Page 15 of 35
IM26.18-20 | Zoonotic Rickettsial and Filamentous Bacterial Infections — SDL Guide
Learning Objectives
- Describe the common causes, etiopathogenesis, clinical features, and management of bacterial zoonotic diseases: leptospirosis, brucellosis, plague, and anthrax
- Describe the pathogenesis, clinical features, and management of diseases caused by Actinomyces and Nocardia
- Describe the pathogenesis, clinical features, and management of rickettsial diseases, particularly scrub typhus, epidemic typhus, and endemic typhus
INSTRUCTIONS
This SDL covers three groups of infections that share a common epidemiological thread: they are all acquired from the environment, animal hosts, or arthropod vectors, and they are all significantly under-recognised in India. Leptospirosis, brucellosis, plague, anthrax, scrub typhus, and Actinomyces/Nocardia infections are each treatable with specific antibiotics but require clinical suspicion driven by the exposure history. A pattern-recognition approach — matching the exposure to the syndrome — is the key clinical skill.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 175 — Rickettsial Diseases; Ch. 167 — Leptospirosis; Ch. 168 — Brucellosis; Ch. 169 — Plague; Ch. 170 — Anthrax (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 13 — Infectious Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three presentations arrive in a busy general medicine clinic in Northeast India during the post-monsoon season. The first: a 34-year-old rice-field worker from Assam with 6 days of fever, severe myalgia, headache, jaundice, and oliguria — he worked barefoot in waterlogged fields last week. The second: a 28-year-old veterinarian with 3 weeks of undulating fever, profuse night sweats, and low back pain — he assisted with calving on a farm in Punjab. The third: a 52-year-old forest guard from Tamil Nadu presenting with fever, headache, and a painless black eschar at the right groin crease that he first noticed 5 days ago. These three patients have completely different infections — leptospirosis, brucellosis, and scrub typhus respectively — but they share the same diagnostic key: the occupational and exposure history. Without eliciting that history, all three look like 'fever with systemic features' and risk being treated with empirical broad-spectrum antibiotics that are wrong for all three. With the history, the diagnosis is made at the bedside before any test returns. This module builds the exposure-to-syndrome pattern that transforms these challenging diagnoses from missed to routine.
WHY THIS MATTERS
Zoonotic and rickettsial infections are among the most underdiagnosed causes of acute febrile illness in India, contributing to a substantial burden of mortality from delayed diagnosis and inappropriate treatment. Scrub typhus is now recognised as one of the most common causes of acute undifferentiated febrile illness in India, with large outbreaks documented in Tamil Nadu, Kashmir, Uttarakhand, Himachal Pradesh, and Northeast India. Leptospirosis is endemic in coastal and agricultural India, causing acute kidney injury, hepatic failure, and death in unrecognised cases. Brucellosis is prevalent wherever livestock farming is practised, yet frequently missed due to its non-specific presentation of undulating fever and musculoskeletal pain. Nocardia and Actinomyces cause indolent, chronic infections that mimic TB and malignancy, requiring specific long-course antibiotic therapy. Mastering the clinical patterns of these infections significantly reduces diagnostic delay and saves lives.
RECALL
Before proceeding, recall the relevant microbiology and epidemiology. Rickettsiae are obligate intracellular Gram-negative bacteria transmitted by arthropods (ticks, mites, lice, fleas) that infect endothelial cells, causing generalised vasculitis — the unifying pathological mechanism underlying all rickettsial diseases. Leptospira interrogans is a thin spirochaete that survives in the kidneys of reservoir animals (rats, dogs, cattle) and is shed in urine into water and moist soil. Brucella species are small Gram-negative coccobacilli that infect domestic animals (cattle, goats, sheep, pigs) and are transmitted to humans by direct contact with infected animals or their products (unpasteurised dairy, placental material). Bacillus anthracis forms heat-resistant spores that survive in soil for decades; Yersinia pestis (plague) is transmitted by flea bites from infected rodents. Actinomyces are filamentous Gram-positive bacteria that are normal oral flora; Nocardia are aerobic filamentous bacteria from soil.
