Page 13 of 35
IM26.15-16 | Gram Negative Nonfermenter and Helicobacter Infections — SDL Guide (Part 2)
Management Principles and Antibiotic Stewardship for Pseudomonas and H. pylori
The management of Pseudomonas and H. pylori infections, while involving very different antibiotics and clinical settings, shares a common thread: both require evidence-based antibiotic selection that accounts for local resistance patterns, both demand confirmation of treatment success (eradication for H. pylori; clinical/microbiological response for Pseudomonas), and both offer important lessons in antimicrobial stewardship — H. pylori because rising clarithromycin resistance is directly driven by the widespread use of macrolides for respiratory infections, and Pseudomonas because empirical broad-spectrum anti-pseudomonal therapy in non-Pseudomonas infections drives resistance without benefit.
Provided image
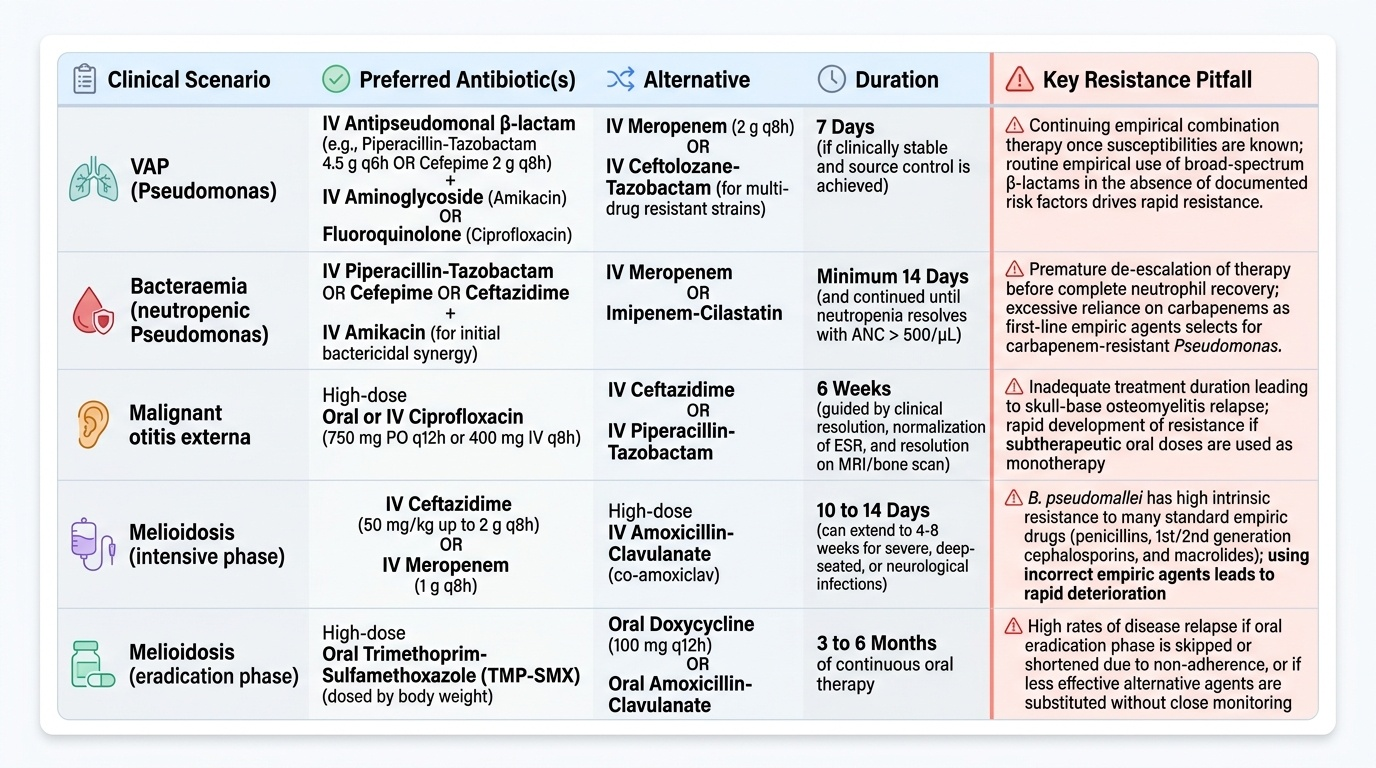
When to add Pseudomonas coverage in empirical therapy: The decision to include anti-pseudomonal cover in empirical regimens for hospital-acquired infections should be guided by specific risk factors, not routine practice. Risk factors for Pseudomonas infection: (a) prior Pseudomonas colonisation or infection; (b) structural lung disease (bronchiectasis, cystic fibrosis); (c) prolonged mechanical ventilation (>5 days); (d) prior broad-spectrum antibiotic use (>5 days) in the current admission; (e) neutropenia (ANC <500/µL); (f) severe burns (>25% TBSA); (g) central venous catheter in an immunocompromised patient. In patients without these risk factors, adding anti-pseudomonal beta-lactams (which have a broader-than-needed spectrum) drives resistance selection without clinical benefit.
