Page 16 of 32
IM25.{15,17} | Geriatric Sensory Loss — SDL Guide
Learning Objectives
- Describe the pathophysiology and clinical features of the four major age-related vision disorders: cataract, AMD, glaucoma, and diabetic retinopathy
- Perform a basic visual assessment including Snellen acuity, confrontation fields, direct ophthalmoscopy, and refer appropriately
- Describe the pathophysiology of presbycusis and distinguish it from other causes of hearing loss using Rinne and Weber tuning fork tests
- Interpret a pure-tone audiogram and identify the audiological patterns of presbycusis and noise-induced hearing loss
- Enumerate the functional consequences of untreated sensory loss in the elderly including falls, cognitive decline, and depression
- Prescribe appropriate interventions for visual and hearing impairment including surgery, anti-VEGF, hearing aids, and low-vision rehabilitation
INSTRUCTIONS
Sensory loss is ubiquitous in the elderly and profoundly affects every dimension of function, safety, and quality of life. This module addresses vision and hearing impairment together, reflecting their frequent co-occurrence and shared impact on falls, cognition, and social participation. The central clinical lesson is that most sensory impairment in elderly Indians is treatable — cataract is surgically curable, hearing aids restore communication — and untreated sensory loss is a driver of dementia, not a consequence of it.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chs 34–36 — Disorders of Vision and Hearing (textbook)
- API Textbook of Medicine, 11th ed., Chapter on Geriatric Sensory Impairment (textbook)
- Lancet Commission on Dementia Prevention, Intervention and Care, 2020 and 2024 update (guideline)
- National Programme for Control of Blindness and Visual Impairment (NPCB+VI), India — operational guidelines (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Saradha, 78 years old, lives alone in a small apartment. Her daughter visits monthly and notices that the television volume has been turned up progressively louder over the past two years. During the visit, she notices her mother does not respond when spoken to from another room, has several small unnoticed cuts on her fingers from cooking, and recently stopped attending her weekly bhajan group 'because the singing sounds distorted.' Her ophthalmologist found moderate cataracts and macular degeneration six months ago, and prescribed glasses, but Saradha says she stopped wearing them 'because they don't help much anymore.' She stopped going out of the house last month after she tripped on the stairs because she misjudged a step. Saradha has not been diagnosed with any life-threatening disease — yet she is becoming progressively isolated, dependent, and at high risk of falls and depression. Sensory loss is among the most prevalent and most treatable causes of functional decline and social isolation in the elderly, and among the most frequently overlooked in routine clinical assessment.
WHY THIS MATTERS
Visual impairment affects approximately 20–30% of Indians over 60 years; of these, the vast majority have treatable or correctable causes (cataract being the most important — surgically curable and freely available under the National Programme for Control of Blindness and Visual Impairment). Hearing loss is even more prevalent: approximately 40–60% of Indians over 60 have clinically significant hearing impairment, predominantly age-related sensorineural hearing loss (presbycusis). Together, visual and hearing impairment are leading drivers of functional dependence, falls, depression, social isolation, and cognitive decline in the elderly. NMC competencies IM25.15 and IM25.17 require KH-level understanding of both conditions — their pathophysiology, clinical identification, functional consequences, and the management that can restore function.
RECALL
Recall the anatomy relevant to these sensory systems. Visual pathway: light → cornea → lens (refraction) → retina (photoreceptors: rods for peripheral/low-light vision; cones for central/colour vision) → optic nerve → optic chiasm → optic tract → lateral geniculate nucleus → visual cortex (occipital lobe). The macula is the central retinal region containing the highest density of cones — responsible for fine central vision and reading. The aqueous humour is produced by the ciliary body and drains through the trabecular meshwork — imbalance causes intraocular pressure (IOP) elevation. Auditory pathway: sound → external auditory canal → tympanic membrane → ossicles (malleus, incus, stapes) → oval window → cochlea (hair cells in the organ of Corti) → auditory nerve (CN VIII) → cochlear nuclei → auditory cortex (temporal lobe). Conductive hearing loss affects the outer or middle ear; sensorineural hearing loss (SNHL) involves the cochlea or auditory nerve. These structural foundations predict the types of hearing and vision loss encountered in the elderly.
Age-Related Vision Loss: Pathophysiology and Causes
Visual impairment in the elderly results from a combination of normal age-related optical changes and specific age-related diseases. Understanding the distinction is essential for clinical assessment: some changes are universal (presbyopia), while others are pathological and require specific treatment.
