Page 3 of 18
IM27.{1-4,12} | Tuberculosis Foundations — SDL Guide (Part 3)
Principles of Prevention and Programme Response
The management of tuberculosis at a population level requires the same rigour and precision as management at the individual level. For the foundations SDL, arc step 4 addresses the preventive and programmatic management principles that flow directly from the epidemiology, pathogenesis, and resistance science covered in the preceding blocks. These principles — TB preventive therapy, infection control, contact tracing, and the NTEP operational framework — are the applied translation of foundational science into public health action and are tested directly in clinical practice when managing household contacts, screening high-risk populations, and advising patients on isolation precautions.
TB preventive therapy (TPT): Individuals with latent TB infection (LTBI) at high risk of progression to active disease should receive TPT to prevent that conversion. NTEP-recommended regimens include: (1) 6H — isoniazid 5 mg/kg (maximum 300 mg) daily for 6 months; (2) 3HP — weekly isoniazid + rifapentine for 3 months (preferred where available for better adherence). TPT is mandatory for: all HIV-positive individuals after ruling out active TB; all children aged <5 years who are household contacts of smear-positive cases; patients starting TNF-α blockers or other immunosuppressants after LTBI is confirmed; and other high-risk groups per current NTEP guidelines. Contraindication: active TB must be excluded before TPT — an inadvertent course of isoniazid monotherapy in active TB would amplify resistance.
Infection control principles: In health facilities, TB infection control is a three-tier hierarchy — administrative (separating infectious from non-infectious patients, fast-tracking suspects, reducing patient dwell time), environmental (natural and mechanical ventilation to dilute droplet nuclei concentration — the single most effective physical control measure), and personal protective equipment (N95 respirators for healthcare workers in high-exposure settings — surgical masks are NOT equivalent as they do not filter 1–5 μm particles). In the home, while full respiratory isolation is impractical, key measures include: sleeping separately, opening windows for natural ventilation, and ensuring the patient covers the mouth when coughing. Once on effective treatment, sputum conversion to smear-negative usually occurs within 2 weeks for drug-sensitive TB — after which the patient is essentially non-infectious while completing the regimen.
Contact tracing and screening: All household and close contacts of smear-positive index cases must be screened systematically. The NTEP protocol requires: symptom screening of all contacts; Mantoux/TST testing of children <5 years; HIV testing of contacts with risk factors; clinical evaluation and CXR for symptomatic contacts. Contacts found to have active TB are started on treatment; asymptomatic LTBI contacts in high-risk groups (children <5, HIV-positive) receive TPT regardless of TST result.
