Page 7 of 32
IM25.{4,9} | Geriatric Vascular Events and Stroke — SDL Guide
Learning Objectives
- Describe the epidemiology and risk factors for stroke in the Indian elderly population
- Classify ischaemic stroke by mechanism and explain how mechanism determines secondary prevention strategy
- Recognise atypical stroke presentations in the elderly including posterior circulation stroke syndromes
- Apply the ABCD² score for TIA risk stratification
- Describe the acute management of ischaemic stroke including eligibility for thrombolysis and mechanical thrombectomy, and the specific blood pressure management principles
- Calculate the CHA₂DS₂-VASc score and apply it to anticoagulation decisions in AF-related stroke in the elderly
INSTRUCTIONS
Stroke is a time-critical emergency with a reversible treatment window. This module teaches the pathophysiology that justifies the counterintuitive BP management rule in acute stroke, the NIHSS-based thrombolysis decision, the CHA₂DS₂-VASc anticoagulation framework, and the multidisciplinary rehabilitation approach. Mastering this content protects your elderly patients from the two leading drivers of stroke recurrence: untreated AF and inadequately controlled hypertension.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 419 — Ischaemic Stroke (textbook)
- API Textbook of Medicine, 11th ed., Chapter on Cerebrovascular Disease (textbook)
- AHA/ASA 2019 Guidelines for the Early Management of Patients with Acute Ischaemic Stroke (guideline)
- European Stroke Organisation 2021 Guidelines for the Management of Spontaneous Intracerebral Haemorrhage (guideline)
- AHA/ACC 2019 Guideline on AF Management — CHA₂DS₂-VASc and anticoagulation (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 10:30 AM. The family of 73-year-old Govindswamy rush him to the emergency department. He woke at 09:00 speaking normally but within minutes began slurring, dropped his morning tea cup, and now cannot lift his right arm. On examination: BP 178/102 mmHg, right hemiparesis, dysarthria, right facial droop. He is fully conscious. The clock is ticking — in ischaemic stroke, 1.9 million neurons die every minute without treatment. The registrar's instinct is to immediately lower the blood pressure. Should she? The answer — no, not yet — is one of the most important and counterintuitive management decisions in vascular medicine, driven by the pathophysiology of autoregulation loss in the acutely infarcted brain. Within four and a half hours of symptom onset, if there is no haemorrhage on CT and no contraindication, intravenous thrombolysis (alteplase) is the life-changing treatment. But in an 83-year-old man with previous stroke and on warfarin, the calculus changes entirely. Geriatric vascular medicine requires not only knowing the acute management protocols but knowing how age and comorbidity alter the risk-benefit equation.
WHY THIS MATTERS
Stroke is the leading cause of acquired disability in the elderly worldwide and the second leading cause of death in India. Stroke incidence doubles with every decade after age 55, meaning the elderly bear a disproportionate burden. Equally significant: approximately 20–25% of strokes in the elderly are preceded by a transient ischaemic attack (TIA) — a neurological emergency with a 10–15% risk of completed stroke within 90 days (one-third of those within the first 2 days). Recognising TIA and initiating urgent secondary prevention is as important as managing the completed stroke. NMC competencies IM25.4 (vascular events in the elderly) and IM25.9 (CVA in the elderly) require KH-level understanding of pathophysiology, atypical presentation in the elderly, acute and long-term management, and rehabilitation — all of which this module addresses.
RECALL
Activate your foundations in cerebrovascular anatomy. The middle cerebral artery (MCA) supplies the lateral cortex: motor/sensory cortex for the contralateral face and arm > leg, Broca area (dominant hemisphere, anterior), Wernicke area (dominant hemisphere, posterior). Anterior cerebral artery (ACA) supplies the medial frontal and parietal cortex: contralateral leg > arm, frontal lobe. Posterior cerebral artery (PCA) supplies the occipital cortex and thalamus: contralateral homonymous hemianopia, thalamic syndromes. Basilar artery supplies the brainstem: cranial nerve palsy ipsilateral + contralateral hemiparesis (crossed signs), coma. FAST clinical recognition: Face drooping, Arm weakness, Speech difficulty, Time to call emergency services. Recall also the distinction between ischaemic (80–85% of strokes) and haemorrhagic stroke (15–20%), as their management differs fundamentally — thrombolysis is given in ischaemic but is contraindicated in haemorrhagic stroke.