Normal age-related visual changes: Presbyopia — the age-related loss of accommodation due to hardening of the crystalline lens (reduced elasticity of lens fibres) and decreased ciliary muscle strength; produces difficulty with near vision (reading, fine detail); begins in the 4th decade and affects virtually everyone by age 50; corrected with reading glasses or bifocals (convex lenses). Reduced pupil size (pupillary miosis) in the elderly reduces the amount of light reaching the retina and increases the depth of field; elderly individuals require significantly more light for equivalent visual function — a practical implication for home lighting assessment. Reduced dark adaptation (slower rhodopsin regeneration) impairs driving at night and navigating in dim environments. Reduced contrast sensitivity (distinct from acuity reduction) impairs the ability to see objects against similar-toned backgrounds — a major cause of falls on stairs and kerbs.
Cataract: A cataract is an opacity of the crystalline lens causing gradual, painless, progressive loss of vision. It is by far the most common cause of visual impairment in elderly Indians and the world's leading cause of reversible blindness. Senile nuclear cataract (the most common type) results from progressive oxidation and protein aggregation in the lens nucleus, causing yellowing and progressive opacification. Clinical features: gradual, painless vision blurring; glare (light scattering at the lens opacity — especially from oncoming headlights); reduced visual acuity on Snellen chart testing; absent red reflex (replaced by white or grey opacity) on direct ophthalmoscopy; visible lens opacity on slit-lamp examination. The NPCB+VI (National Programme for Control of Blindness and Visual Impairment) provides free cataract surgery through its network — awareness of this programme is important for Indian clinical practice. Cataract surgery (phacoemulsification — the standard surgical technique using ultrasonic lens fragmentation + intraocular lens implantation) is curative; post-operative visual outcome is excellent in uncomplicated cases. The indication for surgery is when the visual impairment significantly affects quality of life — there is no fixed visual acuity threshold.
Age-related macular degeneration (AMD): AMD is the leading cause of irreversible vision loss in the elderly in developed countries and increasingly in India. It affects the macula — the central retina responsible for fine vision — causing loss of central vision while preserving peripheral vision. Two forms: (1) Dry (geographic) AMD — 80–85% of cases; characterised by accumulation of extracellular protein-lipid deposits (drusen) under the retinal pigment epithelium, with progressive retinal pigment epithelium (RPE) atrophy; slow, progressive central vision loss; no curative treatment — management focuses on AREDS2 supplementation (high-dose vitamins C, E, zinc, lutein/zeaxanthin) to slow progression in intermediate AMD; (2) Wet (neovascular) AMD — 15–20% of cases; characterised by choroidal neovascularisation (abnormal blood vessel growth under the retina — stimulated by VEGF); can cause rapid, severe central vision loss within weeks; treatment: intravitreal anti-VEGF injections (ranibizumab, bevacizumab, aflibercept) stabilise or improve vision in 70–90% of cases when initiated promptly; this is the most important treatable cause of rapid vision loss in elderly patients.
Glaucoma: A group of conditions characterised by progressive optic nerve damage leading to irreversible visual field loss. Primary open-angle glaucoma (POAG) is the most common type in adults — characterised by elevated IOP (>21 mmHg in most cases) causing optic disc cupping (increased cup-to-disc ratio) and insidious peripheral visual field loss (initial arcuate scotomata); typically asymptomatic until late — central vision preserved until far advanced; requires regular screening (IOP measurement, optic disc assessment) in elderly. Acute angle-closure glaucoma — a dramatic emergency: sudden painful red eye with markedly elevated IOP (often >40 mmHg), nausea, vomiting, halos around lights, blurred vision; requires immediate treatment (IV acetazolamide, topical pilocarpine/timolol, laser peripheral iridotomy).
Diabetic retinopathy: A leading cause of vision loss in working-age adults and elderly diabetics. Pathophysiology: chronic hyperglycaemia → microvascular disease of retinal capillaries → basement membrane thickening, pericyte loss → vascular leakage (macular oedema — leading cause of diabetic vision loss) and neovascularisation (proliferative diabetic retinopathy — causes traction retinal detachment and vitreous haemorrhage). Annual dilated fundal examination is mandatory in all elderly diabetics; management includes strict glycaemic control, anti-VEGF injections (macular oedema), and laser photocoagulation (proliferative disease).
