Page 23 of 32
IM25.19-21 | Geriatric Social and Ethical Care — SDL Guide (Part 2)
Applied Practice: Social Screening, Abuse Response, and Goals-of-Care Conversations
The applied skills in geriatric social and ethical care translate the knowledge from earlier arc steps into clinical actions. Three practical domains are covered here: conducting a social screen as part of the CGA, responding to identified elder abuse, and initiating a goals-of-care conversation. These are the techniques the clinician must internalise and practise.
Social screening should be routine in every geriatric assessment and in any hospitalised elderly patient. A structured social screen covers: (1) Living situation — does the patient live alone or with family? Are there adequate utilities (water, electricity, heating/cooling)? (2) Caregiver support — who provides day-to-day help? What are the caregiver's own health and capacity? Is there caregiver burden (screened with the Zarit Caregiver Burden Interview or a simple single-item question)? (3) Financial security — does the patient have adequate income for medications and food? (4) Social connectedness — frequency of contact with family and friends; loneliness screening. (5) Safety — is the home safe? Are there fall hazards? Is there a history of abuse or neglect? The result of the social screen directly shapes the care plan: an isolated patient needs different discharge planning than one with a robust support network; a patient with suspected abuse needs a different response than one with merely inadequate social support.
Responding to elder abuse requires a structured clinical-legal response. The first step is documentation — objective, detailed, and non-judgmental. Document the history in the patient's own words using quotation marks, note all physical findings with body maps, and photograph injuries where consent is obtained. The second step is safety assessment — is the patient safe to return to the same environment? Can they access help if needed? The third step is disclosure and reporting — in India, the Maintenance and Welfare of Parents and Senior Citizens Act 2007 provides a maintenance tribunal mechanism, and police complaint is available for physical abuse. The fourth step is referral — to social work, to legal aid, to NGOs such as HelpAge India, and, where appropriate, to community health workers (ASHAs) for follow-up. The clinician's role is neither to adjudicate the abuse nor to force the patient to leave the abusive situation against their will (if they have capacity) — but to ensure they have the information, resources, and support to make an informed choice and to be safe.
