Refeeding syndrome is a potentially fatal complication of initiating nutritional support (particularly parenteral nutrition) in severely malnourished patients. As carbohydrates are reintroduced, insulin surges drive intracellular uptake of phosphate, potassium, and magnesium, causing severe hypophosphataemia, hypokalaemia, and hypomagnesaemia. Hypophosphataemia below 0.5 mmol/L causes ATP depletion in red cells (haemolysis), muscles (respiratory and cardiac failure), and the nervous system (seizures, delirium). Prevention: start nutritional support at 50% of estimated requirements for the first 48–72 hours; monitor and correct electrolytes daily; supplement thiamine before refeeding.
SELF-CHECK
A 76-year-old man with a BMI of 15.8 kg/m² is started on nasogastric tube feeding at full calculated rate after a 3-week hospitalisation for aspiration pneumonia during which his intake was negligible. On day 2 of feeding, he develops muscle weakness, respiratory distress, and his serum phosphate is 0.38 mmol/L. What is the MOST likely diagnosis?
A. Aspiration pneumonia recurrence
B. Refeeding syndrome
C. Hypercalcaemia from vitamin D supplementation
D. Pulmonary oedema from fluid overload
Reveal Answer
Answer: B. Refeeding syndrome
Refeeding syndrome occurs when severely malnourished patients (as indicated here by very low BMI of 15.8 and prolonged near-zero intake) receive aggressive nutritional support. As carbohydrates are reintroduced, insulin drives intracellular shift of phosphate, potassium, and magnesium. Severe hypophosphataemia (here 0.38 mmol/L, normal 0.8–1.5 mmol/L) is the hallmark and causes ATP depletion, leading to muscle weakness including the respiratory muscles — explaining the respiratory distress. Prevention requires starting feeding at 50% estimated energy requirements for 48–72 hours, supplementing thiamine before refeeding, and monitoring electrolytes daily. Pulmonary oedema and pneumonia are possible differentials but do not explain the hypophosphataemia. The temporal relationship — day 2 of feeding in a severely malnourished patient — clinches refeeding syndrome.
Management of Nutritional Disorders in the Elderly
The management of nutritional disorders in the elderly must be systematic, cause-targeted, and proportionate to the degree of deficiency and the patient's overall clinical status. Three goals govern every management plan: first, correct the primary cause of inadequate nutrition (address dysphagia, treat depression, review polypharmacy, link to food security programmes); second, provide nutritional support at the appropriate level of intensity matched to the severity of deficiency and clinical context; and third, prevent complications of both the deficiency state and of nutritional support itself (particularly refeeding syndrome). Management is not simply about prescribing a supplement — it is a multidisciplinary process involving the physician, dietitian, speech and language therapist, occupational therapist, and social worker.
Step 1 — Address the cause of nutritional deficiency. Before any nutritional support is initiated, the reversible causes should be identified and addressed. A comprehensive medication review using STOPP-START criteria may identify drugs causing anorexia (digoxin toxicity, SSRIs, opioids) or impairing absorption (PPIs, metformin, cholestyramine). Dental referral is indicated for edentulism or poorly fitting dentures. Dysphagia should be evaluated by a speech and language therapist — modified diet textures (IDDSI framework) and thickened liquids reduce aspiration risk while maintaining oral nutrition. Depression should be treated (antidepressants, social support, cognitive behavioural therapy) — improving mood often restores appetite without any nutritional supplement. Diabetic gastroparesis causing early satiety may respond to prokinetics (metoclopramide, domperidone — noting that metoclopramide is Beers-listed for >12 weeks use in elderly).