Leptospirosis and Brucellosis: Clinical Presentation and Pathogenesis
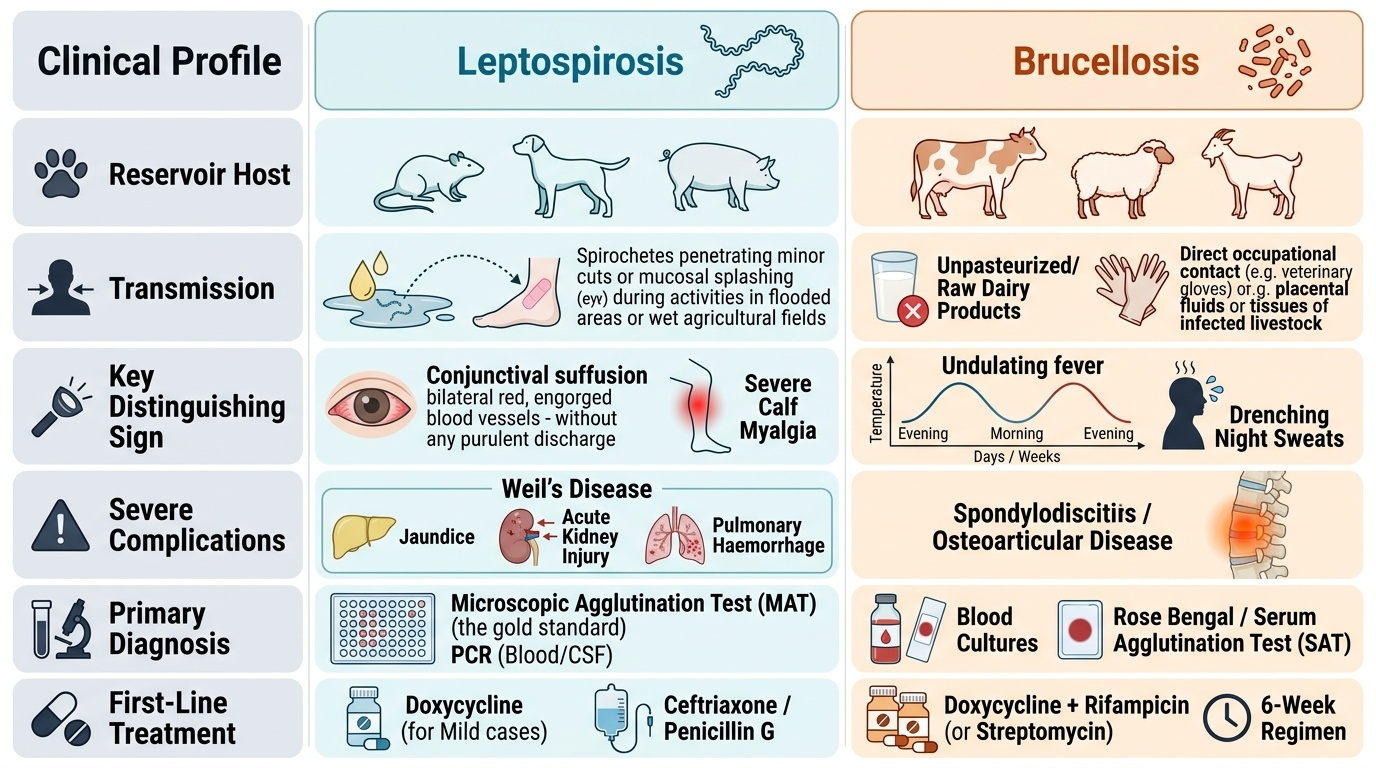
Leptospirosis is a systemic spirochaetal infection caused by Leptospira interrogans (pathogenic serovars), a thin, tightly coiled, aerobic spirochaete transmitted through skin or mucosal contact with water or soil contaminated by the urine of infected reservoir animals — primarily rats, dogs, cattle, and pigs. The spirochaetes penetrate intact mucous membranes and minor skin abrasions; they do not survive in dried or acid environments. In India, leptospirosis is endemic in coastal states (Kerala, Maharashtra, Gujarat, Tamil Nadu, Andaman Islands) and peaks in the post-monsoon season when flooding spreads infected rodent urine across agricultural fields and urban drain systems. Agricultural workers, sewer workers, veterinarians, and flood-affected populations are at highest risk.
Provided image
Pathogenesis: Leptospires spread haematogenously after entry, infecting the vascular endothelium of multiple organs. The key pathological mechanism is endothelial damage and generalised vasculitis — injury to capillary endothelium produces the multi-organ dysfunction characteristic of severe leptospirosis: acute kidney injury (tubular injury, direct leptospiral invasion of renal tubules), hepatocellular injury (jaundice, elevated transaminases), pulmonary haemorrhage (a feared complication), haemolysis, and uveitis (late complication).