Combination therapy for serious Pseudomonas infections: For life-threatening Pseudomonas bacteraemia or VAP, two-agent combination therapy (a beta-lactam + aminoglycoside OR a beta-lactam + fluoroquinolone) provides synergistic bactericidal activity and reduces the emergence of resistance. This is one of the few remaining evidence-supported indications for combination antibiotic therapy. However, once clinical improvement is established and susceptibility results are available, de-escalation to monotherapy is appropriate.
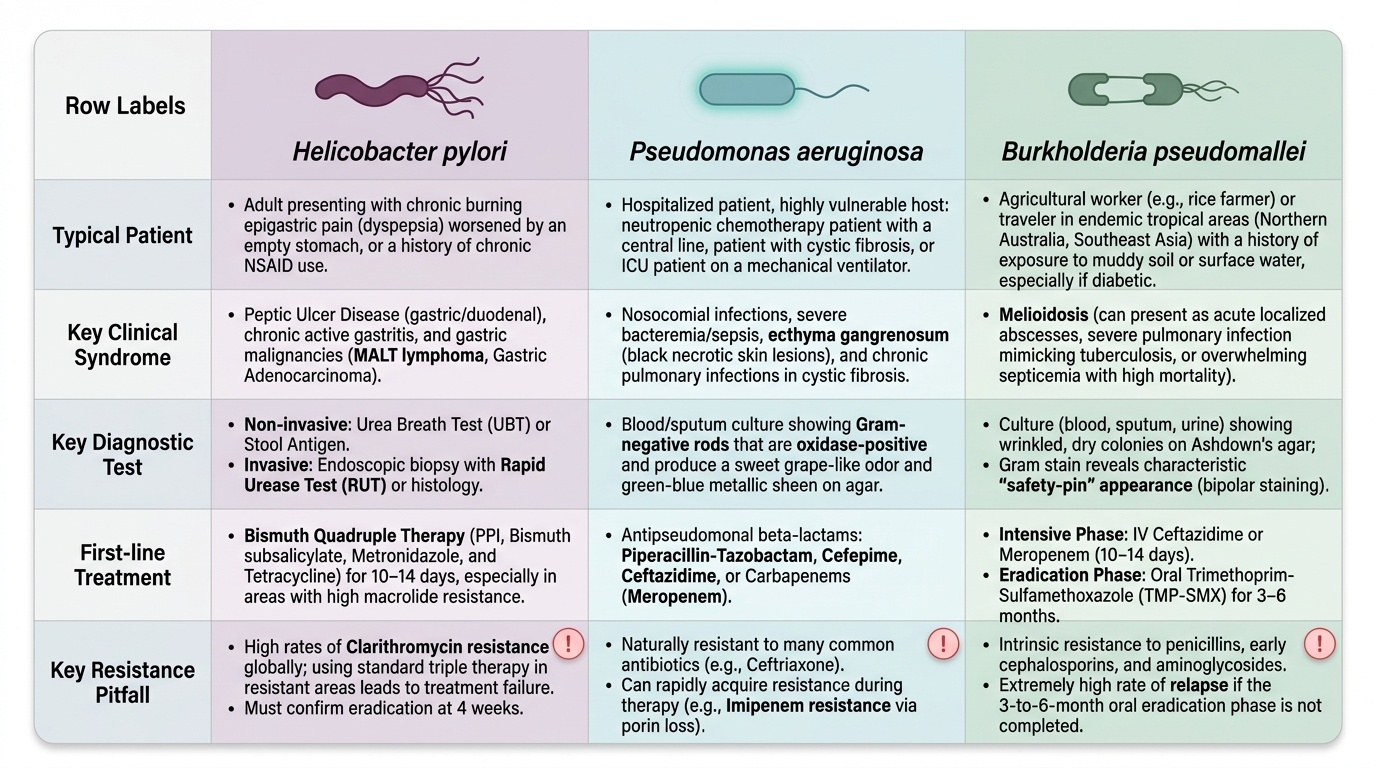
Confirming H. pylori eradication: Eradication must always be confirmed — it is not assumed from symptom resolution. UBT or stool antigen at ≥4 weeks post-treatment are the standard confirmatory tests. Serology should not be used for confirmation (remains positive after eradication for months to years). Failure to confirm eradication leaves the patient at risk of ulcer recurrence and gastric cancer progression. When eradication has failed, second-line therapy should use drugs different from the first-line regimen to avoid cross-resistance: if first-line was clarithromycin-based → use bismuth quadruple or levofloxacin triple; if first-line was bismuth quadruple → culture-guided therapy or levofloxacin triple.