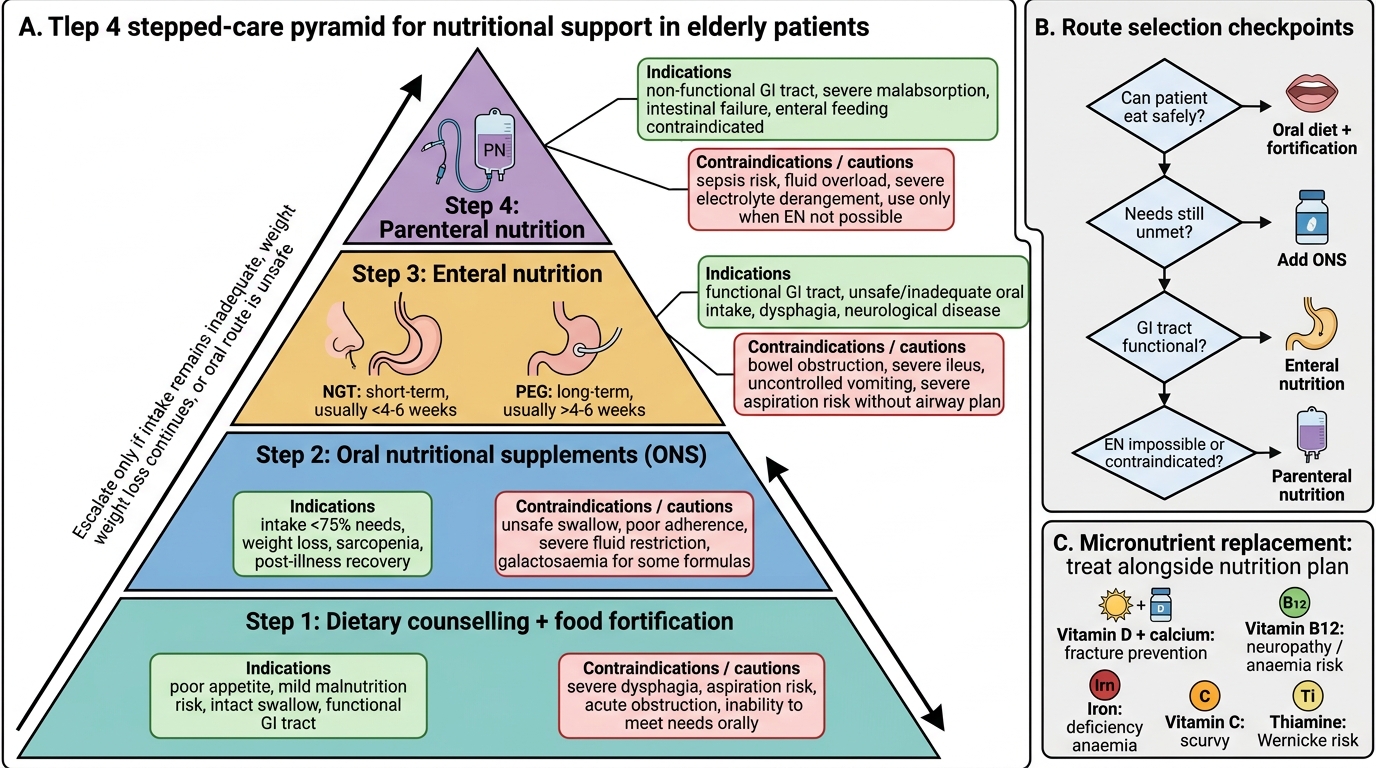
Step 2 — Nutritional support. The level of support is stepped: dietary counselling and food fortification → oral nutritional supplements (ONS) → enteral nutrition (tube feeding) → parenteral nutrition (last resort).
- Dietary counselling and food fortification: enriching regular meals with protein and energy (adding milk powder, eggs, ghee to meals) is the first-line approach for those with mild nutritional risk who can eat normally. Small, frequent, energy-dense meals are better tolerated than three large meals given the early satiety of ageing.
- Oral nutritional supplements (ONS): commercially available protein-energy supplements (e.g., Ensure, Fresubin, Protinex) providing 300–600 kcal/day in addition to regular diet. ESPEN recommends ONS for malnourished elderly patients or those at risk (MNA-SF ≤11). Protein requirements in malnourished elderly: 1.2–1.5 g/kg/day (higher end for those recovering from acute illness or surgery); total energy 25–35 kcal/kg/day. Leucine-enriched ONS may have additional sarcopaenia-specific benefit by lowering the muscle protein synthesis threshold.