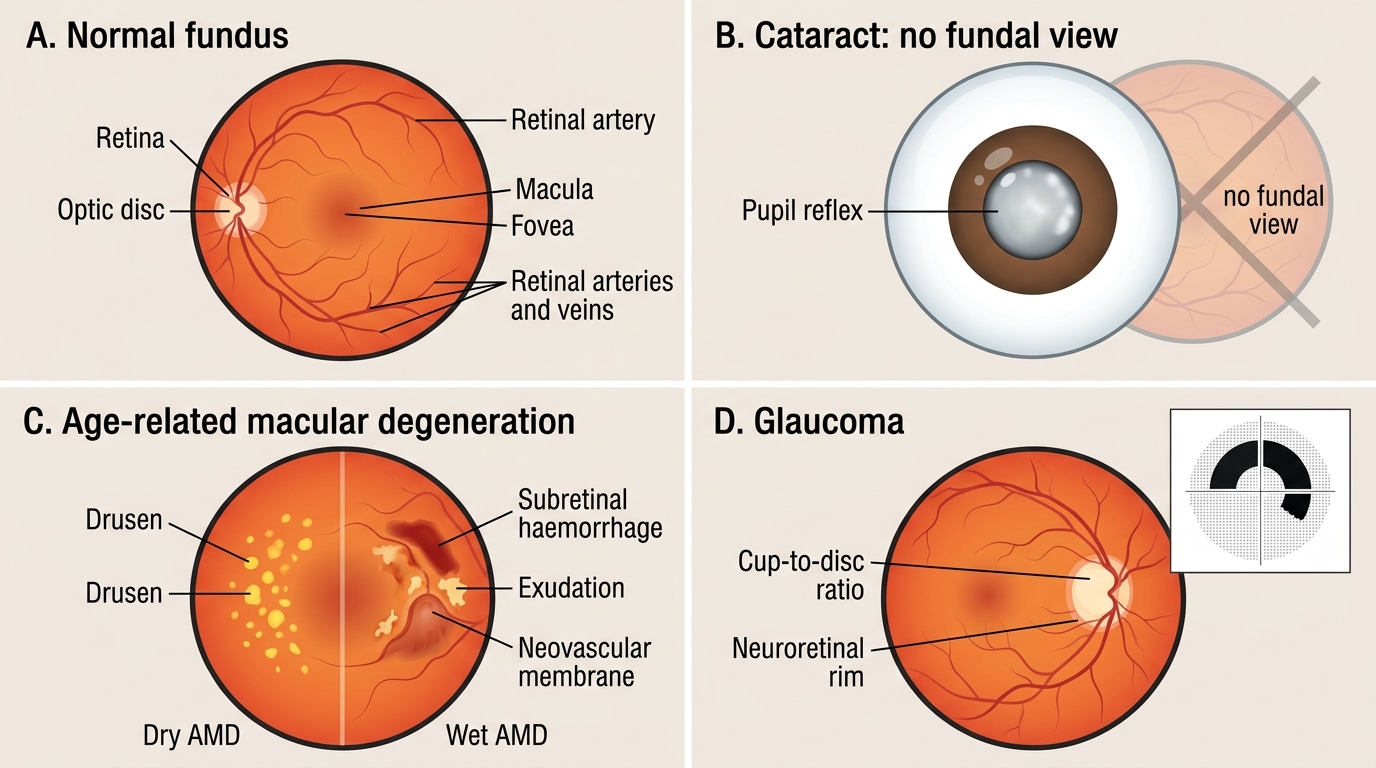
Common Elderly Eye Conditions: Fundus Comparison
Age-Related Hearing Loss: Pathophysiology and Causes
Presbycusis (age-related sensorineural hearing loss) is the most common cause of hearing loss in the elderly, affecting approximately 40–60% of Indians over 60 and rising to over 80% in those above 75. It results from the progressive, bilateral, and symmetrical degeneration of cochlear hair cells in the basal turn of the cochlea — the region responsible for high-frequency sound processing — combined with degeneration of the spiral ganglion neurons of the auditory nerve. The basal turn is preferentially affected because of its constant high metabolic activity and exposure to acoustic trauma over a lifetime.