Epidemiology and Pathophysiology of Vascular Events in the Elderly
Cerebrovascular accident (CVA, stroke) is defined as a rapidly developing clinical sign of focal (or global) disturbance of cerebral function lasting more than 24 hours, with no apparent cause other than vascular origin. A transient ischaemic attack (TIA) is a brief episode of neurological dysfunction caused by focal brain or retinal ischaemia, with clinical symptoms typically lasting less than one hour (revised ABCD² definition) and without evidence of acute infarction on diffusion-weighted MRI. The traditional 24-hour duration threshold for TIA has been largely replaced by tissue-based definitions in clinical practice, but the 24-hour threshold is still used in NMC curriculum context.
The Indian burden is substantial: India has approximately 1.44 million new strokes annually, with a case fatality of 19–42% at 30 days and a 50–70% disability rate among survivors. In the elderly specifically, the risk factors for stroke are: hypertension (the single most important modifiable risk factor — accounts for approximately 35% of attributable stroke risk); atrial fibrillation (AF — the most important cardiac cause of cardioembolic stroke; carries a 5-fold increased stroke risk; the annual stroke rate in non-anticoagulated AF is 5% per year); diabetes mellitus (2–4 fold increased stroke risk); dyslipidaemia (LDL-C reduction with statins reduces stroke risk by approximately 20%); smoking (2-fold risk increase); and prior TIA or stroke (highest short-term risk period is immediately post-TIA).
The mechanism of ischaemic stroke defines management and prevention strategy. The four principal mechanisms are: (1) Large-vessel atherothrombosis — atherosclerotic plaque at carotid bifurcation or intracranially; accounts for approximately 20% of ischaemic strokes; typically produces cortical or watershed infarcts; secondary prevention requires antiplatelet therapy and management of atherosclerosis risk factors (statins, BP control). (2) Cardioembolic stroke — from intracardiac thrombus (most commonly from left atrial appendage in atrial fibrillation, or from left ventricular thrombus post-MI); accounts for approximately 25% of ischaemic strokes; characterised by sudden onset of maximum deficit, cortical infarcts in multiple vascular territories, and haemorrhagic transformation; secondary prevention requires anticoagulation (not antiplatelet — warfarin or DOAC). (3) Small-vessel (lacunar) disease — lipohyalinosis of penetrating arteries (lenticulostriate, pontine perforators); accounts for approximately 25%; produces small (≤1.5 cm) deep infarcts (lacunes) in the internal capsule, thalamus, basal