Page 10 of 35
IM26.12-13 | Central Nervous System and Clostridial Infections — SDL Guide (Part 2)
Management: Bacterial Meningitis, Encephalitis, Tetanus, Botulism, and Gas Gangrene
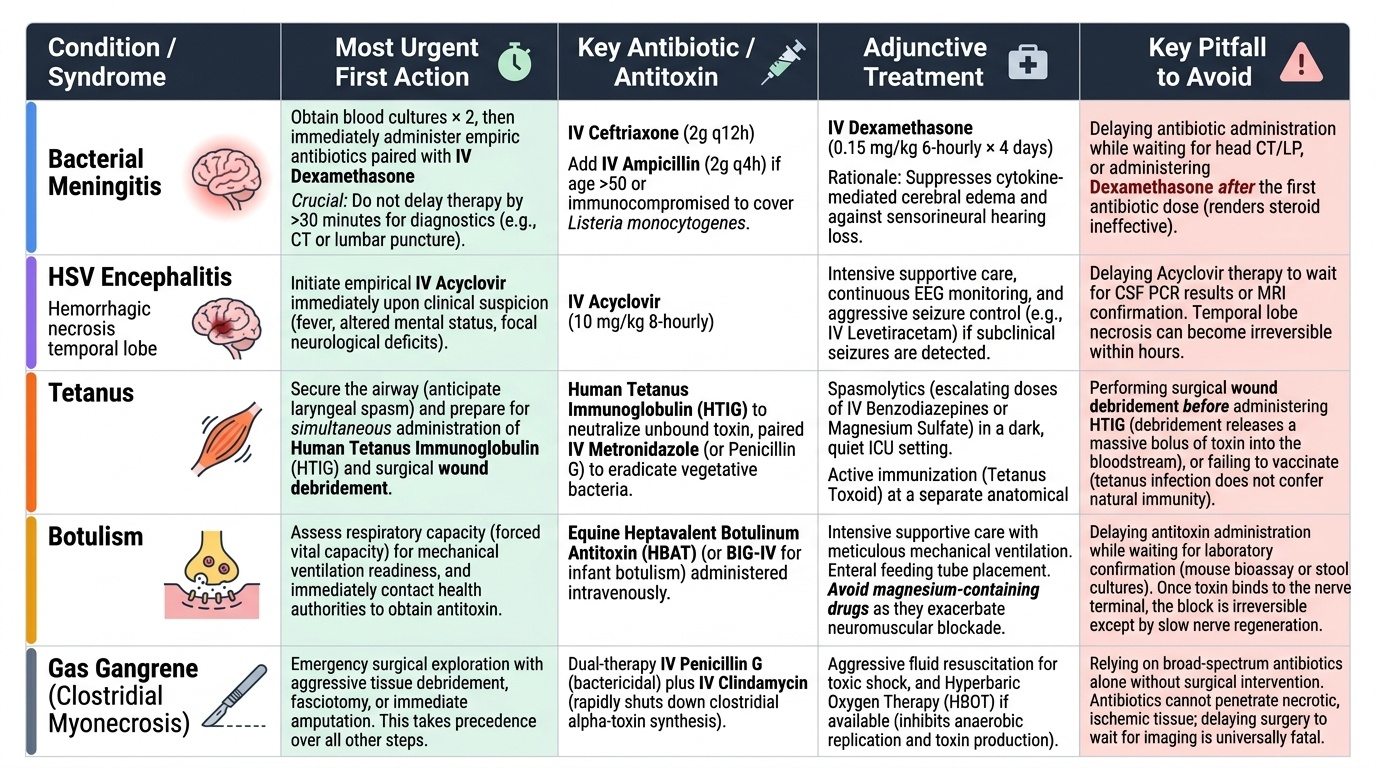
The management of CNS infections and clostridial syndromes is time-critical across all conditions in this SDL — the unifying principle is that each intervention must be started without waiting for complete diagnostic certainty, because the margin between early and delayed treatment is measured in lives and irreversible neurological damage. What follows is a structured management summary for each condition, with a focus on the India-specific context and the most commonly tested clinical decision points. The critical insight that cuts across all five conditions is this: each has a specific mechanism by which delay kills or disables — bacterial meningitis kills through uncontrolled neuroinflammation; herpes encephalitis destroys the temporal lobe with haemorrhagic necrosis; tetanus kills through respiratory failure from laryngeal spasm; botulism kills through diaphragmatic paralysis; and gas gangrene kills through the alpha-toxin–mediated haemolysis and multi-organ failure that outpace any antibiotic regimen if surgery is withheld. Knowing this mechanism predicts which intervention is most urgent in each case. In bacterial meningitis, antibiotics + dexamethasone together are the priority. In tetanus, HTIG plus wound debridement must be simultaneous — HTIG without wound care leaves the toxin source intact; wound debridement without HTIG leaves circulating toxin free to bind. In gas gangrene, no antibiotic regimen replaces the surgical knife.