Clinical phases: Leptospirosis follows a biphasic course in its classic (though not universal) presentation:
- Leptospiraemic phase (days 1–7): abrupt onset of fever (39–40°C), severe myalgia (especially calf muscles), headache, anorexia, nausea, and conjunctival suffusion (bilateral non-purulent conjunctival injection — one of the most discriminating signs of leptospirosis, reflecting the underlying vasculitis). The organism is detectable in blood and CSF during this phase. This phase resolves spontaneously in mild cases.
- Immune phase (days 7–14): in most patients, improvement occurs; in ~10–15%, the immune phase brings organ dysfunction — Weil's disease (the severe form): jaundice + acute kidney injury + haemorrhagic manifestations. AKI in Weil's disease is characteristically non-oliguric initially and responds well to aggressive IV fluids; in advanced cases dialysis may be required. Pulmonary haemorrhage syndrome (leptospirosis-associated pulmonary haemorrhage — LPHH) is the most feared complication — diffuse alveolar haemorrhage, respiratory failure, and mortality up to 50%; occurs independent of jaundice (can occur in anicteric severe disease).
- Anicteric leptospirosis: the majority (~90%) of cases — fever, myalgia, conjunctival suffusion, and leucocytosis, resolving without organ failure; easily missed or misdiagnosed as viral fever.
Diagnosis: LEPTO IgM ELISA is positive from day 5–7; MAT (Microscopic Agglutination Test) is the gold standard (titre ≥1:100 acute, or ≥4-fold rise in paired sera); blood culture in phase 1 (EMJH medium, incubated up to 6 weeks — impractical for acute management). CBC: leucocytosis with neutrophilia, thrombocytopenia, elevated CRP. LFTs: elevated transaminases (ALT, AST), markedly elevated bilirubin (conjugated). Creatinine elevated in renal involvement. Urinalysis: proteinuria, haematuria, casts.
Treatment: mild cases — oral doxycycline 100 mg twice daily × 7 days; severe (Weil's disease) — IV penicillin G 1.5 MU 6-hourly × 7 days or IV ceftriaxone 1g daily × 7 days (equivalent efficacy, preferred when penicillin allergy or if IV access is convenient); ICU support for AKI (fluid management, dialysis if needed), respiratory failure (mechanical ventilation for LPHH), thrombocytopenia. Prevention: doxycycline 200 mg orally once weekly is effective chemoprophylaxis for high-risk exposure (flood relief workers, military operations in endemic areas); validated post-exposure prophylaxis has not been established.
Brucellosis is a systemic infection caused by Brucella species — B. melitensis (goats, sheep — most virulent), B. abortus (cattle), B. suis (pigs), and B. canis (dogs). It is the most common bacterial zoonosis worldwide. In India, brucellosis is prevalent wherever livestock farming is practised — particularly in Rajasthan, Punjab, Haryana, Gujarat, and Uttar Pradesh — yet it is substantially underdiagnosed because of its non-specific presentation and limited laboratory awareness.
Pathogenesis: Brucellae are facultative intracellular bacteria that resist intracellular killing by macrophages; they survive within phagosomes by inhibiting phagosome–lysosome fusion and suppressing reactive oxygen species production. This intracellular survival drives the characteristic undulating fever (waves of fever separated by afebrile periods — reflecting episodic bacteraemia as organisms escape from macrophages) and allows the organism to disseminate to the reticuloendothelial system, bone marrow, liver, spleen, and joints.
Clinical features: Brucellosis is the classic 'undulating fever' — characterised by: fever that rises and falls in waves over days to weeks (undulating pattern), drenching night sweats (the most common symptom — reported in >90% of cases), profound fatigue and malaise, musculoskeletal complaints (arthralgia, back pain — lumbar spine involvement is the most common focal complication; sacroiliitis is characteristic), and hepatosplenomegaly. The 'maltese fever' description from the Mediterranean reflects the classical presentation in goat-herding populations. Focal complications: spondylodiscitis (disc space infection — most commonly at L4-L5, produces severe back pain and elevated ESR), epididymo-orchitis (unilateral painful testicular swelling — in up to 20% of male patients; an important differential for testicular torsion), neurobrucellosis (meningoencephalitis — rare but severe), endocarditis (rare but life-threatening).
Diagnosis: Serum agglutination test (SAT) — titre ≥1:160 or ≥4-fold rise between acute and convalescent sera; ELISA is more sensitive and now preferred; blood culture (gold standard — sensitivity 50–70% in first 2 weeks; BACTEC is preferred; laboratory must be notified of suspected Brucella — BSL-3 organism). Rose Bengal test (RBT) is a rapid bedside agglutination test — useful screening tool in resource-limited settings, high sensitivity but lower specificity. Bone marrow culture has the highest sensitivity (~90%) when blood cultures are negative.