The characteristic audiological profile of presbycusis: High-frequency sensorineural hearing loss (bilateral, symmetrical), with progressive difficulty hearing high-pitched sounds first (consonants such as 's', 'f', 'th', 'sh' — the consonants that provide speech intelligibility) while low-frequency sounds (vowels, environmental sounds) are preserved longer. The clinical consequence is that the patient can hear that someone is speaking but cannot understand what they are saying, especially in background noise. This is a crucial distinction from conductive hearing loss (where volume is globally reduced). Patients with presbycusis often say 'I can hear you but I cannot make out the words' — classically worsened in noisy environments (restaurant, group conversation), where they must also discriminate between competing voices.
Other causes of hearing loss in the elderly: While presbycusis is the most common, other causes must be systematically excluded: Noise-induced hearing loss (NIHL) — cumulative occupational or recreational noise exposure (factory workers, military personnel, musicians); also high-frequency SNHL but may be asymmetrical or notched at 4 kHz. Otosclerosis — progressive conductive and later sensorineural hearing loss from abnormal bone remodelling fixing the stapes footplate; autosomal dominant inheritance; treated surgically (stapedectomy) or with hearing aid. Chronic suppurative otitis media (CSOM) — a major cause of conductive hearing loss in India particularly in those with childhood history of ear discharge; may have mixed loss. Ototoxic drugs — aminoglycosides (cochlear damage — particularly in those with mitochondrial susceptibility), loop diuretics (reversible high-dose), quinine, cisplatin (irreversible cochlear toxicity, dose-dependent); elderly patients are more vulnerable because reduced renal clearance of aminoglycosides increases cochlear exposure. Acoustic neuroma (vestibular schwannoma) — benign tumour of the vestibulocochlear nerve; presents with unilateral progressive SNHL, tinnitus, and sometimes vestibular imbalance; must be excluded by MRI when hearing loss is unilateral or asymmetrical. Menière's disease — episodic vertigo, unilateral fluctuating SNHL, tinnitus, and aural fullness (tetrad); endolymphatic hydrops; less common in elderly but may present late.
Tinnitus — the perception of sound without an external source — is an almost universal accompaniment of sensorineural hearing loss in the elderly. It can be high-pitched ringing, hissing, or buzzing; typically worsened in quiet environments (particularly disturbing at night). Tinnitus is not a diagnosis itself but a symptom requiring audiological assessment. Management: tinnitus retraining therapy (TRT), sound masking, and treating underlying hearing loss with hearing aids (which paradoxically reduce tinnitus awareness by providing external sound to compete with the internal perception).
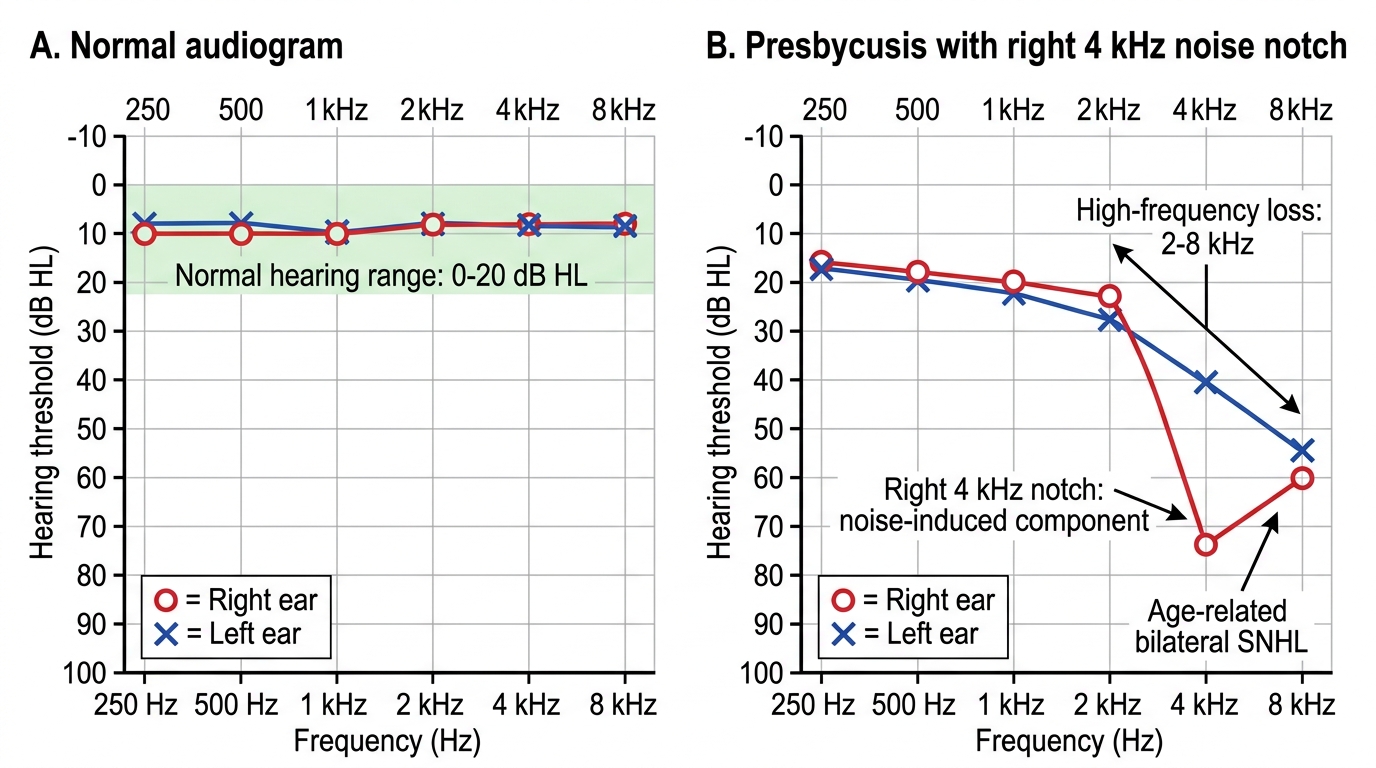
Normal Audiogram vs Presbycusis with 4 kHz Noise Notch
SELF-CHECK
A 74-year-old retired factory worker presents with bilateral hearing difficulty. His wife says he always turns up the television volume and asks people to repeat themselves. Audiometry shows bilateral high-frequency sensorineural hearing loss, symmetrical, with a 4 kHz notch on the right. Which combination of causes BEST explains this audiological profile?