Provided image
Bacterial meningitis — management algorithm:
1. Resuscitation and blood cultures: IV access, blood cultures × 2 before antibiotics if possible — but never delay antibiotics by >30 minutes for cultures in a sick patient.
2. Dexamethasone before or with first antibiotic dose: IV dexamethasone 0.15 mg/kg 6-hourly × 4 days. Rationale: suppresses cytokine-mediated cerebral oedema and sensorineural hearing loss. Most effective when given before the first antibiotic dose (de Gans trial, NEJM 2002). Do not give dexamethasone if bacterial meningitis is not suspected or if the causative organism is known to be non-pneumococcal at initial assessment.
3. Empirical antibiotics by age/risk: Adults 16–50 years: IV ceftriaxone 2g 12-hourly. Adults >50 years / immunocompromised: IV ceftriaxone + IV ampicillin 2g 4-hourly (Listeria cover — cephalosporins have no activity against Listeria). Penicillin allergy: IV chloramphenicol 1g 6-hourly. Post-neurosurgery/trauma (MRSA risk): add IV vancomycin.
4. CT head (if indicated before LP): papilloedema, focal neurology, GCS ≤10, immunocompromised, new seizures — CT before LP; antibiotics must NOT await CT results.
5. Lumbar puncture as soon as safe: interpret CSF using the profile table.
6. Duration: 7–10 days for N. meningitidis; 10–14 days for S. pneumoniae; 21 days for Listeria.
7. Complications: raised ICP (neurosurgical review), SIADH (dilutional hyponatraemia — fluid restriction, sodium supplementation), hearing loss (audiological follow-up at 6 weeks), seizures (IV lorazepam acutely).
8. Contact prophylaxis for meningococcal disease: all household contacts → rifampicin 600 mg twice daily × 2 days, OR ciprofloxacin 500 mg single oral dose, OR ceftriaxone 250 mg IM single dose.
Herpes simplex encephalitis: IV aciclovir 10 mg/kg 8-hourly × 14–21 days. Maintain adequate IV hydration (aciclovir crystallises in renal tubules in dehydrated patients). Anti-epileptic drugs for seizures. ICU care for decreased consciousness. Continue aciclovir even if PCR is initially negative if clinical suspicion remains strong — early PCR can be falsely negative.
Tetanus — 5 simultaneous interventions:
1. HTIG 3000–6000 units IM (or equine ATS if HTIG unavailable — test dose first for anaphylaxis). Give as early as possible to neutralise circulating unbound toxin.
2. Wound debridement: thorough surgical excision removes the organism and stops further toxin production. Even a healed wound should be explored if the source is a recent wound.
3. Antibiotics — IV metronidazole 500 mg 8-hourly × 10 days (drug of choice; kills C. tetani). Note: penicillin is a GABA antagonist at high doses and is no longer preferred for tetanus.
4. Muscle relaxation: IV diazepam 10–40 mg/hour by continuous infusion (enhances GABA action, counteracting toxin's GABA suppression). In severe Grade III–IV: neuromuscular blockade (vecuronium) with ICU ventilation. Patient must be in a dark, quiet room — all stimuli minimised.