Treatment: combination therapy is required to prevent relapse:
- Uncomplicated brucellosis: doxycycline 100 mg twice daily × 6 weeks + rifampicin 600–900 mg once daily × 6 weeks; OR doxycycline × 6 weeks + gentamicin 5 mg/kg daily IV × 7 days (preferred by WHO — lower relapse rate; the gentamicin course runs alongside the first 7 days of doxycycline).
- Spondylodiscitis: doxycycline + rifampicin + streptomycin triple therapy; extended course (3–6 months); neurosurgical input if cord compression.
- Brucellosis must NEVER be treated with a single antibiotic — monotherapy universally results in relapse.
Plague, Anthrax, Actinomyces, and Nocardia Infections
Plague is caused by Yersinia pestis, a Gram-negative coccobacillus transmitted by flea bites from infected rodents (rats, squirrels, prairie dogs). Y. pestis is one of the most lethal bacterial pathogens known to humans, responsible for the Black Death that killed an estimated 25–50 million people in 14th century Europe. Although plague is now rare globally due to improved sanitation and rodent control, India experienced the last major outbreak in Surat, Gujarat in 1994 (pneumonic plague), and small sporadic cases continue to be reported from Himachal Pradesh and other states. Plague is a notifiable disease and a potential bioterrorism threat; it must be on the differential for any patient presenting with acute febrile lymphadenopathy following rodent exposure in India or in travellers from endemic areas (Central Asia, Africa, South America). Early recognition and prompt treatment are critical, since mortality approaches 100% without specific antibiotics.
Three clinical forms of plague:
- Bubonic plague (most common — 80–90%): transmitted by flea bite. The classic presentation is an acutely ill, febrile patient with an intensely painful, swollen lymph node cluster (bubo) in the inguinal, axillary, or cervical region (corresponding to the drainage region of the bite site). The bubo can be so painful that the patient holds the affected limb immobile. Bacteraemia follows; without treatment, secondary pneumonic plague can develop. Diagnosis: Gram stain and culture of bubo aspirate (safety precaution — notify the laboratory); FA staining of material; serology.
- Pneumonic plague: acquired by inhalation of respiratory droplets from a patient with plague pneumonia (secondary) or directly from animal reservoir (primary). Extremely contagious — requires airborne precautions. Presents as rapidly progressive pneumonia with haemoptysis; virtually 100% fatal without treatment within 24 hours of respiratory symptoms.
- Septicaemic plague: overwhelming bacteraemia, disseminated intravascular coagulation, and haemorrhagic necrosis of extremities (historically giving rise to the 'Black Death' name — purpuric skin necrosis).
Treatment: streptomycin (historical gold standard — 15 mg/kg IM twice daily × 10 days) or gentamicin 5 mg/kg IV daily × 10 days (now preferred). Alternatives: doxycycline 100 mg twice daily × 10 days, ciprofloxacin. Post-exposure prophylaxis for contacts: doxycycline or ciprofloxacin × 7 days. Isolation: standard precautions for bubonic; droplet + airborne for pneumonic plague.
Anthrax is caused by Bacillus anthracis, a spore-forming Gram-positive bacillus found in soil and in livestock (cattle, goats, sheep). Anthrax is an important bioterrorism agent (aerosolised spores used as a weapon — inhalation anthrax with near-100% mortality if untreated). In India, anthrax cases occur in agricultural states where cattle handling is common.
Three clinical forms of anthrax:
- Cutaneous anthrax (most common — >95%): a painless black eschar (malignant pustule) at the site of skin contact with spore-contaminated material; surrounded by marked non-pitting oedema; fever; regional lymphadenopathy. The key distinguishing feature: painless (unlike infected wounds or necrotising fasciitis, which are painful). Treatment: oral ciprofloxacin or doxycycline × 7 days; 10% mortality if untreated, <1% with treatment.
- Inhalation anthrax: mediastinal widening on CXR (from haemorrhagic mediastinal lymphadenopathy — Woolsorter's disease); biphasic illness: initial flu-like prodrome → abrupt deterioration with respiratory failure, mediastinitis, haemorrhagic meningitis; mortality >80% despite treatment.
- GI anthrax: from ingestion of undercooked meat from infected animals; oropharyngeal or intestinal ulcers; rare in India.
