Page 20 of 32
IM25.16 | Geriatric Rehabilitation — SDL Guide (Part 2)
Interpreting Rehabilitation Outcomes and Addressing Barriers
Rehabilitation outcomes in the elderly must be interpreted within the context of: the severity of the underlying impairment (infarct size in stroke, fracture type and surgical approach in hip fracture), pre-morbid functional status (the rehabilitation goal is to return the patient to their pre-illness baseline or as close as possible — not to achieve a normative standard for age), comorbidities that limit participation (pain, cardiac/respiratory limitation, depression, cognitive impairment), and time elapsed since onset of illness. The concept of the rehabilitation potential is central: identifying which patients are most likely to benefit from intensive inpatient rehabilitation versus those whose limited potential makes a different care trajectory more appropriate.
Provided image
Predicting rehabilitation outcomes in stroke: The NIHSS (National Institutes of Health Stroke Scale — 0–42, measures stroke severity across 11 domains including consciousness, gaze, visual field, facial palsy, motor limb, ataxia, sensory, language, dysarthria, neglect) is the strongest predictor of rehabilitation potential. NIHSS ≤8 at 72 hours post-stroke is associated with favourable outcome; NIHSS >25 predicts poor 90-day outcome. Pre-stroke mRS (functional status before the current event) is equally important — a patient who was already dependent (mRS 4) before a mild stroke has much lower absolute recovery potential than a fully independent person (pre-stroke mRS 0–1) with the same stroke severity. The NIHSS + pre-stroke mRS composite is used clinically to guide rehabilitation intensity.
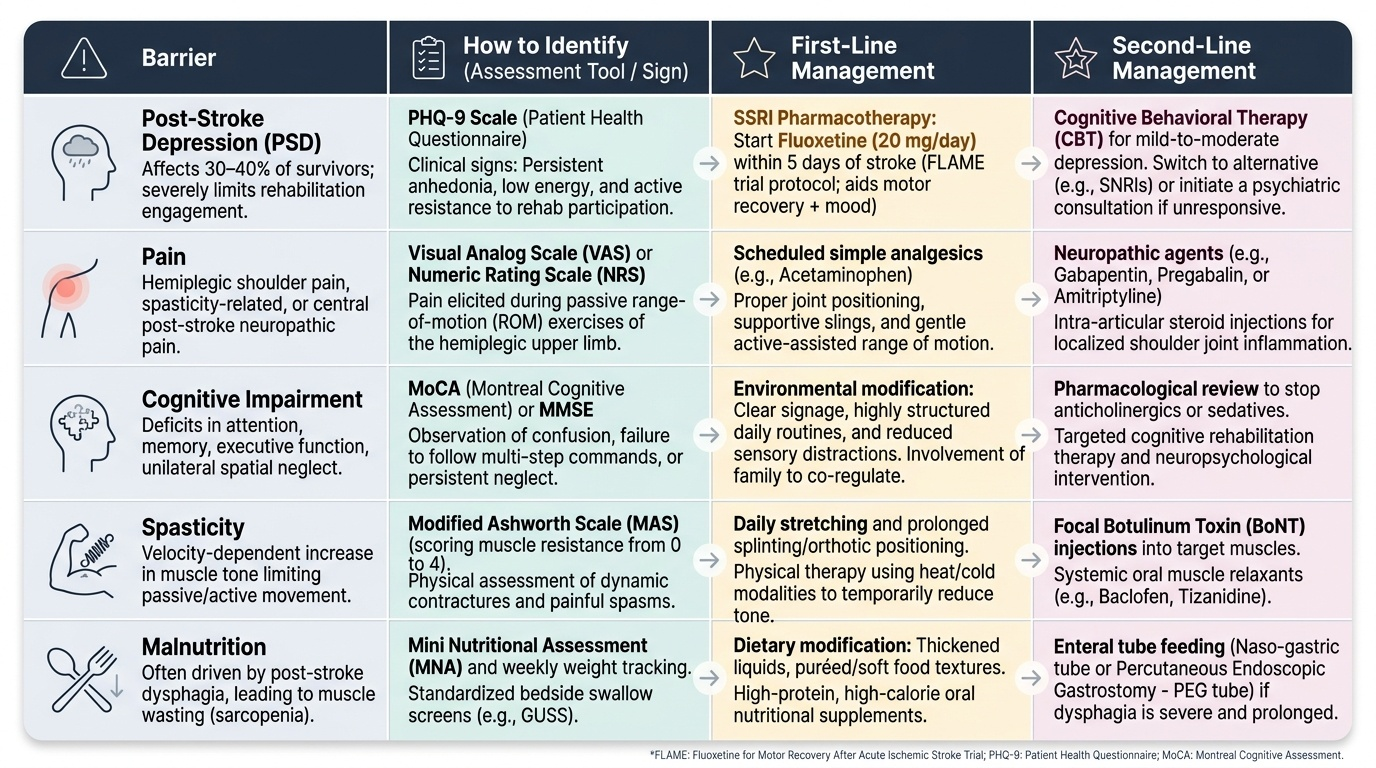
Barriers to rehabilitation and how to address them: Several factors can undermine rehabilitation progress and must be actively identified and treated:
- Post-stroke depression (PSD): Affects 30–40% of stroke survivors; characterised by depressed mood, anhedonia, energy loss, and — critically — poor rehabilitation engagement. PSD is an independent predictor of worse rehabilitation outcome. Treatment: SSRI (fluoxetine has evidence specifically in PSD from FLAME trial — 20 mg/day started within 5 days of stroke; also evidence for motor recovery, not just mood); CBT for mild-moderate PSD.
- Pain: Inadequately treated pain reduces physiotherapy participation and motivation. Common causes in elderly rehabilitation patients: shoulder pain in stroke (hemiplegic shoulder pain from subluxation or improper positioning), nociceptive pain from arthroplasty incision, neuropathic pain from stroke (central post-stroke pain, diencephalic origin — burning, allodynia, extremely difficult to treat — gabapentin/amitriptyline).