5. Airway management: prophylactic tracheostomy in moderate–severe tetanus (before laryngeal spasm); mechanical ventilation for respiratory failure.
Severity grading (Ablett): Grade I — trismus only; Grade II — trismus + dysphagia, mild spasms; Grade III — trismus + generalised spasms + autonomic instability + respiratory compromise; Grade IV — Grade III + haemodynamic instability.
Botulism: Early IV trivalent botulinum antitoxin (types A, B, E) — effective only against unbound circulating toxin. Supportive: mechanical ventilation for respiratory failure (the primary cause of death). No antibiotics needed for food-borne botulism (killing C. botulinum may release more toxin). Wound botulism: debridement + IV penicillin/metronidazole.
Gas gangrene (clostridial myonecrosis): Surgical emergency — immediate radical debridement or amputation of the affected muscle compartment (no antibiotic can substitute). IV benzylpenicillin G 24 million units/day by continuous infusion + IV clindamycin 900 mg 8-hourly (clindamycin inhibits ribosomal synthesis and therefore toxin production — an important adjunct). Hyperbaric oxygen is adjunctive where available. ICU care for septic shock and haemolytic anaemia.
SELF-CHECK
A 62-year-old man with type 2 diabetes presents with fever, headache, and confusion. He has neck stiffness but no rash. CSF shows: turbid, WBC 4,200/µL (80% PMNs), glucose 30 mg/dL (blood glucose 110 mg/dL), protein 380 mg/dL, Gram stain: small Gram-positive bacilli. Which empirical regimen is MOST appropriate?
A. IV ceftriaxone 2g 12-hourly alone
B. IV ceftriaxone 2g 12-hourly + IV ampicillin 2g 4-hourly + IV dexamethasone 0.15 mg/kg 6-hourly
C. IV aciclovir 10 mg/kg 8-hourly — Gram-positive bacilli suggest herpes
D. IV vancomycin alone — Gram-positive bacilli indicate MRSA meningitis
Reveal Answer
Answer: B. IV ceftriaxone 2g 12-hourly + IV ampicillin 2g 4-hourly + IV dexamethasone 0.15 mg/kg 6-hourly
Gram-positive bacilli in CSF from an elderly diabetic patient = Listeria monocytogenes. Listeria is intrinsically resistant to ALL cephalosporins (including ceftriaxone) — ceftriaxone alone would fail. Ampicillin (or penicillin) is the only beta-lactam with activity against Listeria and must be added. Dexamethasone is added as standard. Aciclovir is for viral encephalitis, not purulent bacterial meningitis. Vancomycin covers Gram-positive cocci, not Gram-positive bacilli.
SELF-CHECK
A 28-year-old heroin user ('skin-popping') presents with 3 days of descending weakness — first diplopia and dysphagia, then progressive bilateral arm and leg weakness. Temperature 37.2°C. No sensory loss. Deep tendon reflexes are absent. CSF: normal protein, normal WBC. The MOST likely diagnosis is:
A. Tetanus — IV drug use is a risk factor for contaminated wound infection with C. tetani
B. Guillain-Barré syndrome — ascending paralysis with areflexia and CSF albuminocytological dissociation
C. Wound botulism — descending flaccid paralysis, areflexia, no fever, no sensory loss in an IV drug user
D. Myasthenia gravis — fatigable weakness with diplopia and dysphagia
Reveal Answer
Answer: C. Wound botulism — descending flaccid paralysis, areflexia, no fever, no sensory loss in an IV drug user
Wound botulism from skin-popping: IV drug user, descending flaccid paralysis (cranial nerves first: diplopia, dysphagia → limb weakness), absent DTRs, no fever, no sensory loss, consciousness preserved, normal CSF. Tetanus produces ascending spastic (not flaccid) paralysis with trismus. Guillain-Barré is ascending and CSF typically shows albuminocytological dissociation (elevated protein, normal WBC) — not normal CSF. Myasthenia produces fatigable weakness — worse with use, better with rest — not progressive descending flaccid paralysis.