Treatment: ciprofloxacin 400 mg IV 12-hourly (first-line for inhalation and severe cutaneous, given B. anthracis natural susceptibility to fluoroquinolones) + raxibacumab (antitoxin, where available). Duration: 60 days (inhalation anthrax — because spores can remain dormant in lungs for weeks).
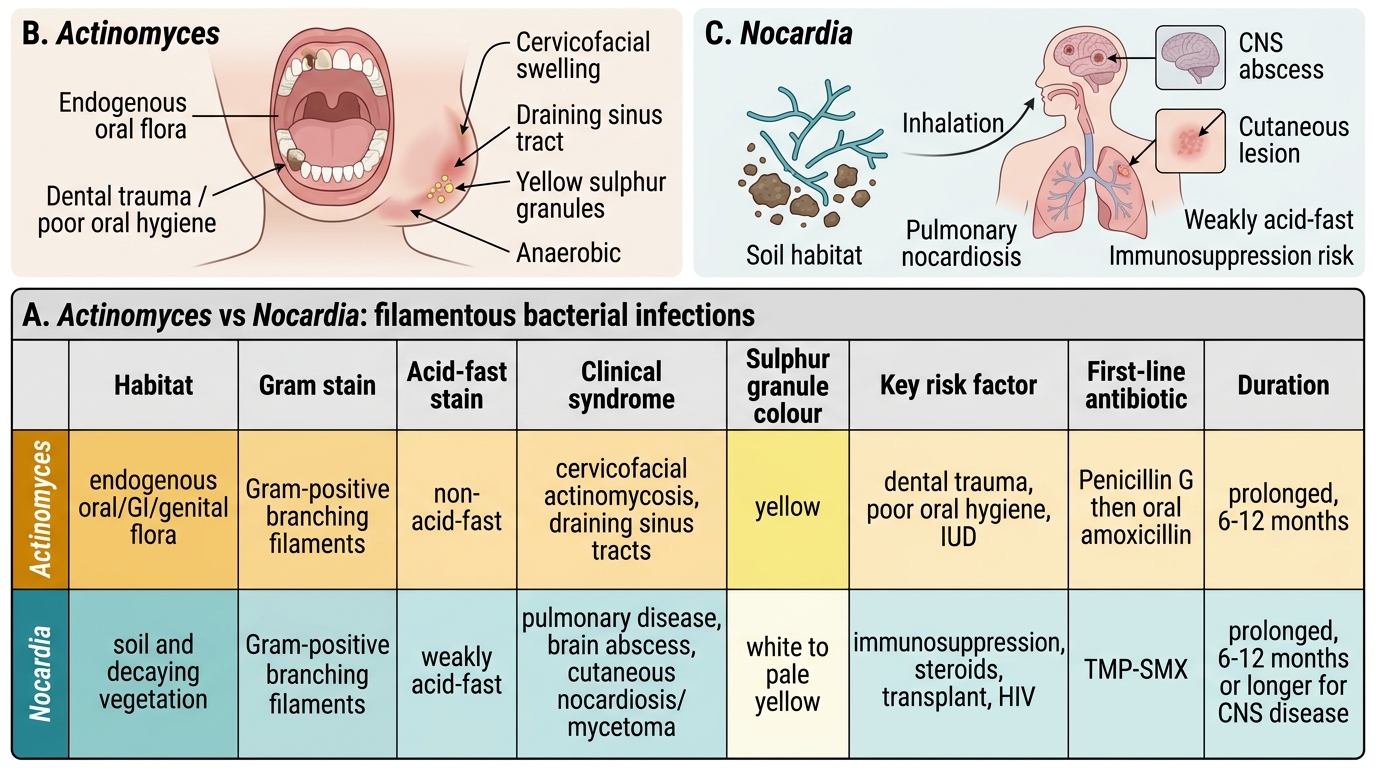
Actinomyces and Nocardia infections are caused by filamentous bacteria that produce indolent, chronic, suppurative infections mimicking TB or malignancy. Both are important differentials in the immunocompromised patient.