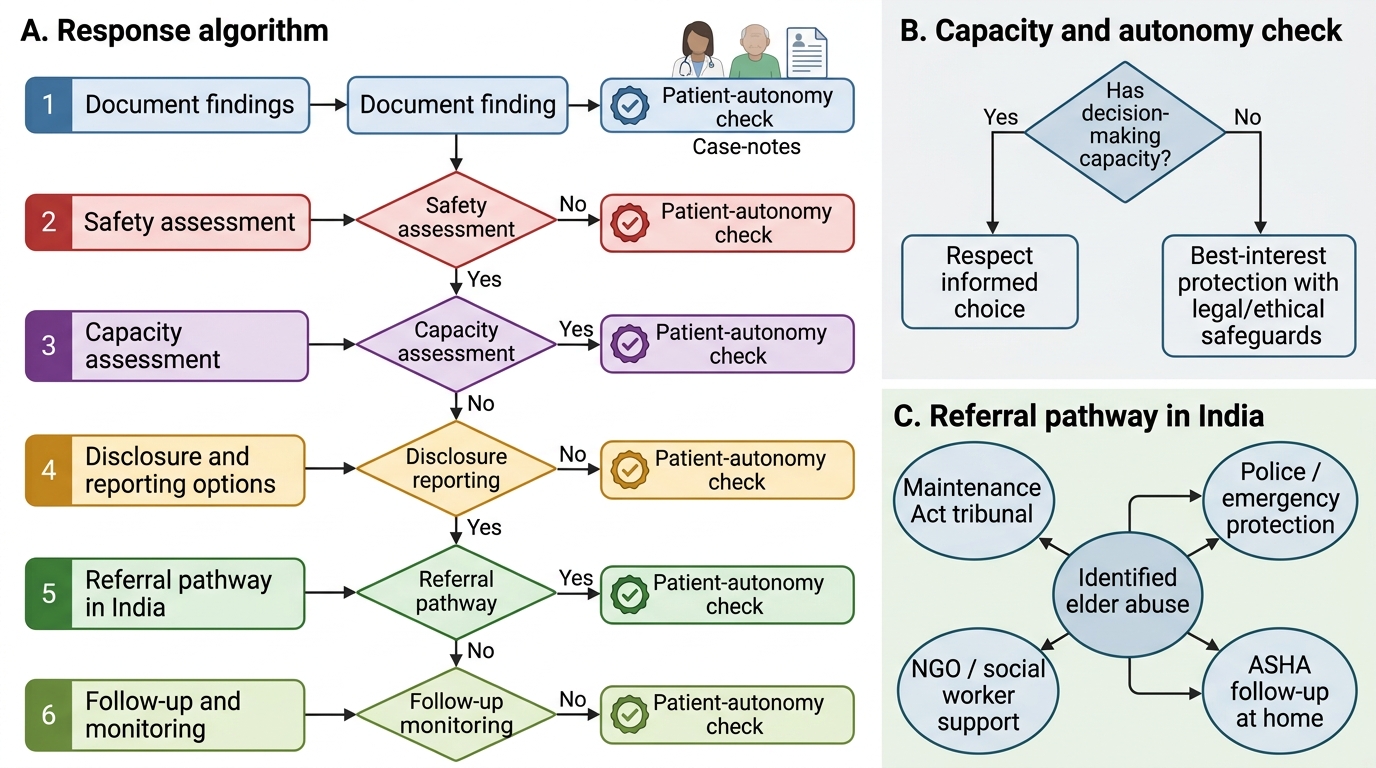
Algorithm for Responding to Identified Elder Abuse
Goals-of-care conversations are structured clinical encounters, not incidental corridor exchanges. The SPIKES protocol (Setting, Perception, Invitation, Knowledge, Empathy, Strategy/Summary) — developed for breaking bad news — applies with modification to goals-of-care discussions. The key elements: (1) choose a quiet, private setting with the patient (if capacitous) and key family members present; (2) elicit what the patient and family understand about the current condition and its trajectory; (3) ask what matters most to the patient ('What does a good day look like for you?' or 'What would you be willing to go through to get more time?'); (4) share clinical information about prognosis and options honestly; (5) express empathy when the information is difficult; and (6) agree on a plan that reflects the patient's values — whether that is full resuscitation and aggressive treatment, comfort-focused care, or something in between. Document the conversation and the agreed plan clearly in the notes.
SELF-CHECK
A physician is discharging an 80-year-old woman who lives alone after a fall with minor injuries. Social screening reveals she has no family in the city, depends on a neighbour for meals, and reports feeling lonely most days. Which is the MOST appropriate next step for discharge planning?
A. Discharge with standard fall precaution advice and no additional referral
B. Retain in hospital until family can be located
C. Refer to social work, provide information about domiciliary care services and day centres, and arrange ASHA or community health worker follow-up
D. Recommend transfer to a private old-age home
Reveal Answer
Answer: C. Refer to social work, provide information about domiciliary care services and day centres, and arrange ASHA or community health worker follow-up
The patient has multiple identified social risk factors — isolation, dependence on a single informal support person, and reported loneliness — that must be addressed before discharge. Simply discharging with advice (option A) leaves these risks unaddressed and increases re-admission risk. Detaining a capacitous patient who is medically fit for discharge (option B) is ethically impermissible without legal authority. Recommending institutional care (option D) is premature when domiciliary options have not been explored and violates the ageing-in-place principle. The appropriate response is multidisciplinary social work referral, information about community services, and community follow-up — ideally through the ASHA network for ongoing monitoring.