Self-Assessment: CNS and Clostridial Infections
You have now covered the full scope of CNS infections (bacterial meningitis, viral encephalitis) and clostridial neurotoxin syndromes (tetanus, botulism, gas gangrene). The scenarios below integrate the clinical, diagnostic, and therapeutic reasoning across both groups. Work through each case independently before reading the analysis — the goal is to build the habit of systematic clinical reasoning under time pressure.
Scenario A: A 35-year-old HIV-positive patient (CD4 count 68 cells/µL, not on ART) presents with 3 weeks of progressive headache, low-grade fever, and confusion. He has mild neck stiffness. CT head: no mass lesion. CSF: lymphocytic pleocytosis (80 WBC/µL), glucose 32 mg/dL (blood glucose 88 mg/dL), protein 180 mg/dL, Gram stain negative. India ink: encapsulated yeasts visualised.
Analysis: HIV + CD4 <100 + subacute headache + encapsulated yeasts = cryptococcal meningitis. Confirm: CSF CrAg (>98% sensitivity) and fungal culture. Treatment: Induction — IV amphotericin B 0.7–1.0 mg/kg/day + oral flucytosine 25 mg/kg QID × 2 weeks; consolidation — fluconazole 400 mg/day × 8 weeks; maintenance — fluconazole 200 mg/day lifelong until CD4 >200 on ART. Start ART at 5 weeks (delay reduces immune reconstitution inflammatory syndrome — IRIS risk). Monitor opening CSF pressure — elevated ICP is a major cause of early death; manage with serial therapeutic LP (drain to pressure <20 cm H₂O).
Scenario B: A 70-year-old woman who had a difficult tooth extraction 10 days ago presents with 4 days of jaw stiffness, neck stiffness, and 2 days of back spasms triggered by light and noise. Her vaccination history is unknown. Temperature 38.5°C.
Analysis: Dental extraction + trismus + reflex spasms triggered by sensory stimuli = tetanus (dental extraction can seed C. tetani). Grade II–III. Management: (1) HTIG 3000–6000 units IM immediately; (2) oral metronidazole 400 mg 8-hourly × 10 days; (3) IV diazepam infusion; (4) prophylactic tracheostomy given Grade III features; (5) quiet darkened ICU room; (6) primary tetanus vaccination course after recovery.
Scenario C: A 16-year-old presents with fever, severe headache, vomiting for 8 hours, and increasing drowsiness. Temperature 40.1°C, GCS 13, neck stiffness, no rash, no papilloedema. Kernig's sign positive.
Analysis: Classic bacterial meningitis, LP is safe (no papilloedema, no focal signs). Management: blood cultures × 2 → IV dexamethasone 0.15 mg/kg → IV ceftriaxone 2g (age 16, community-acquired) → LP immediately. CSF: if purulent with neutrophilia → continue ceftriaxone; if lymphocytic with normal glucose → viral meningitis (supportive care, add aciclovir if any encephalitic features); if lymphocytic with low glucose + high protein → TB meningitis (GeneXpert CSF, empirical anti-TB therapy).
Scenario D: A 55-year-old farmer presents 24 hours after sustaining a deep cut with a rusty plough. The wound has become exquisitely painful, with crepitus on palpation, bronzed skin discolouration, and malodorous dark discharge. He has fever (40°C), HR 128/min, BP 96/60 mmHg, and jaundice with haemoglobinuria.
Analysis: Deep contaminated wound + rapid progression + crepitus + haemolysis + systemic toxaemia = gas gangrene (clostridial myonecrosis). This is a surgical emergency — immediate surgical debridement of the wound ± amputation + IV benzylpenicillin + IV clindamycin + ICU care. No diagnostic delay; no antibiotic-first approach.