NTEP operational framework for treatment: The current NTEP framework mandates: (1) upfront CBNAAT/NAAT testing for ALL presumptive TB cases before treatment; (2) daily FDC-based regimens — the drug-sensitive regimen is 2HRZE/4HRE (intensified in the tb-treatment SDL); (3) Nikshay notification within 24 hours of diagnosis for all patients in public and private sectors; (4) Ni-kshay Poshan Yojana nutritional support automatically triggered on notification; (5) treatment support through trained treatment supporters or video-observed treatment (VOT) where available; (6) treatment outcome monitoring at defined intervals — sputum conversion at 2 months, end-of-treatment.
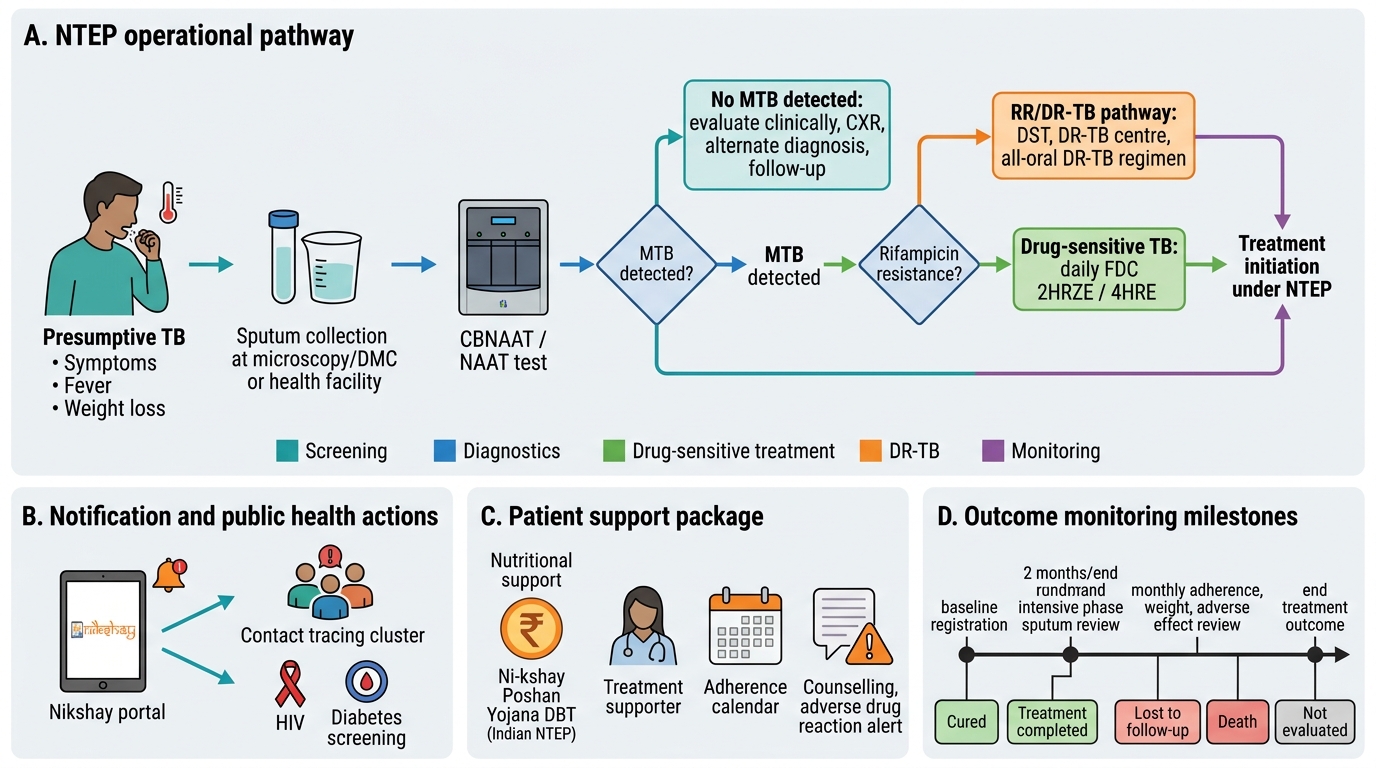
NTEP Pathway From Presumptive TB to Treatment Outcome
Self-Assessment: Integrating TB Foundations
At this stage you should be able to integrate all five foundational TB competencies into a coherent clinical framework. The following scenarios and reflection prompts are designed to test whether the pieces connect — not just whether each fact was memorised in isolation. TB medicine in India is distinctive in its epidemiological context, the NTEP infrastructure, and the dual-epidemic pressures from HIV and diabetes. A clinician who understands these foundations approaches every patient with cough, weight loss, or unexplained fever through an active TB lens.
Scenario A — Epidemiology applied: A 28-year-old male construction worker from UP presents with 6 weeks of cough and fever. He shares a dormitory with 12 co-workers. His employer has not tested any contacts. How many co-workers are statistically at risk of having been infected if the index patient is smear-positive and symptomatic for 6 weeks?
Analysis: A smear-positive TB patient with active symptoms can infect on average 10–15 contacts per year if in close indoor contact. In a dormitory setting (poor ventilation, prolonged shared air space), the infection probability is higher than the general household attack rate of 5–10%. However, infection rate differs from disease rate — of those infected, only ~10% will develop disease in their lifetime. The programmatic response: all 12 contacts require TST/IGRA testing and clinical screening under NTEP contact-tracing guidelines; contacts aged <5 years and HIV-positive contacts require particular urgency.
Scenario B — Pathogenesis applied to atypical presentation: A 38-year-old woman with HIV (CD4 count 85 cells/μL) is admitted with fever, headache, and confusion. Chest X-ray shows bilateral diffuse small nodular infiltrates. Sputum smear is negative. What form of TB does the radiology suggest, and why is the smear negative despite active disease?
Analysis: Bilateral diffuse 1–2 mm nodules = miliary TB — haematogenous dissemination. In severe HIV immunosuppression (CD4 <200 cells/μL), the granuloma cannot form adequately, so bacilli disseminate without containment. Smear negativity in miliary TB reflects the pattern of disease: bacilli are in the bloodstream and disseminated tissue rather than concentrated in airways — fewer bacilli per millilitre of sputum. This patient requires blood culture for M. tuberculosis, urine AFB culture, and if meningeal signs are present, lumbar puncture for CSF analysis. Management: initiate 4-drug TB regimen and ART within 2–8 weeks (8 weeks if CNS involvement confirmed).
Scenario C — Drug resistance reasoning: A TB patient reports he took "some TB tablets" for 2 months before stopping when he felt better, then resumed treatment 3 months later when symptoms recurred. His current sputum is CBNAAT (Xpert MTB/RIF) positive and shows rifampicin resistance. What is the most likely mechanism of this resistance, and what should NOT be done?