- Enteral nutrition (tube feeding): indicated when oral intake is insufficient (<50% of estimated requirements for >3–5 days) despite ONS, and the gut is functional. Nasogastric tube (NGT) is appropriate for short-term use. Percutaneous endoscopic gastrostomy (PEG) is considered for long-term enteral feeding (>4 weeks) in patients with dysphagia (e.g., post-stroke, motor neurone disease). The decision to place a PEG in a patient with advanced dementia is ethically complex and should involve a goals-of-care conversation — evidence does not show that PEG feeding improves survival or quality of life in advanced dementia.
- Parenteral nutrition (PN): reserved for patients with non-functional gut (paralytic ileus, short bowel syndrome, malabsorptive conditions) where enteral nutrition is not possible. Carries risk of line infection, thrombosis, and metabolic complications including refeeding syndrome; use the enteral route whenever the gut is functional.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Stepped Nutritional Support in Elderly Patients
Step 3 — Specific micronutrient replacement:
- Vitamin D: supplement all elderly patients with 800–2000 IU cholecalciferol daily (the upper end for those with documented deficiency or institutionalised elderly with no sun exposure). In deficiency (25-OH-D <20 ng/mL), loading doses of 50,000 IU weekly for 8 weeks may be used, followed by maintenance. Co-administer calcium 1000–1200 mg/day for fracture prevention.
- Vitamin B12: intramuscular hydroxocobalamin 1 mg on alternate days for 2 weeks (total 6–7 injections), then 1 mg every 3 months (life-long if due to atrophic gastritis or pernicious anaemia). Oral high-dose B12 (1000–2000 mcg/day) is an alternative for dietary deficiency where intrinsic factor is intact.
- Iron: oral ferrous sulphate 200 mg three times daily (85 mg elemental iron per dose); take on empty stomach with vitamin C for enhanced absorption. If oral not tolerated or malabsorbed (atrophic gastritis, post-gastrectomy), IV iron (ferric carboxymaltose or iron sucrose) is indicated.
- Vitamin C: 500–1000 mg daily for confirmed scurvy; dietary improvement (fresh fruit and vegetables) for mild deficiency.
- Thiamine: 100 mg IV or IM three times daily for suspected Wernicke's (do not wait for confirmation — give empirically to any confused, ataxic, or malnourished elderly patient before glucose or nutritional support).
- Zinc: 30–45 mg elemental zinc daily for 8–12 weeks for documented deficiency or poor wound healing.
Refeeding precautions: in any patient with severe malnutrition (BMI <16, weight loss >20%, prolonged minimal intake >5 days), start nutritional support at 10 kcal/kg/day and increase slowly over 4–7 days to target; supplement thiamine 200–300 mg IV daily for the first 10 days; supplement phosphate, potassium, and magnesium; monitor electrolytes daily for the first week.
Exercise and physical activity are inseparable from nutritional management of sarcopaenia. Resistance exercise (progressive resistance training — squats, leg press, arm curls against resistance) is the most effective intervention for maintaining and increasing muscle mass and strength — more effective than nutrition alone. Nutrition and exercise have synergistic effects: providing protein immediately before or after resistance exercise maximises the anabolic stimulus. The prescription for sarcopaenic elderly patients is protein 1.2–1.5 g/kg/day + supervised resistance training 2–3 times per week.
Self-Assessment: Integrating Nutritional Assessment and Management
The self-assessment section of this module asks you to apply the full arc of geriatric nutritional medicine — from recognising the clinical presentation and understanding the aetiopathogenesis, through systematic assessment, to appropriate management — across clinical scenarios drawn from realistic Indian hospital and community settings. For each scenario, work through the clinical reasoning before reading the analysis. The aim is not merely to recall facts but to demonstrate the KH-level clinical reasoning that the IM25.22 competency requires: seeing the nutritional diagnosis behind the presenting complaint, connecting the mechanism to the finding, and selecting appropriate investigations and interventions. In each scenario, there is a specific 'trap' — a feature that a less careful clinician would attribute to ageing, to the primary diagnosis, or to incidental findings rather than to an underlying nutritional disorder. Recognising these traps is the core competency this section develops, and it is the same skill that separates an excellent geriatrician from an adequate one in clinical practice.