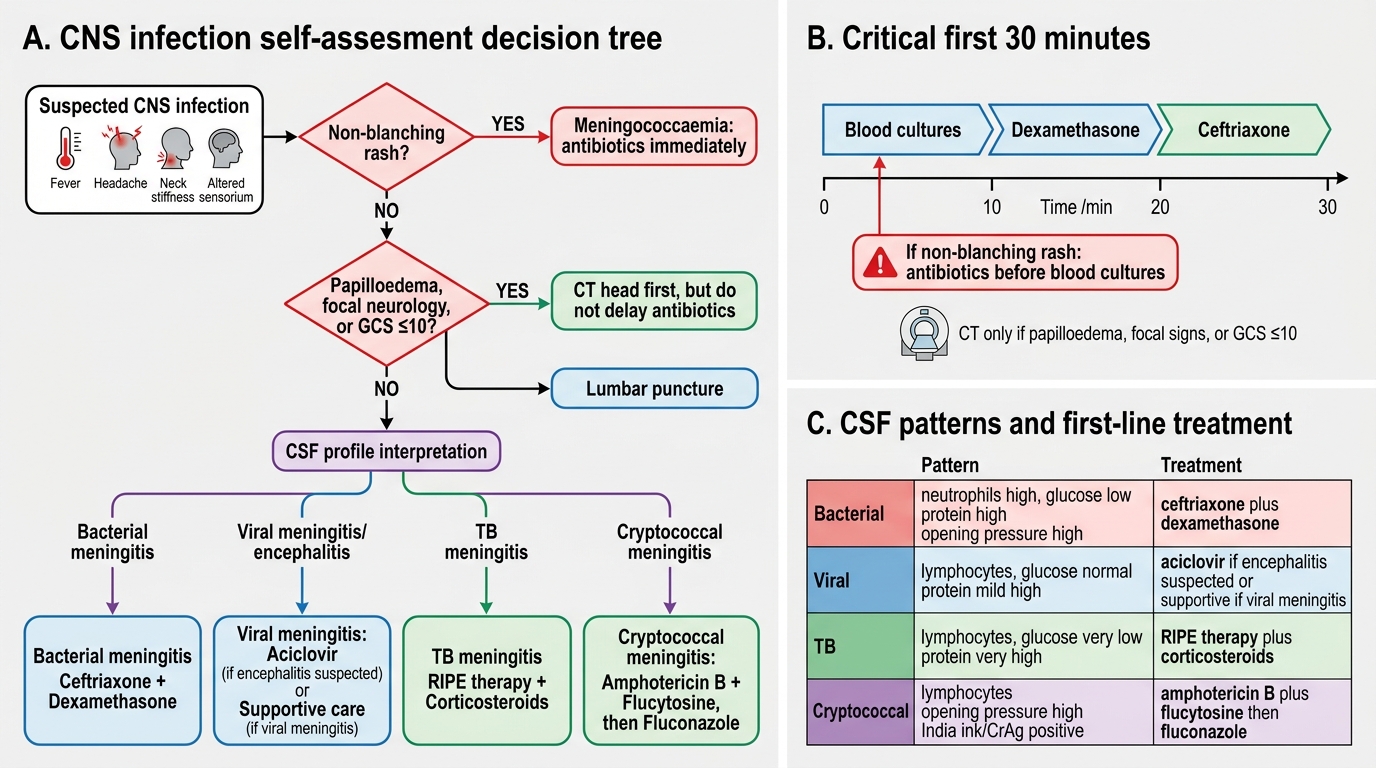
CNS Infection Decision Tree
CLINICAL PEARL
Two critical time-dependent decisions in this SDL: (1) In bacterial meningitis — do not let CT head delay antibiotics. The recommendation is: blood cultures → dexamethasone → ceftriaxone all within 30 minutes of presentation; CT is reserved only for patients with papilloedema, focal neurology, or GCS ≤10. In a patient with non-blanching rash, antibiotics go in before blood cultures. (2) In tetanus — metronidazole, not penicillin, is the antibiotic of choice. Penicillin at high doses acts as a GABA antagonist and can paradoxically worsen tetanic spasms. The mnemonic: TETANUS = ascending SPASTIC (jaw locked 'up'); BOTULISM = descending FLACCID (cranial nerves fall 'down'). The toxin location explains the direction: tetanus acts in the spinal cord (central → ascending effect); botulism acts at the peripheral NMJ (cranial nerve NMJs have the shortest axons → affected first, descending spread).