A. Bilateral otosclerosis — the most common cause of bilateral hearing loss in the elderly
B. Presbycusis (age-related bilateral high-frequency SNHL) with an additional right-sided noise-induced notch at 4 kHz from occupational exposure
C. Bilateral acoustic neuromas — bilateral SNHL in elderly is almost always neoplastic
D. Chronic suppurative otitis media — bilateral discharge and conductive loss
Reveal Answer
Answer: B. Presbycusis (age-related bilateral high-frequency SNHL) with an additional right-sided noise-induced notch at 4 kHz from occupational exposure
Presbycusis produces bilateral, symmetrical, progressive high-frequency sensorineural hearing loss — fitting the bilateral component. The right-sided 4 kHz notch is the pathognomonic audiological signature of noise-induced hearing loss (NIHL) — the 4 kHz frequency is particularly vulnerable to acoustic trauma, and the right ear is often more exposed when operating machinery (right-hand dominant users position their left ear further from the machine). A retired factory worker has occupational noise exposure history. This combination is common in elderly males. Otosclerosis is conductive (not sensorineural). Bilateral acoustic neuromas are rare. CSOM causes conductive loss, not SNHL.
Functional Consequences, Investigation and Management of Sensory Loss
The functional consequences of sensory loss in the elderly extend far beyond the immediate sensory deficit and have broad clinical implications across geriatric domains. Both visual and hearing impairment independently and synergistically contribute to: falls risk (visual impairment impairs depth perception, contrast sensitivity, and environmental hazard detection; hearing loss impairs spatial awareness from vestibular contributions); cognitive decline (hearing loss is the largest modifiable risk factor for dementia in mid-life — Lancet Commission 2024; visual impairment also associated with cognitive decline, possibly through reduced environmental engagement and social participation); depression (social isolation from communication barriers and loss of enjoyable activities); functional dependence (IADLs — driving, shopping, using the telephone — all require intact sensory function); and communication barriers in healthcare (missed instructions, incorrect medication administration, diagnostic errors from miscommunication).
Clinical assessment of vision: Distance visual acuity: Snellen chart at 6 metres (6/6 = normal; 6/60 = can only see at 6 metres what a normal person sees at 60 metres); near visual acuity with Jaeger chart. Confrontation visual fields (identifies gross field defects — hemianopia, scotoma). Direct ophthalmoscopy (red reflex, fundal examination — disc, macula, vessels). Intraocular pressure (Goldmann tonometry — normal 10–21 mmHg). Colour vision (Ishihara plates — relevant for inherited defects, less used routinely in elderly). Referral criteria: significant reduction in distance acuity; any visual field loss; IOP >21 mmHg; abnormal fundal findings (optic disc changes, macular changes, haemorrhages).