Self-Assessment: Integrating Geriatric Social and Ethical Reasoning
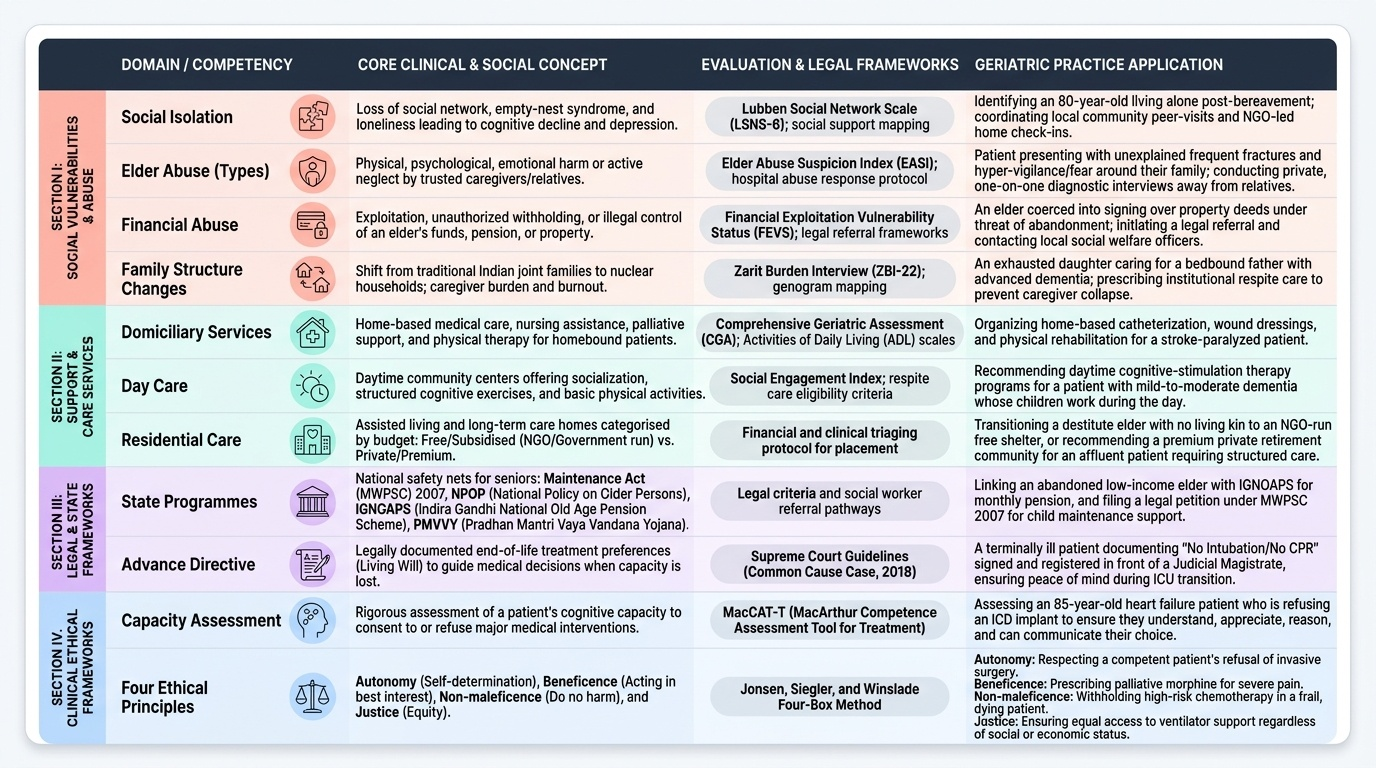
At this point in the module you have studied the major social problems of elderly patients, the spectrum of available social interventions in the Indian context, and the ethical frameworks governing clinical decision-making in geriatric care. This self-assessment section consolidates that learning through applied scenario-based exercises and a reference summary table. For each scenario below, work through the clinical reasoning before reading the analysis — identify the social or ethical problem, apply the relevant framework (capacity assessment, abuse response protocol, social intervention menu, ethical principle), and arrive at a management decision. The goal is to develop the reflective, structured approach that the IM25.19–IM25.21 competencies require at the KH level. Notice, as you work through these scenarios, that the social and ethical dimensions of each case are not separable from the clinical dimensions — they are the clinical problem. A physician who identifies the acute medical issue but misses the abuse, the capacity question, or the social support gap has delivered incomplete care. This integrated clinical-social-ethical reasoning is the hallmark of excellence in geriatric medicine and is what examiners test at the applied KH level. These scenarios are deliberately drawn from realistic Indian clinical settings — emergency admissions, pre-discharge assessments, end-of-life disputes — where the social and legal context is inseparable from the clinical decision. Work through them not as examination exercises but as rehearsals for the actual encounters you will face.
Provided image
Scenario A: An 85-year-old retired professor is admitted with worsening heart failure. He is alert and oriented. He refuses the recommended ICD implant, stating he has 'lived a full life' and does not want a surgical procedure. His daughter is insistent that 'everything possible' be done and accuses the clinical team of giving up on her father. How should the clinician proceed?
Analysis: The patient has demonstrated capacity (he is alert, oriented, and gives a coherent reason for his decision based on his values and life stage). A capacitous patient's refusal of an elective procedure must be respected — this is the principle of autonomy overriding beneficence. The clinician's role is to ensure the refusal is informed (that he understands the risks of not having an ICD — increased sudden death risk), not to change his mind. A goals-of-care conversation with the patient and daughter together, exploring the patient's values and the daughter's concerns, is indicated. The clinical team should not override the patient's decision to satisfy the family.