ganglia, pons; presents with one of the classic lacunar syndromes (pure motor hemiparesis, pure sensory stroke, sensorimotor stroke, ataxic hemiparesis, dysarthria-clumsy hand); secondary prevention with aggressive BP control and antiplatelet therapy. (4) Cryptogenic stroke — no identifiable cause despite full investigation; accounts for approximately 30%; likely includes embolism from patent foramen ovale (PFO), small-vessel disease, atrial cardiopathy.
Haemorrhagic stroke comprises intracerebral haemorrhage (ICH) (most common haemorrhagic type — hypertension is the leading cause, rupturing small penetrating arteries; typical sites: putamen, thalamus, cerebellum, pons) and subarachnoid haemorrhage (SAH) (rupture of berry aneurysm — sudden onset worst headache of life). In the elderly, cerebral amyloid angiopathy (CAA) is an increasingly recognised cause of lobar ICH — amyloid-β deposition in cortical and leptomeningeal vessels causing fragility; associated with Alzheimer pathology.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
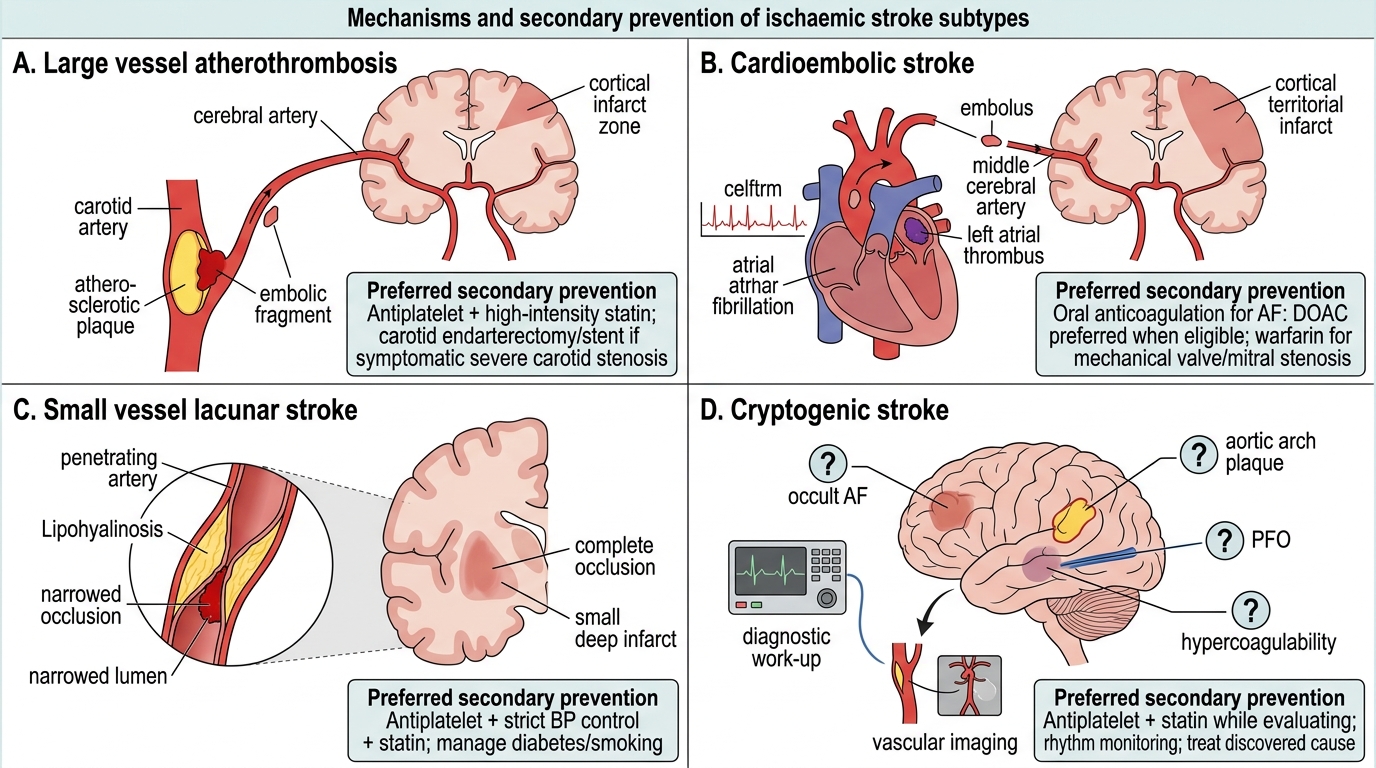
Ischaemic Stroke Subtypes: Mechanism and Secondary Prevention
Atypical Presentation and TIA Recognition in the Elderly
Atypical stroke presentation is more common in the elderly than in younger adults, and this creates diagnostic delays that translate to missed reperfusion windows and missed TIA recognition. Understanding why the elderly present atypically requires grasping the interplay between their pre-existing cerebrovascular disease, reduced physiological reserve, and altered pain and autonomic responses.
Provided image
Atypical features in elderly stroke: While the FAST symptoms (face drop, arm weakness, speech difficulty) remain the most common presentation, the elderly may additionally or exclusively present with: sudden-onset confusion or delirium (especially with thalamic or large MCA strokes — confusion without obvious focal deficit); unexplained falls (cerebellar or brainstem stroke causing ataxia and loss of balance without obvious hemiparesis); acute dysphagia (posterior circulation stroke — may present only as drooling or aspiration without hemiparesis); sudden onset vertigo with gait instability (posterior inferior cerebellar artery (PICA) territory — lateral medullary/Wallenberg syndrome); transient monocular blindness (amaurosis fugax) — TIA of the retinal artery, presenting as 'curtain across the vision' lasting minutes (often the warning before hemispheric stroke). In elderly patients with pre-existing dementia, cognitive baseline makes it difficult to identify new focal deficits — collateral history from a carer is essential.