Provided image
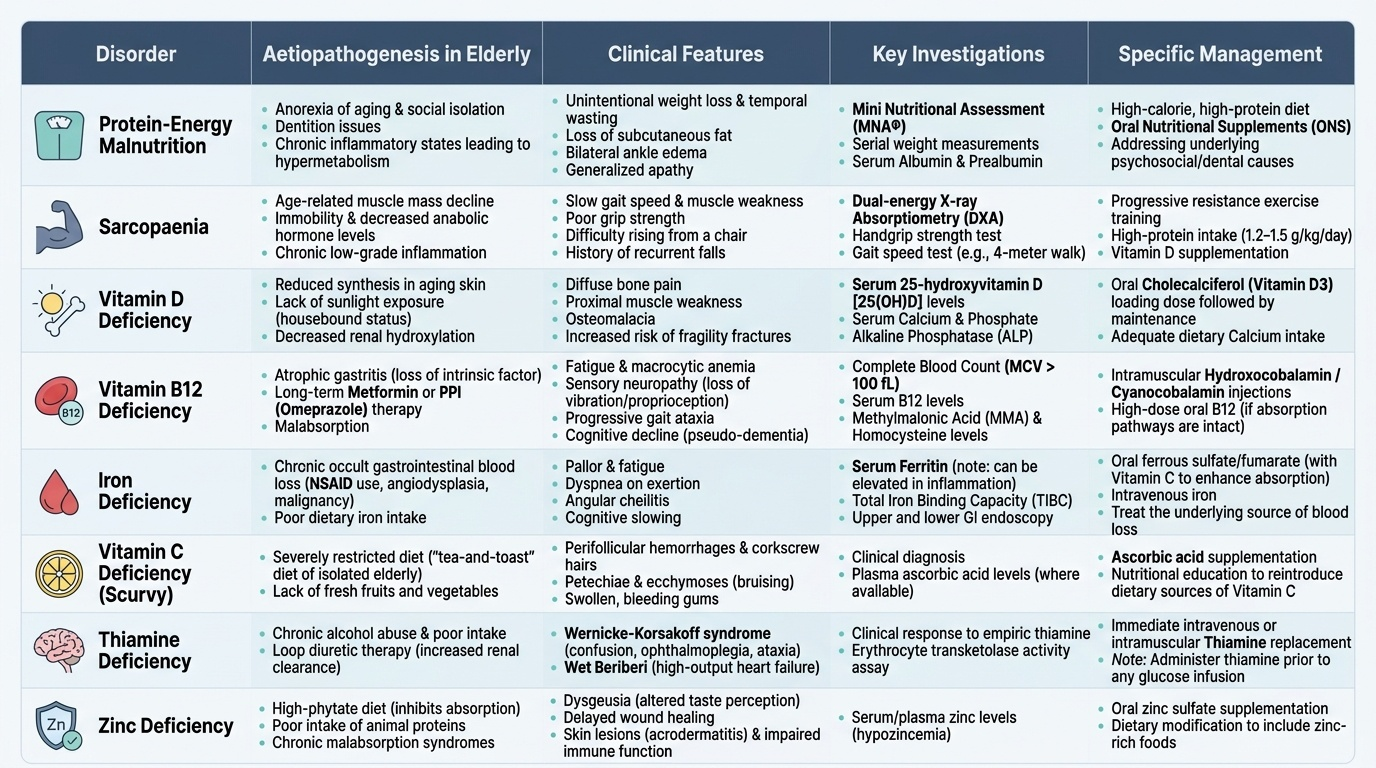
Scenario A: A 77-year-old man on omeprazole (for GERD) and metformin (for type 2 diabetes) for 10 years presents with fatigue, memory problems, and a slowly progressive gait disturbance. On examination: MMSE 21/30 (mild impairment), loss of vibration sense to the knee bilaterally, slightly wide-based gait, no weakness. Blood results: Hb 10.8 g/dL, MCV 110 fL, serum B12 48 pg/mL. What is the diagnosis, and what treatment should be given?