NSAID co-prescribing and H. pylori: Patients who require long-term NSAID or aspirin therapy and are H. pylori-positive should receive H. pylori eradication AND PPI co-therapy — both interventions independently reduce ulcer risk, and their combination is superior to either alone. H. pylori eradication is the single most cost-effective intervention to prevent peptic ulcer disease on a population level.
Melioidosis in India — key stewardship point: Melioidosis is substantially underdiagnosed in India because clinicians and laboratories are not alert to B. pseudomallei. A febrile diabetic patient presenting with pneumonia, multiple organ abscesses, or an undiagnosed febrile illness in an endemic area (Northeast India, Odisha, coastal areas during monsoon) should have blood culture sent in two blood culture bottles specifically requesting incubation for slow-growing organisms. Misdiagnosis as pyogenic abscess and treatment with gentamicin (to which B. pseudomallei is intrinsically resistant) is a common and fatal error. IV ceftazidime or meropenem is the correct empirical choice in suspected melioidosis.
Self-Assessment: Gram-Negative Nonfermenter and H. pylori Infections
You have now covered the pathogenesis, clinical presentation, diagnostic approach, and management of H. pylori and Pseudomonas/Burkholderia infections. The scenarios below test the integration of these topics in clinical contexts — work through each case before reading the analysis.
Provided image
Scenario A: A 50-year-old woman is diagnosed with a low-grade gastric MALT lymphoma confined to the stomach (Stage IE) on endoscopic ultrasound. H. pylori rapid urease test is positive. She asks whether she needs chemotherapy.
Analysis: H. pylori-associated gastric MALT lymphoma Stage I responds to H. pylori eradication alone in 60–80% of cases — complete regression without chemotherapy or radiation. The treatment principle: H. pylori eradication removes the chronic antigenic stimulus that drives the B-cell lymphoma. Prescribe bismuth quadruple therapy (given high clarithromycin resistance likelihood); confirm eradication at 4 weeks; re-stage by repeat endoscopy with biopsies at 3 months post-eradication to assess regression. If the lymphoma persists or progresses after eradication, oncology referral for chemotherapy or radiation is indicated.
Scenario B: A 22-year-old male with acute leukaemia is on day 7 of induction chemotherapy. He develops fever (39.4°C), and blood culture at 16 hours shows Gram-negative rods, oxidase-positive. He has an existing central venous catheter. He is currently receiving cefepime empirically. The sensitivity shows: sensitive to ceftazidime, piperacillin-tazobactam, meropenem, amikacin, and ciprofloxacin; resistant to imipenem and ceftriaxone.
Analysis: Oxidase-positive Gram-negative rod in a neutropenic patient with a central line = Pseudomonas aeruginosa bacteraemia (ecthyma gangrenosum would confirm if present on skin). Imipenem resistance is likely mediated by OprD porin loss (the most common mechanism of imipenem resistance in Pseudomonas that leaves meropenem susceptible). Management: remove or change the central venous catheter (source control); switch to IV meropenem + IV amikacin (combination therapy for life-threatening Pseudomonas bacteraemia, to prevent emergence of resistance); de-escalate to meropenem monotherapy once clinical improvement established.
Scenario C: A 55-year-old diabetic male from Assam presents during monsoon season with 2 weeks of fever, weight loss, and right upper quadrant pain. CT abdomen shows multiple liver abscesses, right pleural effusion, and a lung cavity. Blood culture grows an oxidase-positive Gram-negative bacillus that is resistant to gentamicin. He was initially treated with gentamicin for 5 days without improvement.
Analysis: Multiple organ involvement (liver abscess + lung cavity + fever in a diabetic from Northeast India during monsoon) + oxidase-positive Gram-negative rod + gentamicin resistance = melioidosis (Burkholderia pseudomallei). Intrinsic gentamicin resistance is a diagnostic clue. Immediate treatment: IV ceftazidime 2g 8-hourly (or IV meropenem) for the intensive phase × 10–14 days, followed by oral TMP-SMX + doxycycline × 3–6 months for the eradication phase. Drainage of accessible abscesses. Notify the laboratory to confirm B. pseudomallei identification.
CLINICAL PEARL
Three high-yield pearls from this SDL: (1) H. pylori-positive MALT lymphoma Stage I is one of the few cancers where antibiotics are the first-line treatment — H. pylori eradication alone achieves remission in the majority of patients without chemotherapy. (2) Ecthyma gangrenosum — a necrotic black-eschar skin lesion in a neutropenic febrile patient — is pathognomonic of Pseudomonas bacteraemia and demands immediate anti-pseudomonal combination therapy. (3) Burkholderia pseudomallei is intrinsically resistant to gentamicin; in a febrile diabetic from endemic Northeast India with multiple organ abscesses who is not improving on gentamicin, melioidosis must be suspected — IV ceftazidime or meropenem is the correct choice.