- Cognitive impairment: Post-stroke cognitive impairment (PCI) occurs in up to 60% of stroke survivors; dementia doubles falls during rehabilitation. Strategy: repetition-based learning (procedural memory is relatively preserved in mild dementia), consistent staff, visual cues, errorless learning principles.
- Spasticity: Post-stroke spasticity develops weeks to months after the acute event; produces painful muscle stiffness, contracture risk, hygiene difficulties (clenched fist), and impaired positioning. Management: physiotherapy (stretching, splinting, positioning); botulinum toxin type A injections (botox) to specific spastic muscles (the most effective focal treatment — reduces tone, improves passive range, facilitates physiotherapy; the effect lasts 12–16 weeks and can be repeated); baclofen (oral, central muscle relaxant — limited evidence in spasticity post-stroke; significant sedation in elderly — STOPP consideration); baclofen intrathecal pump for severe generalised spasticity.
- Nutritional deficiency: Malnutrition in the rehabilitation patient (common in stroke — dysphagia, depression, reduced appetite) delays wound healing, impairs muscle synthesis for strength recovery, and increases infection risk. Dietitian input for appropriate texture-modified diet (for dysphagia) and caloric/protein supplementation.
Social rehabilitation extends the recovery from the hospital to the community. Components: community physiotherapy (continuing exercise programme after discharge — evidence shows gains are lost within 6 months if community rehabilitation ceases); day hospitals (attend 3–5 times per week for structured rehabilitation — alternative to prolonged inpatient stay, provides therapy while living at home); community occupational therapy (home modification follow-up, community skills training — using public transport, shopping); stroke support groups (peer support, information sharing, community reintegration — Stroke Association India; ARDSI — Alzheimer's and Related Disorders Society of India for dementia rehabilitation); carer training and education (family members as co-therapists in community rehabilitation; carer health monitoring for burnout).
SELF-CHECK
A 68-year-old woman with right MCA stroke (NIHSS 12 on admission, now 8 at day 7) is in the inpatient stroke rehabilitation unit. Her physiotherapist reports that she engages poorly in sessions, is often tearful, and states 'what's the point — I'll never be the same.' Her Barthel Index has not improved from 35 over the past 8 days. Which intervention should the physician prioritise?