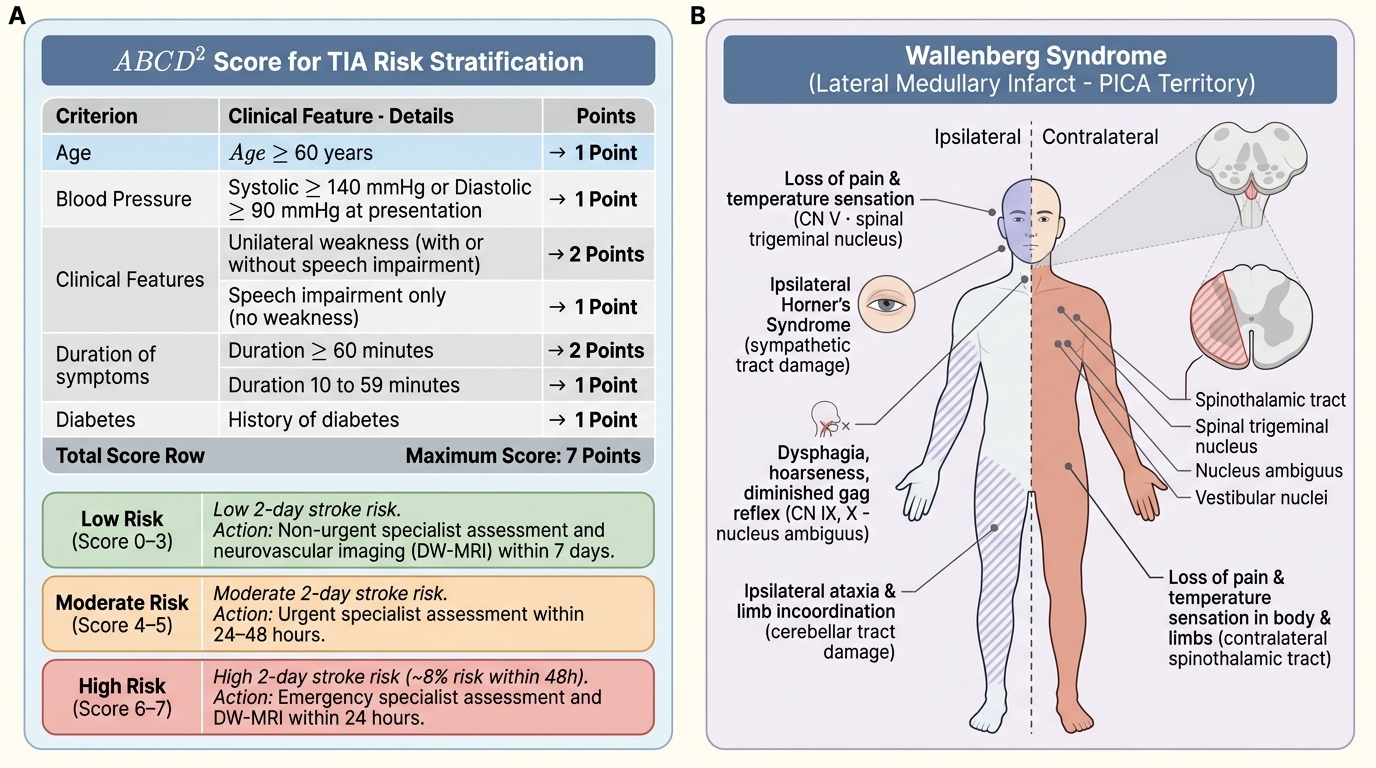
TIA recognition and the ABCD² score: The ABCD² score stratifies the 2-day stroke risk after TIA: Age ≥60 (1 point) + Blood pressure ≥140/90 at presentation (1 point) + Clinical features: unilateral weakness = 2, speech impairment only = 1 (0 if other) + Duration: ≥60 min = 2, 10–59 min = 1 (0 if <10 min) + Diabetes (1 point). Maximum score 7. Score ≤3 = low risk; 4–5 = moderate; 6–7 = high risk (8% 2-day stroke risk). In the UK/India current practice, the ABCD² score is used alongside neurovascular imaging (DW-MRI) to guide urgency of specialist assessment. All suspected TIA should be assessed within 24 hours (high-risk) or 7 days (low-risk) by a neurovascular specialist.
The Wallenberg syndrome (lateral medullary syndrome, PICA territory) is the prototype posterior circulation stroke and a classic examination topic. It presents with: ipsilateral facial pain/numbness (CN V nucleus); ipsilateral Homer syndrome (descending sympathetic chain); ipsilateral palatal palsy, dysarthria, dysphagia (CN IX, X nuclei); ipsilateral cerebellar ataxia; contralateral loss of pain and temperature in the limbs (spinothalamic tract). Because it does not cause hemiparesis, it may be mistaken for 'vestibular neuritis' or labyrinthitis — the distinguishing features are dysphagia, Horner syndrome, and crossed sensory signs, none of which occur in labyrinthitis.