Scenario B: A 72-year-old man is being assessed for discharge after hip replacement surgery. He lives alone; his wife died two years ago. Assessment reveals moderate dependence for IADLs, mild cognitive impairment (MMSE 22/30), and a pension income of ₹8,000/month. He has no family in the city. What social interventions should be initiated?
Analysis: This patient requires a multidimensional discharge plan. IADL dependence → home health aide or domiciliary care service referral. Mild cognitive impairment → cognitive monitoring follow-up; medication safety review. Low income → IGNOAPS application if eligible; assessment for HelpAge India domiciliary services. Social isolation → day care centre referral for social programming and monitoring. The physiotherapy for post-surgical rehabilitation can be arranged as a domiciliary service initially, transitioning to a day rehabilitation facility. The Maintenance Act 2007 is not applicable here (no evidence of abuse or responsible family neglect). This is an integrated social care discharge plan, not merely a medical discharge.
Scenario C: A 78-year-old woman with advanced Alzheimer's disease is admitted in respiratory failure. Her advance directive, executed 5 years ago, states she does not wish to be intubated or maintained on mechanical ventilation. Her son is present and insists on full resuscitation including intubation. The advance directive is registered with the local Collector as per the Supreme Court's Common Cause 2018 guidelines. What is the clinician's ethical and legal obligation?
Analysis: A validly executed, properly registered advance directive is legally binding in India following Common Cause v Union of India 2018. The patient expressed, when capacitous, her wish not to be intubated. The son's demands do not override a registered advance directive. The clinician's obligation is to honour the advance directive and provide comfort-focused care (oxygen, symptom management). A Medical Board assessment may be convened per the Supreme Court guidelines to confirm the applicability of the directive to this specific clinical situation. The son should be compassionately informed of the legal and ethical situation.
Self-Assessment: Ethical Principles Applied
This final self-assessment block consolidates the ethical principles and social care skills developed throughout the module, offering an integrative review exercise and a structured approach to preparing for assessments on IM25.19–IM25.21 competencies. The four bioethical principles — autonomy, beneficence, non-maleficence, and justice — are not applied in isolation but in tension with each other; the skill lies in identifying which principle is dominant in a given situation and how to navigate the conflict when more than one applies. In practice, geriatric ethical dilemmas rarely involve a clean application of a single principle. More commonly, beneficence (acting in the patient's best interest) conflicts with autonomy (respecting the patient's right to refuse), or justice (fair use of limited resources) conflicts with beneficence (providing maximum benefit to one individual). The clinician who can name the competing principles, articulate why each applies, and reason through to a defensible decision is the one who performs well in both examinations and real clinical practice. The Indian legal anchors covered in this module — the Maintenance Act 2007 and the Common Cause judgment of 2018 — are high-yield examination targets that also have genuine practical relevance for every physician practising in India.
Consolidation framework — applying the four principles in geriatric practice:
| Principle | Geriatric application | Common clinical scenario |
|---|---|---|
| Autonomy | Respect informed refusal of treatment; capacity assessment before override; advance directives | Elderly patient refuses surgery; advance directive refusing CPR |
| Beneficence | Treat reversible conditions; provide adequate analgesia; arrange social support | Under-treated pain in dementia; inadequate discharge planning |
| Non-maleficence | Avoid futile or disproportionately burdensome treatment; polypharmacy review | Stopping a Beers-listed drug; declining CPR in end-stage cancer |
| Justice | Allocate resources on clinical need not age alone; address social inequity; challenge ageism | ICU triage using Clinical Frailty Scale, not age; IGNOAPS for destitute elderly |
Key legal and policy anchors in India:
- Common Cause v Union of India (2018): advance directives are legally valid; right to die with dignity; Medical Board mechanism for implementation.
- Maintenance and Welfare of Parents and Senior Citizens Act (2007): children/heirs legally obligated to maintain parents/senior citizens; maintenance tribunals; old-age homes in every district for BPL elderly.
- National Policy for Older Persons (NPOP, 1999 revised 2011): framework for health care, social security, and welfare of older persons.
- IGNOAPS: monthly pension to BPL elderly (₹200/month age 60–79, ₹500/month age ≥80).
- PMVVY: pension security scheme for elderly aged ≥60 years.