A. Increase physiotherapy session intensity to twice daily — rehabilitation dose is the primary determinant of outcome
B. Discharge to nursing home — failure to progress by day 7 indicates poor rehabilitation potential
C. Screen formally for post-stroke depression (PHQ-9 or GDS) and initiate SSRI therapy (fluoxetine 20 mg) alongside ongoing rehabilitation
D. Arrange CT brain to exclude haemorrhagic transformation causing the behavioural change
Reveal Answer
Answer: C. Screen formally for post-stroke depression (PHQ-9 or GDS) and initiate SSRI therapy (fluoxetine 20 mg) alongside ongoing rehabilitation
The clinical picture — tearfulness, anhedonia ('what's the point'), withdrawal from rehabilitation engagement, and plateau in functional progress — is a classic presentation of post-stroke depression (PSD), which affects 30–40% of stroke survivors. PSD is an independent barrier to rehabilitation participation and outcome. The FLAME trial demonstrated that fluoxetine 20 mg started within 5 days of stroke improves both mood and motor recovery. The immediate action: formal depression screening (GDS or PHQ-9) to confirm diagnosis, then initiate SSRI. Simply increasing physiotherapy dose without addressing the depression will have limited effect. Discharge at day 7 plateau is premature — the barrier must be identified and treated first. CT brain is not indicated without new focal neurological signs.
Applied Practice: Rehabilitation Across Clinical Contexts
The rehabilitation framework applies across the clinical contexts most common in geriatric medicine. The scenarios below test your ability to prescribe a rehabilitation plan with the specificity that a real MDT referral requires — not 'please do rehabilitation' but a defined set of goals, team members, functional targets, timeline, and discharge criteria.
Context 1 — Post-stroke rehabilitation: Murugadoss (from the hook), day 5 post-right MCA stroke, left hemiparesis (MRC 2/3), aphasia (improving), dysphagia (thickened fluids). Rehabilitation prescription: (a) Physiotherapy: daily sessions, goal — safe bed-to-chair transfer by day 10, standing with Zimmer frame by day 14, progress to 10-metre walk with tripod by day 21; CIMT contraindicated (too early — arm MRC 2); positioning programme for subluxation prevention; (b) Occupational therapy: ADL assessment; one-handed dressing training; identify home modifications required (patient lives with wife in first-floor flat with stairs); (c) Speech and language therapy: daily dysphagia management, texture-modified diet, family education for safe feeding; aphasia communication strategies; (d) Psychology: post-stroke depression monitoring (GDS at day 7 and weekly); (e) Social work: home visit arranged, carer assessment of wife's capacity to support. Outcome measure: Barthel Index weekly; mRS at 3 months.
Context 2 — Post-hip fracture rehabilitation: Mrs Padma, 82 years old, day 3 post-hemiarthroplasty for displaced subcapital fracture. CFS 5 (mildly frail). Pre-fracture: lived alone, walking with stick. Rehabilitation prescription: (a) Physiotherapy: stand at bedside day 1, transfer to chair day 2 ✓ already done; goal — 10-metre indoor walk with Zimmer frame by day 7; progress to outdoor walk with stick by day 14; hip precautions (no flexion >90°, no internal rotation/adduction — posterior approach); fall prevention programme; (b) Occupational therapy: ADL assessment with hip precautions in mind; raised toilet seat, shower chair, grabbing rail for home; home visit before discharge (patient lives alone — essential); assess kitchen and bedroom safety; (c) Nutrition: high-protein diet, vitamin D 1000 IU; caloric supplement if intake low; (d) VTE prophylaxis: LMWH continued for 28 days; (e) Osteoporosis: zoledronic acid IV before discharge; (f) Discharge planning: decision between home (with community OT and physio follow-up) vs interim residential rehabilitation unit. Barthel Index weekly target: ≥60 by day 14 for home discharge with community support.