Clinical assessment of hearing: Whisper test (a practical screening tool: stand 60 cm behind the patient, cup your hand over the ear not being tested, and whisper a combination of numbers and letters — the patient repeats; a failure to hear identifies significant hearing loss); Rinne and Weber tuning fork tests (512 Hz) — Rinne test distinguishes conductive from sensorineural loss (Rinne positive = air conduction > bone conduction = normal or SNHL; Rinne negative = bone > air = conductive loss); Weber test (midline — lateralises to better ear in SNHL, to worse ear in conductive loss). Audiometry (pure-tone audiometry) is the definitive investigation — provides hearing thresholds (dB) across frequencies (250–8000 Hz) for each ear separately via air and bone conduction. Speech audiometry measures speech discrimination (the most functionally relevant parameter). The HHIE-S (Hearing Handicap Inventory for the Elderly — Screening Version) is a 10-item questionnaire assessing the functional impact of hearing loss — validated for elderly screening.
Management of visual impairment: (1) Cataract: phacoemulsification + intraocular lens implantation — curative; available under NPCB+VI in India free of charge; typical visual outcome 6/6 to 6/9 in uncomplicated cases. (2) Glaucoma (POAG): topical prostaglandin analogues (latanoprost 0.005% — first-line; once daily, evening; reduces IOP by 25–30%); beta-blockers (timolol 0.5%); carbonic anhydrase inhibitors; laser trabeculoplasty; trabeculectomy for advanced cases. (3) Wet AMD: intravitreal anti-VEGF injections (ranibizumab, bevacizumab, aflibercept) — reduce VEGF-driven neovascularisation; typically given monthly for 3 months then as needed; must be started promptly to prevent permanent scarring. Dry AMD: AREDS2 supplements to slow progression. (4) Diabetic macular oedema: anti-VEGF first-line; laser photocoagulation for peripheral proliferative disease. (5) Low vision rehabilitation: for irreversible vision loss — magnifiers, large-print materials, talking clocks, smartphone accessibility features; occupational therapy for home hazard modification.
Management of hearing loss: (1) Hearing aids are the mainstay of treatment for presbycusis and most other causes of permanent hearing loss. Modern behind-the-ear (BTE) and in-the-ear (ITE) digital hearing aids amplify selectively across frequencies, reduce background noise, and have Bluetooth connectivity. Patient acceptance and adherence are major challenges — many elderly patients delay seeking treatment (average 7–10 years between first noticing hearing loss and fitting a hearing aid) due to stigma, cost, or denial; counselling about the consequences of untreated hearing loss (dementia risk, social isolation) improves motivation. Assistive listening devices (ALDs) — personal amplifiers, telephone amplifiers, visual doorbell alerts, captioned telephones — supplement hearing aid use. (2) Cochlear implants — for profound bilateral sensorineural hearing loss unresponsive to hearing aids; technology is effective in elderly patients with excellent outcomes for speech recognition; not yet widely available in India's public health system but available in tertiary centres. (3) Cerumen (earwax) management — impacted cerumen is a reversible cause of conductive hearing loss; irrigation or microsuction; counsel against cotton bud use. (4) Surgical options — stapedectomy for otosclerosis, tympanoplasty for CSOM with perforation.