Actinomycosis: caused by Actinomyces israelii and related species — anaerobic or microaerophilic, Gram-positive filamentous bacteria that are normal oral flora. Actinomycosis is not a true zoonosis — it is an endogenous infection triggered by mucosal disruption (dental extraction, jaw trauma, aspiration, abdominal surgery). Three classic forms: (a) cervicofacial (jaw) — the most common (55%): indolent, indurated, painless jaw/neck mass with multiple draining sinuses producing sulphur granules (yellow macroscopic aggregates of bacterial filaments — pathognomonic); (b) thoracic — lung/pleural mass, often mistaken for carcinoma or TB; crosses tissue planes, extending to chest wall; (c) abdominal/pelvic — post-appendicectomy or post-IUD insertion; pelvic mass extending to adjacent organs. Diagnosis: culture and histology of sulphur granules (Gram stain: Gram-positive branching filaments). Treatment: high-dose penicillin IV (benzylpenicillin 18–24 million units/day) × 4–6 weeks, followed by oral amoxicillin × 6–12 months — long courses are required because of poor antibiotic penetration into the indurated fibrous mass.
Nocardiosis: caused by Nocardia asteroides and related species — aerobic filamentous bacteria found in soil. Unlike Actinomyces, Nocardia is an exogenous infection acquired by inhalation or skin inoculation. It is a significant opportunistic infection in immunocompromised patients: organ transplant recipients (calcineurin inhibitors predispose), HIV with CD4 <200, long-term corticosteroid users, and patients with chronic granulomatous disease. Primary pulmonary nocardiosis (most common): productive cough, fever, weight loss, cavitating lung infiltrates — mimicking TB closely. Brain abscess occurs in 25% of disseminated nocardiosis. Cutaneous nocardiosis: skin nodules, mycetoma (Madura foot — chronic swelling of the foot with multiple draining sinuses; white/yellow granules). Diagnosis: Gram stain (Gram-positive branching filaments, weakly acid-fast — modified ZN stain, important distinguishing feature from Actinomyces which is not acid-fast). Culture on blood agar (slow growing — 3–7 days). Treatment: TMP-SMX (co-trimoxazole) is first-line for most forms; for CNS/disseminated nocardiosis: IV imipenem + amikacin + TMP-SMX triple therapy × 4–6 weeks then step-down to TMP-SMX for 6–12 months. Duration is long to prevent relapse.
Actinomyces vs Nocardia: Filamentous Bacterial Infections
SELF-CHECK
A 40-year-old farmer from Punjab develops 3 weeks of undulating fever, drenching night sweats, and severe low back pain. He is the primary caretaker for a herd of cattle that recently had several spontaneous abortions. ESR is 85 mm/hr. The MOST appropriate initial diagnostic test is:
A. Widal test — undulating fever in India should first prompt investigation for enteric fever
B. Blood culture (BACTEC system) + Rose Bengal plate test / serum agglutination test (SAT) for Brucella
C. Sputum AFB smear and culture — low back pain with fever suggests spinal tuberculosis
D. LEPTO IgM ELISA — cattle exposure and fever suggests leptospirosis
Reveal Answer
Answer: B. Blood culture (BACTEC system) + Rose Bengal plate test / serum agglutination test (SAT) for Brucella
The clinical triad of undulating fever + night sweats + low back pain (sacroiliitis) in a cattle farmer with recent cattle abortions is highly characteristic of brucellosis. Cattle spontaneous abortion (brucellosis-related) is a key epidemiological clue. Blood culture (BACTEC is preferred — incubate for 3 weeks) has 50–70% sensitivity in the first 2 weeks; Rose Bengal test or SAT is a rapid sensitive screening test. Widal test is for Salmonella typhi (enteric fever does not cause spinal pain or undulating fever). AFB smear is appropriate for TB, but the exposure history here strongly points to Brucella. Leptospirosis causes acute illness with conjunctival suffusion and AKI — not a 3-week undulating course.
Rickettsial Diseases: Scrub Typhus, Epidemic Typhus, and Endemic Typhus
Rickettsial diseases are caused by obligate intracellular, Gram-negative bacteria belonging to the genera Rickettsia, Orientia, and Anaplasma, all transmitted by arthropod vectors (ticks, mites, lice, fleas). They share a common pathological mechanism: endothelial cell invasion → endothelial injury → generalised vasculitis affecting multiple organs simultaneously — producing fever, rash (where present), and multi-organ dysfunction. In India, rickettsial diseases — particularly scrub typhus — are now recognised as a major cause of acute undifferentiated febrile illness and have been identified as one of the most underdiagnosed infections in the subcontinent. Misdiagnosis as typhoid or viral fever, and inappropriate treatment, leads to preventable deaths.