Context 3 — Frailty and deconditioning: Mr Periasamy, 77 years old, admitted for pneumonia, now medically recovered. Pre-admission: walking with difficulty, socially isolated. CFS 6 (moderately frail). Barthel 55. Rehabilitation goals: (a) Physiotherapy: progressive ambulation programme — Otago exercises (seated leg exercises → standing exercises → walk practice); aim: TUG <14 seconds before discharge; (b) Occupational therapy: ADL assessment, fall risk assessment, home modification recommendations; (c) Social work: assessment for home care package (personal care assistant for bathing, meals), day centre referral to maintain socialisation and physical activity after discharge; (d) Depression screening: GDS (social isolation + frailty = high risk); (e) Medication review (STOPP): identify and deprescribe sedatives, anticholinergics, fall-risk medications. Discharge criterion: safe ambulation indoors; functional support in place at home; family or carer briefed on escalation signs.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
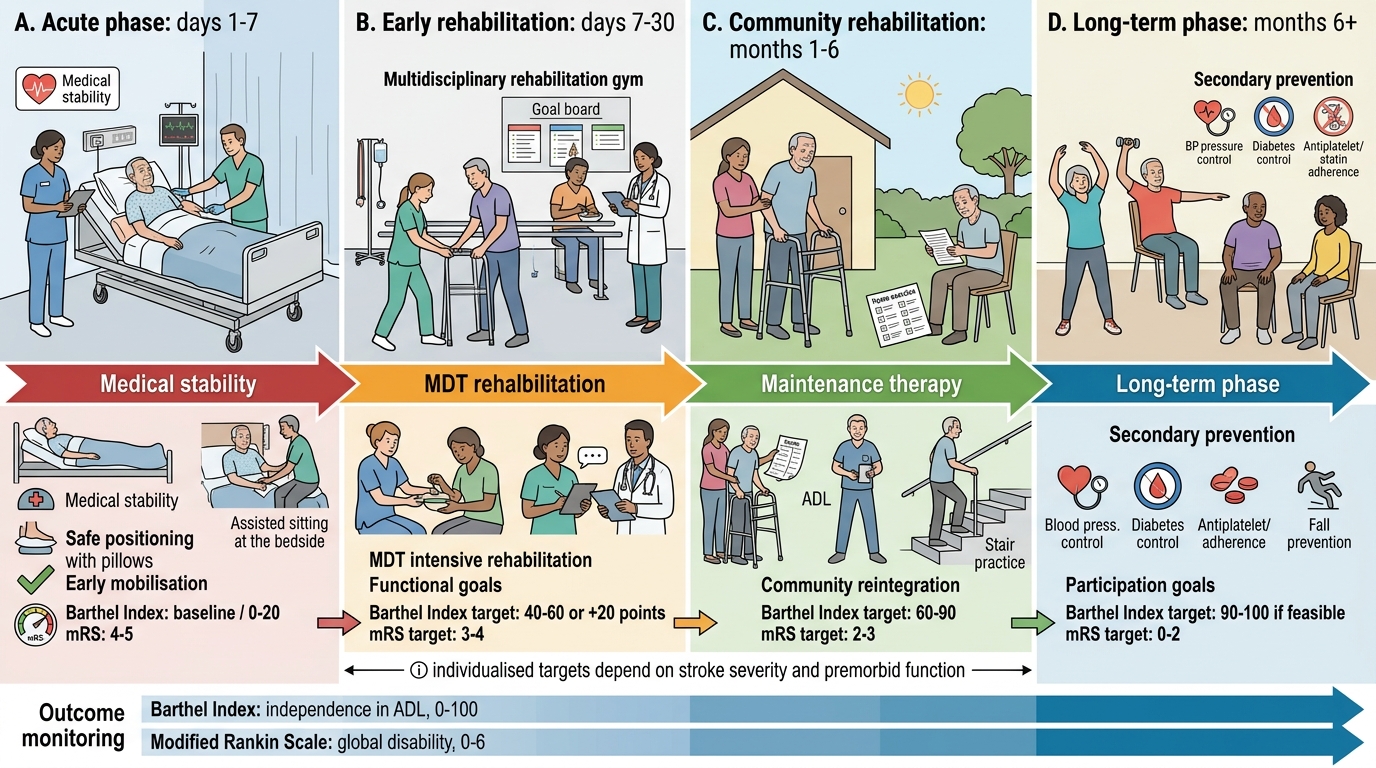
Post-Stroke Rehabilitation Timeline and Outcome Targets
Self-Assessment: Rehabilitation Planning and Monitoring
The following self-assessment scenarios require you to integrate the skills arc: indication and principles → functional assessment → physiotherapy and OT roles → outcome interpretation and barrier management → applied clinical plans. These reflect the NMC KH-level requirement for rehabilitation competency.