Analysis: Low serum B12 (<200 pg/mL, severely low here at 48 pg/mL), macrocytic anaemia (MCV 110), posterior column signs (vibration loss, gait disturbance), and cognitive impairment = vitamin B12 deficiency causing subacute combined degeneration of the spinal cord and reversible cognitive impairment. Two contributing mechanisms: (1) omeprazole-induced achlorhydria reducing gastric acid needed to cleave B12 from food proteins; (2) metformin inhibiting ileal absorption of B12 (intrinsic factor-B12 complex). Treatment: IM hydroxocobalamin 1 mg on alternate days for 2 weeks, then 1 mg every 3 months for life (atrophic gastritis likely given PPI use — oral B12 would also be poorly absorbed). Neurological improvement may take months and may be incomplete if deficiency was prolonged. Monitor for improvement in MMSE at 3 months.
Scenario B: A 72-year-old woman with rheumatoid arthritis is referred for pre-operative nutritional assessment before hip replacement surgery. MNA-SF = 8 (at risk). BMI 18.6 kg/m². Weight loss 5.5 kg in 6 months (8% of body weight). MAC 20 cm. She reports eating one small meal per day. Serum albumin 2.9 g/dL; CRP 44 mg/L. What would you recommend?
Analysis: Multiple indicators of malnutrition — MNA-SF in 'at risk' zone, low BMI, significant recent weight loss (>5% in 6 months), low MAC, low albumin (partially confounded by RA-associated chronic inflammation). Surgery should be deferred for at least 2–4 weeks of pre-operative nutritional rehabilitation. Initiate ONS (300–600 kcal/day additional) on top of dietary counselling. Target protein 1.2–1.5 g/kg/day. If she cannot achieve this orally, nasogastric feeding for 10–14 days pre-operatively is indicated (ESPEN recommends 7–14 days' pre-operative nutritional support for severely malnourished surgical patients). Also check vitamin D, B12, iron, folate — RA patients on methotrexate are at risk of folate deficiency; anti-inflammatory treatment may improve appetite by reducing disease activity.
Scenario C: An 84-year-old man presents with bleeding gums, painful legs, and petechial haemorrhages concentrated around hair follicles. He lives alone and states he has not eaten fresh food in months because he cannot go to the market. His diet consists of biscuits and tea. What is the diagnosis and management?
Analysis: Scurvy — perifollicular haemorrhages (pathognomonic: corkscrew hairs with surrounding petechiae), gingival bleeding, and leg pain (subperiosteal haemorrhage) in the context of prolonged dietary deficiency of fresh fruit and vegetables. Diagnose clinically (serum vitamin C can confirm if needed). Treat with vitamin C 500–1000 mg/day orally for 4 weeks, then dietary supplementation with fresh fruits and vegetables. Address the social root cause — domiciliary food service referral, ASHA community follow-up, social work assessment for support with shopping and meal preparation. Symptoms typically resolve within 1–2 weeks of treatment.
CLINICAL PEARL
Thiamine before glucose — always. Any elderly patient presenting with confusion, ataxia, or ophthalmoplegia in the context of poor nutritional intake must receive intravenous thiamine (200–300 mg IV, diluted in normal saline) BEFORE any glucose-containing fluid or nutritional support is administered. Giving glucose first in a thiamine-deficient patient can precipitate or worsen Wernicke's encephalopathy by driving thiamine-dependent metabolic pathways in an already-depleted state. This is especially important for malnourished elderly patients admitted through the emergency department, where glucose-containing IV fluids are often started reflexively.
A second pearl: serum albumin reflects illness severity, not just nutrition. A low albumin in an acutely ill elderly patient (e.g., pneumonia, sepsis, surgery) is largely an acute-phase response — albumin is a negative acute-phase reactant and its synthesis is downregulated by IL-6 and TNF-α. This does not mean the patient is well-nourished; it means albumin alone is insufficient to make that determination. Use MNA-SF, weight history, and dietary intake alongside albumin — the combination is both more accurate and more clinically actionable.