SELF-CHECK
A 77-year-old hypertensive woman presents with sudden onset vertigo, difficulty swallowing, and unsteady gait beginning 2 hours ago. On examination: right-sided facial numbness, Horner syndrome on the right, falling to the right on Romberg test, absent gag reflex on the right, and decreased pain/temperature sensation on the left arm and leg. What is the most likely diagnosis and vascular territory?
A. Left middle cerebral artery ischaemic stroke — contralateral hemiparesis expected
B. Right posterior inferior cerebellar artery (PICA) occlusion causing right lateral medullary (Wallenberg) syndrome
C. Acute vestibular neuritis — reassure and prescribe vestibular sedatives
D. Left internal carotid artery dissection causing transient ischaemic attack
Reveal Answer
Answer: B. Right posterior inferior cerebellar artery (PICA) occlusion causing right lateral medullary (Wallenberg) syndrome
The combination of: ipsilateral (right) Horner syndrome, ipsilateral facial numbness, ipsilateral limb ataxia, ipsilateral palatal/gag palsy, AND contralateral (left) loss of pain and temperature — is the classic Wallenberg (lateral medullary) syndrome, caused by occlusion of the posterior inferior cerebellar artery (PICA) or vertebral artery supplying the right lateral medulla. The crossed sensory pattern (ipsilateral face + contralateral limbs) is pathognomonic. Vestibular neuritis does not cause dysphagia, Horner syndrome, or crossed sensory signs — these features mandate urgent CT/MRI brain to confirm stroke.
Acute Stroke Management: Diagnosis and Reperfusion
Acute stroke management follows the principle: 'time is brain.' Every minute without reperfusion causes approximately 1.9 million neurons to die. The system-level goal is minimising door-to-needle time to less than 60 minutes and door-to-puncture time (for thrombectomy) to less than 90 minutes. The individual clinical sequence is: recognise the stroke syndrome → arrange immediate brain imaging → determine eligibility for reperfusion → treat the precipitant and prevent complications.
Brain imaging: Non-contrast CT (NCCT) is the first-line investigation — available 24/7, fast, and reliably excludes haemorrhage (the critical first step before thrombolysis). NCCT is normal in the first 6–24 hours of ischaemic stroke (sensitivity for early ischaemia is 26–57%); however, it identifies haemorrhage as bright (hyperdense) immediately. MRI with diffusion-weighted imaging (DWI) is more sensitive for early ischaemia and is the gold standard for TIA (detecting small infarcts that confirm the TIA was in fact a completed small stroke). CT angiography (CTA) identifies large vessel occlusion (LVO) — essential for selecting candidates for mechanical thrombectomy.
Intravenous thrombolysis with alteplase (IV-tPA): The standard of care for eligible patients with ischaemic stroke. The treatment window is 4.5 hours from symptom onset (or from time last known well if onset unwitnessed). Dose: 0.9 mg/kg IV (maximum 90 mg), 10% as bolus, remainder over 60 minutes. Absolute contraindications include: haemorrhage on CT; previous intracranial haemorrhage; symptoms onset >4.5 hours (or unknown onset); blood glucose <50 or >400 mg/dL; platelet count <100,000; current anticoagulation with therapeutic INR or DOAC use; major surgery or trauma within 3 months. Geriatric considerations for thrombolysis: Age is NOT an absolute contraindication — randomised evidence (IST-3 trial) supports benefit in patients over 80, though the risk of symptomatic intracranial haemorrhage (sICH) is somewhat higher. The NIHSS stroke severity score guides eligibility; very mild strokes (NIHSS ≤3–4) may not benefit from thrombolysis. The decision in elderly patients should account for pre-stroke functional status (thrombolysis in a patient already fully dependent from prior stroke offers limited benefit).
Mechanical thrombectomy (MT, endovascular treatment): For eligible patients with large vessel occlusion (LVO — typically MCA or basilar artery) confirmed on CTA, mechanical thrombectomy using a stent retriever or aspiration catheter performed within 24 hours (extended to 24 hours in selected patients with evidence of salvageable penumbra on perfusion imaging) achieves recanalization rates of 85–90%, with significantly better outcomes than medical management alone (number needed to treat = 2.6 for functional independence at 3 months, from pooled RCT data). Older patients benefit from MT, though baseline functional status must guide patient selection.