Scenario A: Mr Kumar, 73 years old, is 6 weeks post-total knee replacement. He was fully independent before surgery (Barthel 100). He is now at home, attending outpatient physiotherapy twice weekly, but reports that his knee is painful during exercises and he is struggling to comply with the home exercise programme. His wife says he seems low in mood since the operation. Barthel Index at 6 weeks: 75/100 (mainly limited by stair-climbing and outdoor mobility). What are the priority actions?
Analysis: (1) Pain management: inadequate analgesia is the primary barrier to physiotherapy participation; review analgesic regimen (topical diclofenac gel for local anti-inflammatory; paracetamol 1 g QDS; intra-articular corticosteroid injection if significant inflammatory component); rule out post-operative wound/periprosthetic joint infection (examine wound, CRP, WCC); (2) Post-operative depression: screen with GDS/PHQ-9 (onset post-major surgery, functionally able but low mood = risk); SSRI if confirmed; (3) Physiotherapy review: discuss compliance barriers with physiotherapist; home exercise programme simplification and written instruction may improve adherence; (4) Goal review: is the Barthel target of 100 at 12 weeks realistic given current trajectory? — a shared goal-setting conversation with the patient.
Scenario B: Mrs Janaki, 82 years old, has had two falls in hospital during her admission for atrial fibrillation rate control. She is frail (CFS 5), has mild dementia (MMSE 22), and moderate osteoporosis. Her Barthel Index on admission was 65. The consultant asks for an occupational therapy assessment and physiotherapy review. What specific outputs would the physician expect from each?
Analysis: Physiotherapy outputs: TUG test (baseline fall risk quantification); gait analysis (identify specific impairments — balance deficits, muscle weakness, gait pattern); falls risk factors analysis (muscle weakness, balance impairment, antalgic gait from OA); short-term goal prescription (safe mobility on the ward); long-term plan (Otago exercise programme for community discharge). Occupational therapy outputs: ADL assessment at baseline and goals for safe discharge; cognitive-perceptual assessment (MMSE 22 — assess apraxia, visuospatial neglect, executive function barriers to safe ADL); home environment pre-assessment (from patient and family history — identify kitchen, bathroom, and external access hazards); assistive device recommendations (raised toilet seat, grab rails, bath seat or shower if bath hazardous, non-slip bath mat); family/carer briefing for fall prevention at home.
Scenario C: Critically evaluate the following rehabilitation plan written by a house officer: 'Mr Rajan, 68, post-stroke day 10. Please physio and OT. Discharge when better.' What are the deficiencies in this plan and what would an adequate plan contain?
Analysis: Deficiencies: (1) No NIHSS or Barthel to define baseline function; (2) No specific physiotherapy goals (what mobility target, in what timeframe?); (3) No OT goals specified (ADL retraining, home assessment?); (4) No SLT referral (post-stroke aphasia/dysphagia must always be screened — this patient had aphasia); (5) No depression screening plan; (6) No functional discharge criterion (what Barthel or TUG score triggers safe discharge?); (7) 'Discharge when better' is not a criterion — 'better' is unmeasurable. Adequate plan would include: NIHSS documented; Barthel Index at baseline; specific referrals to all relevant MDT members with clinical justification; short-term functional goals (transfer by day X, walking by day Y); outcome measures to be repeated weekly; discharge criterion (Barthel ≥60 with home care package in place); post-discharge follow-up plan (community physiotherapy, stroke clinic at 6 weeks, mRS at 3 months).