High-yield examination points:
- Six forms of elder abuse and their clinical indicators
- Capacity assessment as decision-specific and time-specific (not global)
- Common Cause 2018 judgment — right to advance directive and dying with dignity
- Maintenance Act 2007 — legal obligation of children and tribunal mechanism
- Social intervention spectrum from domiciliary → day centre → residential care
- Goals-of-care conversation structure (SPIKES)
- Four bioethical principles and their geriatric applications
Geriatric Social and Ethical Care Domains
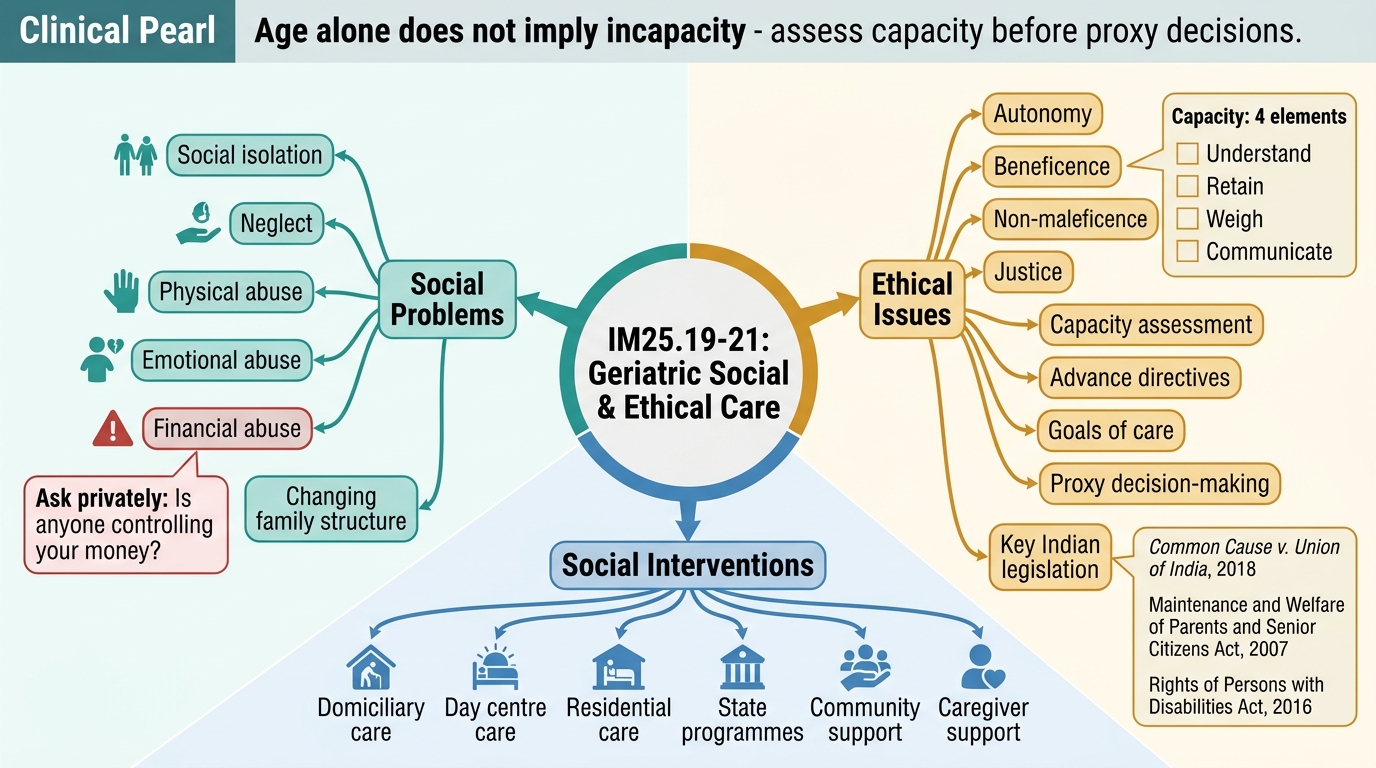
CLINICAL PEARL
The single most common ethical error in geriatric medicine is conflating age with incapacity. An 85-year-old patient who refuses treatment is not, by virtue of age alone, lacking capacity — and proceeding to override their decision without a formal capacity assessment is both ethically impermissible and legally indefensible following Common Cause (2018). Always conduct a capacity assessment before invoking proxy decision-making. Remember the four elements: understand, retain, weigh, communicate. A patient who can do all four has capacity, even if their decision is one you disagree with.
A second pearl: in India, financial abuse is the commonest form of elder abuse and is the one least likely to be volunteered. Ask every elderly patient seen alone, after the family has stepped outside: 'Is anyone controlling your money or preventing you from accessing it?' This single question, asked in a private clinical encounter, surfaces the most prevalent form of abuse that an unstructured consultation will miss.