Blood pressure management in acute stroke: One of the most counterintuitive aspects of acute stroke management. In the acutely infarcted brain, autoregulation is impaired in the ischaemic penumbra, meaning cerebral perfusion becomes pressure-dependent. Lowering BP aggressively in the first 24–48 hours can extend the infarct by reducing perfusion to the ischaemic penumbra. Current guidelines (AHA/ASA): In ischaemic stroke candidates for thrombolysis, BP must be brought below 185/110 mmHg BEFORE administering tPA; post-tPA, maintain BP <180/105 mmHg for 24 hours. In patients NOT receiving reperfusion, permissive hypertension up to 220/120 mmHg is allowed in the first 24–48 hours. In haemorrhagic stroke (ICH), blood pressure reduction is recommended: target systolic BP 130–180 mmHg (INTERACT-2 trial: rapid reduction to <140 mmHg is safe and trends to better outcomes); avoid SBP <130 mmHg.
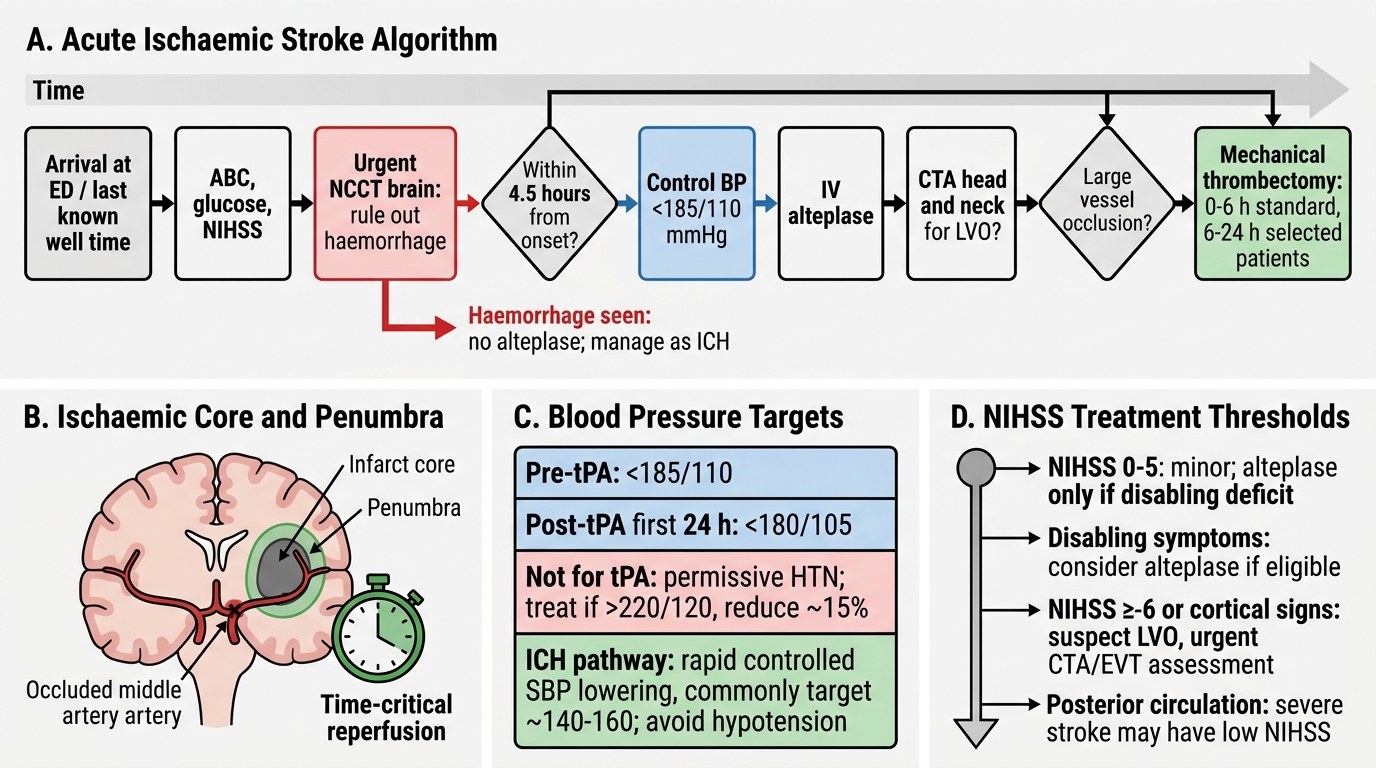
Acute Ischaemic Stroke: Time-Based Management Algorithm