Provided image
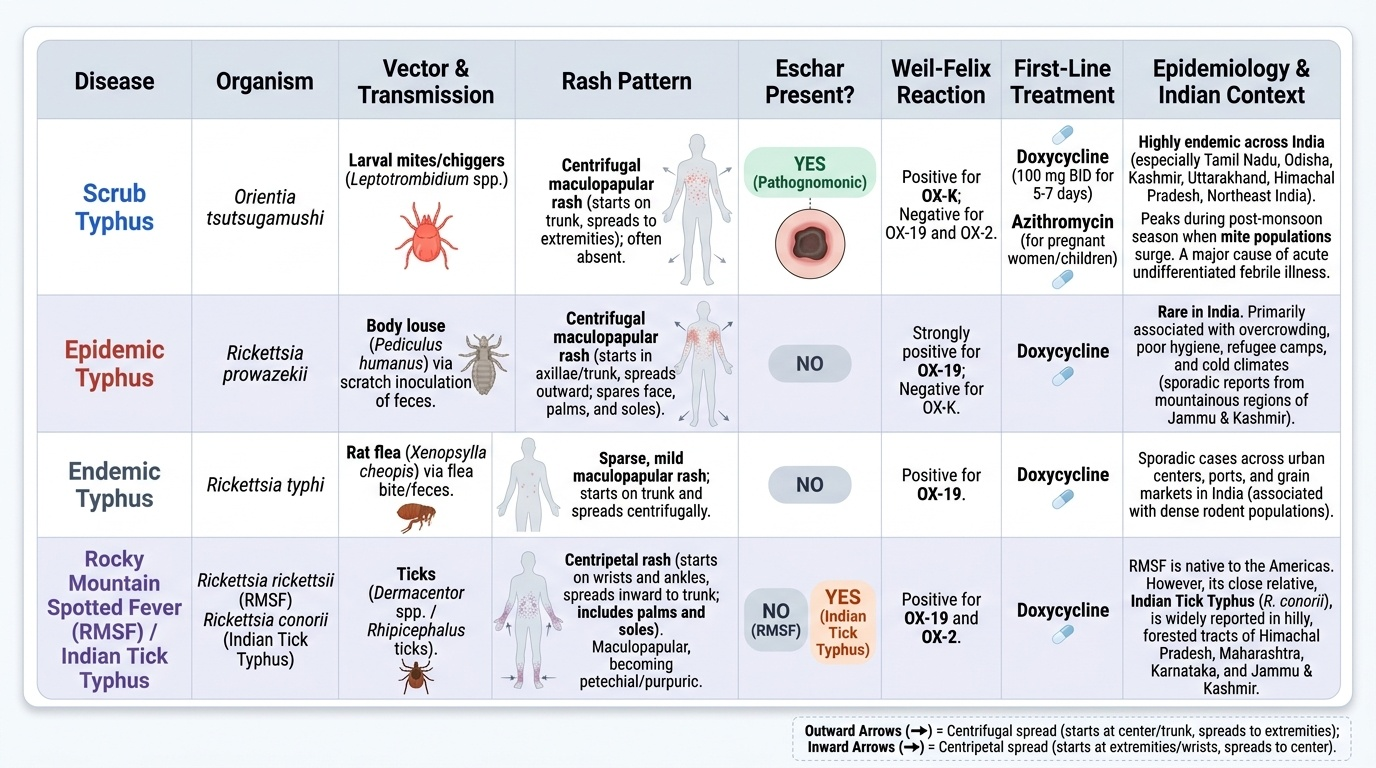
Scrub typhus is caused by Orientia tsutsugamushi, transmitted by the bite of larval mites (chiggers) of the genus Leptotrombidium. The chigger bite site leaves a characteristic eschar — a painless necrotic lesion with a black crust and surrounding erythema — which, if found, is pathognomonic. Endemic across the 'tsutsugamushi triangle': South Asia (India — particularly Tamil Nadu, Odisha, Kashmir, Uttarakhand, Himachal Pradesh, Northeast India), Southeast Asia, and the Pacific. In India, it peaks during the post-monsoon season when mite populations are highest. The organism has an extraordinary antigenic diversity (11 serotypes with limited cross-immunity), explaining why repeat infection is possible.
Clinical features of scrub typhus:
- Incubation period: 6–21 days after the chigger bite
- Fever (abrupt onset, 39–41°C), severe headache, myalgia, and malaise
- Eschar: present in 30–70% of patients depending on the population and diligence of examination; most commonly found in moist, concealed skin folds — the groin, axillae, behind the ears, the scalp hairline, the popliteal fossa, and the belt line. Clinical examination must include all these sites explicitly.