Analysis: This patient has acquired rifampicin resistance from treatment interruption — inadequate treatment duration allowed selection of pre-existing rpoB mutants. He now has RR-TB/MDR-TB. The critical rule: never add a single new drug to this patient's existing regimen (would add one drug to virtual monotherapy, selecting a doubly resistant strain). He requires full DST for second-line drugs, and should be placed on the NTEP MDR-TB regimen under supervision.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
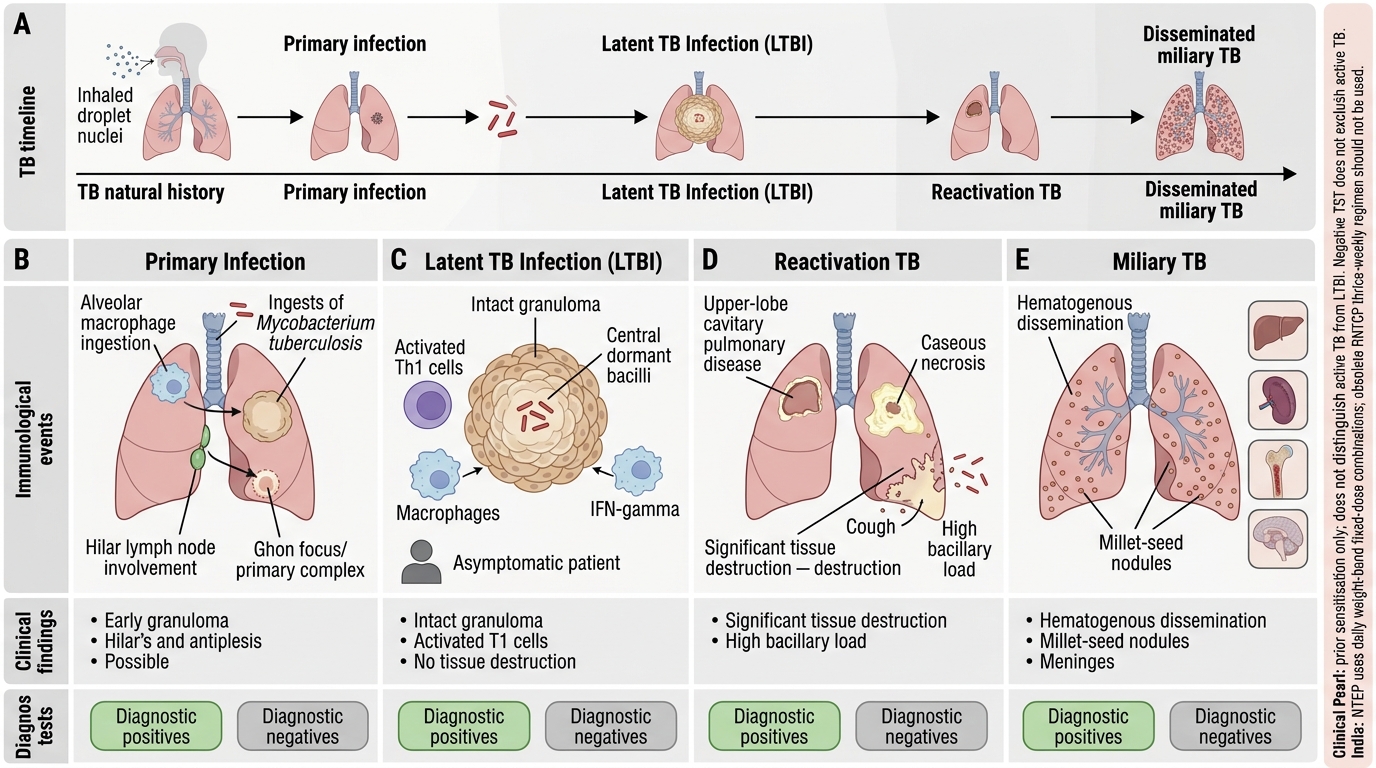
Natural History of Tuberculosis: Stages, Immunology, and Diagnosis
CLINICAL PEARL
The single most important clinical principle for TB management in India is the distinction between the NTEP (National Tuberculosis Elimination Programme) and the obsolete RNTCP. The programme was renamed in 2020 to reflect the elimination target. More importantly, the treatment regimen changed fundamentally: India abandoned the thrice-weekly intermittent regimen under RNTCP and moved to a daily, weight-band-dosed, fixed-dose combination (FDC) regimen under NTEP. Any citation of the old thrice-weekly schedule in a clinical setting is not just out of date — it represents a prescribing error that may contribute to treatment failure. Every TB prescription must now be daily, using FDCs, with doses adjusted to the patient's weight band (as published in the current NTEP Technical and Operational Guidelines). Smear-positive status still matters for initial categorisation but has been partially superseded by molecular (CBNAAT) results under the new diagnostic algorithm.
A second pearl: the TST (Mantoux test) does NOT distinguish active TB from LTBI — it only indicates prior sensitisation. A positive Mantoux in an asymptomatic contact with a normal chest X-ray = LTBI. A negative Mantoux does NOT exclude active TB — especially in malnourished patients, HIV-positive patients (CD4 <200), or children with miliary TB, where anergy from severe immune suppression gives a false-negative result.