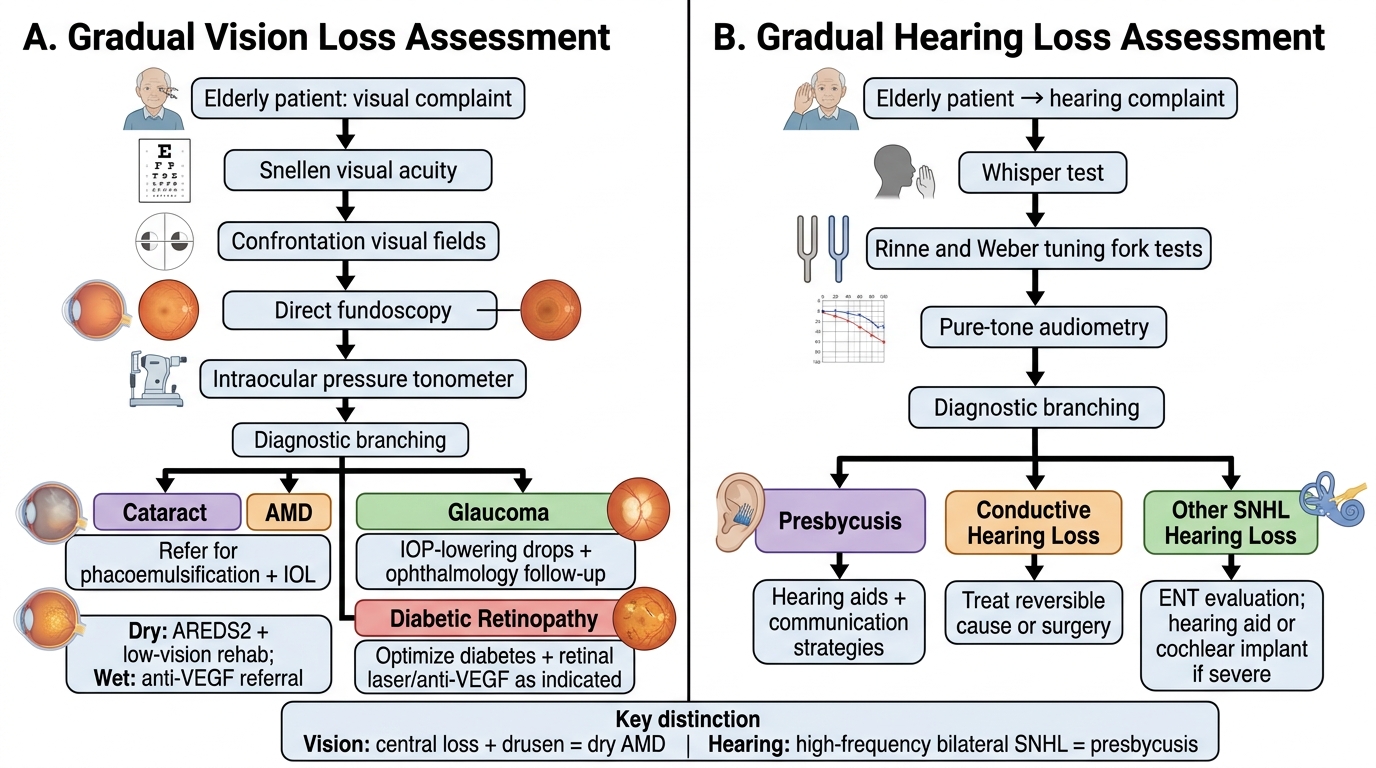
Assessment and Management of Vision and Hearing Loss in Older Adults
SELF-CHECK
An 80-year-old woman presents with a 3-year history of gradual visual loss. She reports difficulty reading fine print and recognising faces but can navigate her home and detect environmental hazards. On direct ophthalmoscopy, a grey stippled appearance is visible at the macula bilaterally with numerous small yellowish deposits. Visual acuity is 6/24 bilaterally; peripheral fields are intact. What is the most likely diagnosis and the appropriate initial management?
A. Primary open-angle glaucoma — start topical timolol and refer for IOP monitoring
B. Dry age-related macular degeneration (AMD) — manage with AREDS2 supplementation and low-vision rehabilitation; monitor for conversion to wet AMD
C. Diabetic macular oedema — start anti-VEGF injections and optimise glycaemic control
D. Bilateral cataracts — refer for phacoemulsification surgery
Reveal Answer
Answer: B. Dry age-related macular degeneration (AMD) — manage with AREDS2 supplementation and low-vision rehabilitation; monitor for conversion to wet AMD
The presentation is classic for dry AMD: bilateral, gradual, central visual loss (reading/face recognition — macula-dependent tasks) with preserved peripheral vision (navigation intact); bilateral macular drusen (yellowish deposits) and retinal pigment epithelium changes visible on fundoscopy; age 80 — AMD prevalence rises sharply after 75. Management of dry AMD: AREDS2 supplementation (high-dose vitamins C, E, zinc, lutein/zeaxanthin) slows progression in intermediate-to-advanced dry AMD. Low-vision rehabilitation for current impairment. Annual monitoring for conversion to wet AMD (rapid vision loss, straight lines appearing wavy — metamorphopsia, on Amsler grid — is the alert sign that triggers urgent anti-VEGF referral). POAG causes peripheral field loss, not central; cataract causes blurring but red reflex is absent (not macular deposits); diabetic macular oedema requires diabetes history.