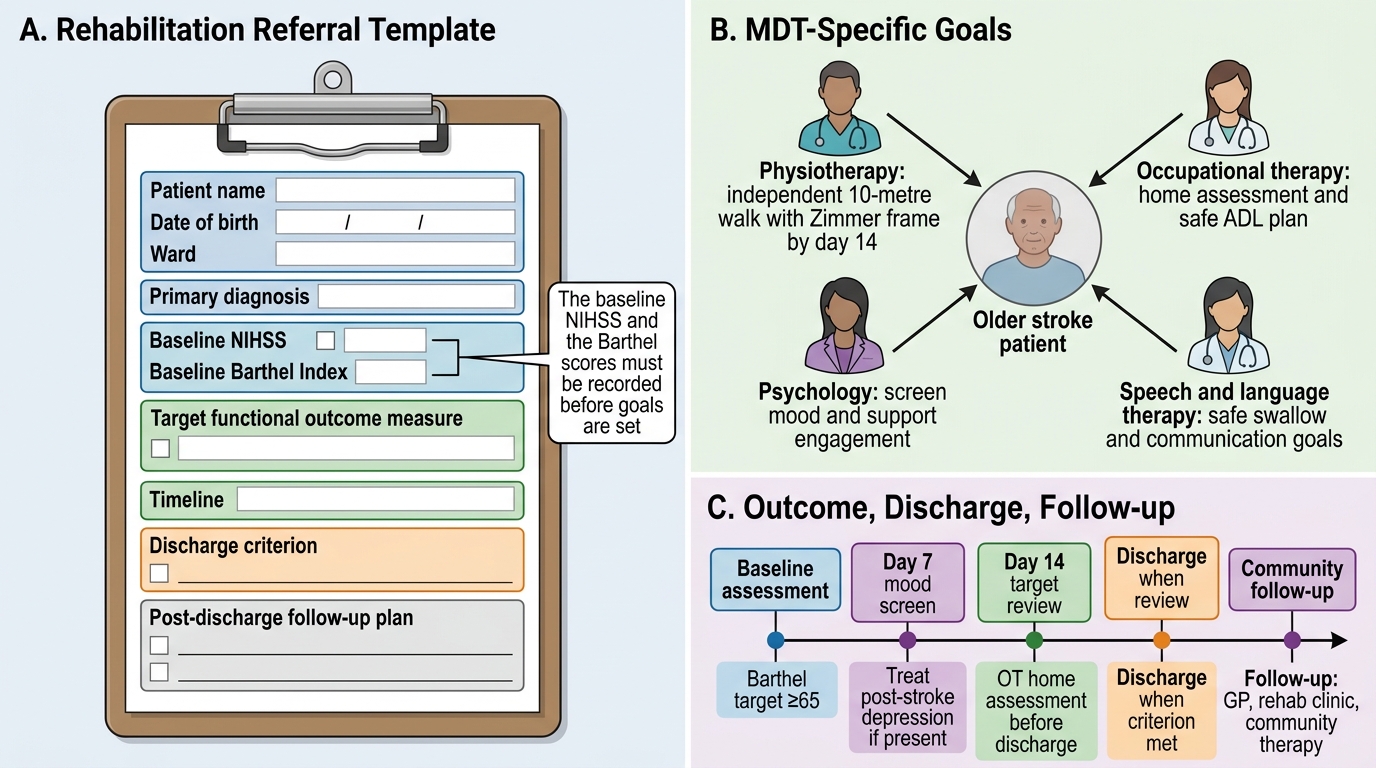
Structured Geriatric Rehabilitation Referral Template
CLINICAL PEARL
Three pearls that define expert-level geriatric rehabilitation practice: (1) A rehabilitation plan must have a specific, measurable, patient-valued goal. 'Please rehabilitate' is not a plan; 'Goal: independent 10-metre walk with Zimmer frame by day 14, to enable return home to wife, Barthel target ≥65' is a plan. Goal specificity drives team motivation, patient engagement, and resource justification. (2) Post-stroke depression is a treatable cause of rehabilitation failure — screen for it actively at day 7 and treat it promptly. Tearfulness and lack of engagement in a stroke patient are not 'expected reactions to disability' — they may represent depression that responds rapidly to SSRI treatment and transforms rehabilitation participation. (3) The occupational therapist's home assessment is among the highest-value geriatric interventions — it prevents re-hospitalisation from falls and enables safe independent living. Never discharge a frail elderly patient from a new disability without an OT home assessment. The 30-minute OT visit can prevent a 30-day readmission.