- Generalised maculopapular rash: appears in week 2 (less common in Indian patients than in Asian populations — present in ~20–40%); trunk → peripheries
- Relative bradycardia (lower heart rate than expected for the degree of fever)
- Complications (in severe/untreated cases): encephalitis (altered consciousness, seizures), myocarditis, acute respiratory distress syndrome (ARDS), acute kidney injury, hepatitis, and haemorrhagic fever
Diagnosis: Scrub typhus IgM ELISA is the standard test (sensitivity 90–95% after day 7 of illness); IFA (immunofluorescence assay) is the gold standard reference test; Weil-Felix test (Proteus OXK agglutination) — historically used in India but insensitive (40–60%) and non-specific; no longer recommended. PCR on eschar swab or blood provides early diagnosis before serology is positive.
Treatment: doxycycline 100 mg twice daily × 7 days is dramatically effective — patients typically defervesce within 24–48 hours of starting doxycycline (failure to respond is itself a diagnostic clue suggesting an alternative diagnosis). Alternative for pregnant women and children <8 years: azithromycin 500 mg daily × 3 days (proven efficacy in Indian paediatric scrub typhus). Important: chloramphenicol was historically used but achieves only bacteriostasis (not bactericidal) and is associated with higher relapse and mortality rates than doxycycline; it is no longer preferred.
Epidemic typhus is caused by Rickettsia prowazekii, transmitted by the human body louse (Pediculus humanus corporis). It is classically associated with war, famine, displacement, and crowded unsanitary conditions — the organism is shed in louse faeces, which are scratched into the bite site or inhaled. Now rare in India but can occur in marginalised populations. Clinical features: severe febrile illness with severe headache, macular rash (trunk → extremities, characteristically sparing the face, palms, and soles), confusion, and multi-organ failure. A distinctive feature: Brill-Zinsser disease — recrudescent typhus occurring years after primary infection, caused by R. prowazekii reactivation from latency; clinically similar to epidemic typhus but milder. Treatment: doxycycline 100 mg twice daily × 7 days.
Endemic typhus (murine typhus) is caused by Rickettsia typhi, transmitted by rat fleas (Xenopsylla cheopis). Worldwide distribution; in India associated with urban rat-infested environments. Clinically milder than epidemic typhus: fever, headache, maculopapular rash (trunk → extremities — same pattern as epidemic typhus but milder, may be absent). Weil-Felix: OX-19 positive (distinguishing from scrub typhus which is OX-K positive, though Weil-Felix is no longer recommended). Treatment: doxycycline × 7 days.
Rocky Mountain Spotted Fever (RMSF) — caused by Rickettsia rickettsii; not endemic in India but important to know for travellers returning from the Americas. Distinctive feature: rash begins on the wrists and ankles (distal extremities) and spreads centripetally — the REVERSE of epidemic/endemic typhus. Petechial/purpuric rash involving the palms and soles is characteristic. Treatment: doxycycline; delay kills — do not await serology before starting treatment.
SELF-CHECK
A 30-year-old forest worker from Tamil Nadu presents with 8 days of fever (40°C), severe headache, and a painless black lesion at the right groin. Weil-Felix OX-K titre is 1:640. He is started on doxycycline 100 mg twice daily. After 36 hours, his fever resolves and he feels significantly better. Which statement about this case is CORRECT?
A. The Weil-Felix OX-K positivity is sufficient to confirm scrub typhus without further testing
B. Rapid defervescence within 24–48 hours of doxycycline is a characteristic feature of scrub typhus and supports the clinical diagnosis
C. The lesion at the groin is likely ecthyma gangrenosum from Pseudomonas, not an eschar
D. Chloramphenicol should be added because doxycycline alone has insufficient efficacy for scrub typhus
Reveal Answer
Answer: B. Rapid defervescence within 24–48 hours of doxycycline is a characteristic feature of scrub typhus and supports the clinical diagnosis
The rapid clinical response to doxycycline — defervescence within 24–48 hours — is a highly characteristic feature of scrub typhus (and all rickettsial diseases) and strongly supports the clinical diagnosis. It is considered a therapeutic 'doxycycline test.' The painless black eschar at the groin in a forest worker from Tamil Nadu with OX-K positivity further supports scrub typhus. Note: Weil-Felix OX-K titre ≥1:320 is suggestive of scrub typhus, but the IgM ELISA is the preferred confirmatory test. Weil-Felix alone is insufficient for definitive diagnosis (insensitive, non-specific) — IgM ELISA should also be ordered. Ecthyma gangrenosum is a Pseudomonas skin lesion in neutropenic patients — the clinical context here is entirely different. Chloramphenicol is NOT preferred over doxycycline for scrub typhus.